👉 We spend decades arguing about how low to push LDL-C
👆 Almost no one asks the obvious question:
🤔 How much LDL-C did our ancestors actually have?
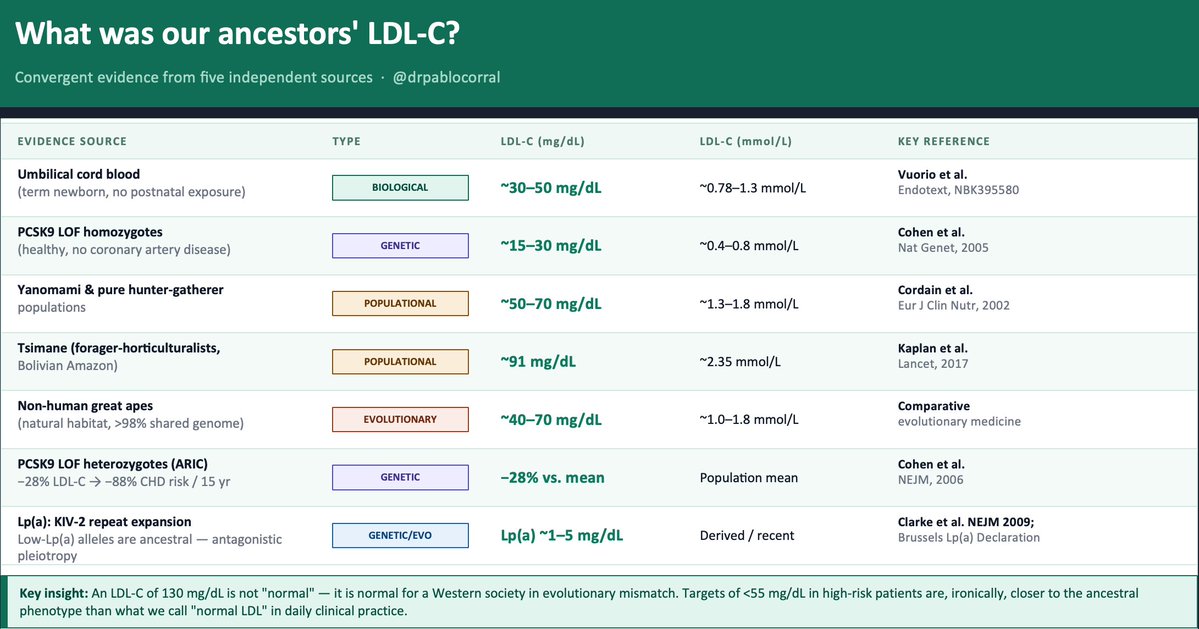
The evidence exists — five independent lines, all converging on the same uncomfortable answer.
1️⃣ The term newborn. Before any dietary or metabolic influence, a healthy neonate arrives with LDL-C of ~30–50 mg/dL. That is the LDLR operating without environmental interference. Everything that rises after birth is acquired.
2️⃣ The Tsimane (Kaplan et al., Lancet 2017) — forager-horticulturalists of the Bolivian Amazon — have a LDL-C between 70 to 90 mg/dL and the lowest prevalence of coronary atherosclerosis ever recorded in any human population. Five times less than the U.S. in adults over 75. And their LDL is rising as roads and processed food arrive.
3️⃣ PCSK9 loss-of-function variants. African American carriers of nonsense mutations (Y142X/C679X, ~2% frequency): −28% LDL-C and −88% CHD risk over 15 years (Cohen et al., NEJM 2006). Homozygous LOF carriers live with LDL-C of ~15–30 mg/dL. Perfectly healthy. Nature already ran the trial.
4️⃣ Evolutionary genetics. Recent positive selection signals exist on gain-of-function PCSK9 variants that raise LDL-C — likely adaptive in food-scarce ancestral environments. Modern hypercholesterolemia is not "normal." It is an ancestral survival advantage turned pathological by evolutionary mismatch.
5️⃣ Great apes in natural habitat: ~40–70 mg/dL LDL-C. Same genome. Different environment.
👆 Bonus — Lp(a). The KIV-2 repeat expansion that raises Lp(a) is a derived, recent variant. Low-Lp(a) alleles are ancestral. Elevated Lp(a) is a textbook antagonistic pleiotropy signal — possibly protective against bleeding early in life, atherogenic over decades
📍The convergent estimate: ancestral LDL-C was ~30–70 mg/dL.
📍An LDL-C of 130 mg/dL is not "normal." It is normal for a Western society in evolutionary mismatch. Targets of <55 mg/dL in high-risk patients — which still feel aggressive to many clinicians — are, ironically, closer to the ancestral phenotype than what we call "normal LDL" in daily practice.
🤔 The question is not "is it safe to lower LDL this much?"
The question is: why did we let it rise this high?
@society_eas@nationallipid
The cholesterol wars are over.
LDL won.
New guidelines. Four landmark trials. An oral PCSK9 inhibitor that matches injectables. And data proving we should be treating patients we currently aren't.
Here's everything clinicians need to know. 🧵
@Drlipid It looks like there is a typo in the upper left green bar text. I was expecting “< 75 nmol/L” instead of “< 50 nmol/L”.
Thank you for your important postings spreading awareness on lipid health and the excellent content you publish to help establish the facts.
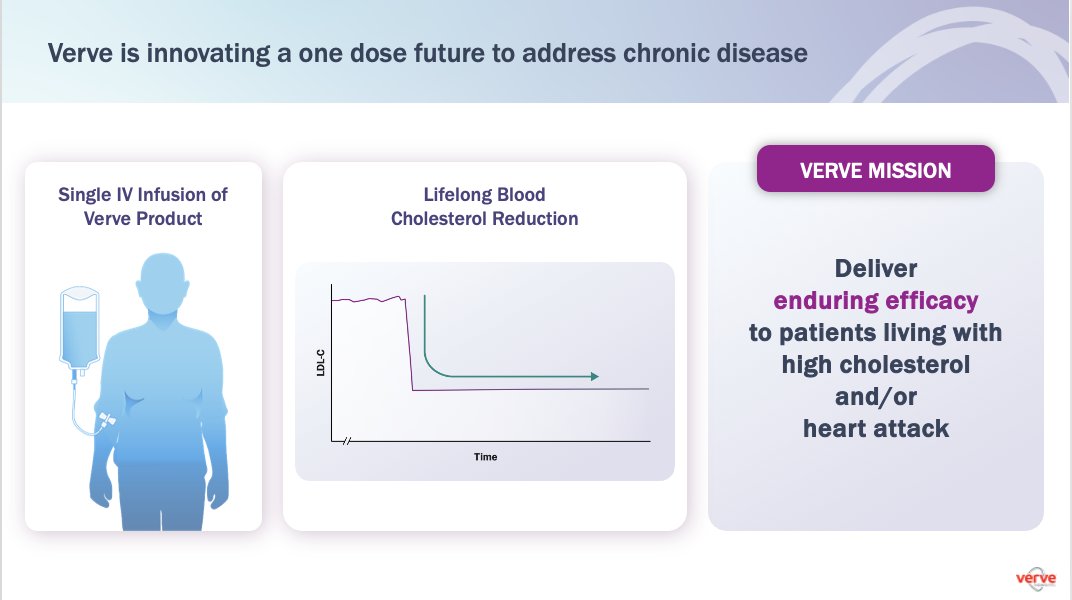
@VerveTx team is thrilled today to present initial data from the Heart-2 Phase 1b clinical trial of VERVE-102, an in vivo base editing investigational medicine targeting PCSK9
And the emerging product profile of VERVE-102 (for patients receiving ≥50mg total RNA dose):
a. A single IV infusion with *excellent* safety leading to
b. mean LDL-C reduction of 59%
c. a max of 69% so far
d. and consistent LDL-C reductions, with each patient getting >50%
e. and durability of reduction for the base editing mechanism out to 2 years plus (and probably lifelong)
🙏🏾
f. If this profile holds as we move through clinical development, this is going to be a remarkable new Rx option for the millions of patients living with high cholesterol or heart attack
and
suggests that a one-dose future for this chronic disease should be possible
Conference call webcast at 8AM ET here: https://t.co/ivO7gp6AOE
Additional slides to come at 9A
$VERV
Press release here: https://t.co/8qOSJcrcLY
I very much agree with the antagonist on this debate. Outside of Familial Dysbetalipoproteinemia TG-related CV risk is driven by apoB. Lowering TG is of secondary importance and there is no established concentration which can serve as a goal -
Do you really want to understand the Lipid Hypothesis? The following magnificent, incredibly enjoyable 5-part totally inclusive series written by David Steinberg in the Journal Of Lipid Research (open access) has long been forgotten. It was so important on my lipiddology learning curve. I consider it mandatory reading for any lipidologist, any clinician or person really interested in the evolution of the Lipid Hypothesis and Atherosclerosis. Of course, the deniers will not look at it. This treatise is a Thematic review series: the pathogenesis of atherosclerosis. An interpretive history of the cholesterol controversy: part I - https://t.co/MBFMDpkr44 Part II https://t.co/NCLSGSYSEc Part III https://t.co/ceOX4oByod Part IV https://t.co/fpfi2q12FH Part V https://t.co/ICru1muaFw @nationallipid@society_eas
The @NEJM is getting serious about covering #AI in medicine with a new series and journal. A #GPT4 preview, review and editorial today
This important advance is covered in-depth in a new book
https://t.co/hGyrJt4yt7
Looking for an internship in quantum computing? Check out what our amazing interns did this year at Bleximo and join us next summer!
https://t.co/SALg1VMGsn
Join Scott Aaronson and Bleximo Researcher @amarchenkova at the closing keynote of the #Q2B Conference for a Fireside chat, reflecting on the year's accomplishments and discussions on the future of quantum hardware, error correction, and algorithms