Fatigue in SLE
An NIH lupus cohort study looked at fatigue in SLE and found associations with organ damage, obesity, but does not correlate with disease activity in systemic lupus erythematosus (SLE) patients.
https://t.co/63JVDUwu88
HCQ: 5 mg/kg/day Is Only the Starting Point
HCQ is one of the most important drugs in rheumatology, especially for SLE. It reduces flares, organ damage, cardiovascular events, and pregnancy complications, and it improves survival. Yet many clinicians still prescribe HCQ as if body weight reliably predicts drug exposure. It does not.
https://t.co/PMvEwWD8NP
😍See our recent article on @RheumNowNews@RheumNow how to dose hydroxychloroquine for disorders like #SLE, #lupus, #Sjogrens using modern, personalized medicine tools rather than guessing by body weight:
https://t.co/Uqw3yv8QD9
❤️🔥Many of my patients have been asking me about GLP-1 agonists and if they are safe in autoimmune diseases like #SLE#lupus and #Sjogrens. I go over the medical studies in my latest post:
https://t.co/TULfsvm6sZ
Weight-loss drugs may affect joints directly
A new study from Aarhus University shows that the hormone GLP-1, which is mimicked in medication for diabetes and weight loss, is present in joint fluid. In the long term, this may open up new treatments for arthritis.
https://t.co/P9kYq2lzMI
🔥The modern, most accurate method of dosing hydroxychloroquine (HCQ) is by using drug levels and not by body weight for #lupus#SLE#Sjogrens patients.
https://t.co/O5SDXNEeUp
https://t.co/cQINO8nLP0
The best way to dose HCQ is to measure trough, whole blood levels, and aim for 750 – 1150 ng/mL.
Dosing HCQ at 5 mg/kg/d is so old-fashioned. It underdoses many patients, leading to lupus flares, increased disease activity, and hospitalizations. In others, it leads to toxic levels, increasing the risk of side effects like HCQ retinopathy (eye damage).
There is a strong link between poor sleep and lupus. If you have an autoimmune disease like #SLE, #lupus, or #Sjogrens, getting enough good-quality sleep is really important. Learn more here: https://t.co/SXBznumCMI
Thanks to @Kaleidoscope_FL
😡I hate it when recent #SLE#lupus research studies start off with the statement "lupus is a disease of unknown cause." That is simply NOT true. #SLE#lupus#Sjogrens and related autoimmune diseases are "polygenetic diseases!" A session at last year's annual @ACRheum meeting emphasized this, and I stood and applauded the presenters for proving this.
Family members of people with autoimmune diseases are increased risk of developing these disorders, but there are things they can do to lower their chances. Give your family members a copy of my recommendations: https://t.co/nQKvWa0w5E
😡 Almost all the labs we rely on to diagnose and follow disease activity in #SLE, #lupus, #Sjogrens are over 55 years old!
https://t.co/TwmJREyhlk
This leads to delayed diagnoses, mistakes in diagnosis, and mistakes in properly identifying disease activity and response to medications.
We need to work on strategies to solve this HUGE problem
Produced by @Kaleidoscope_FL
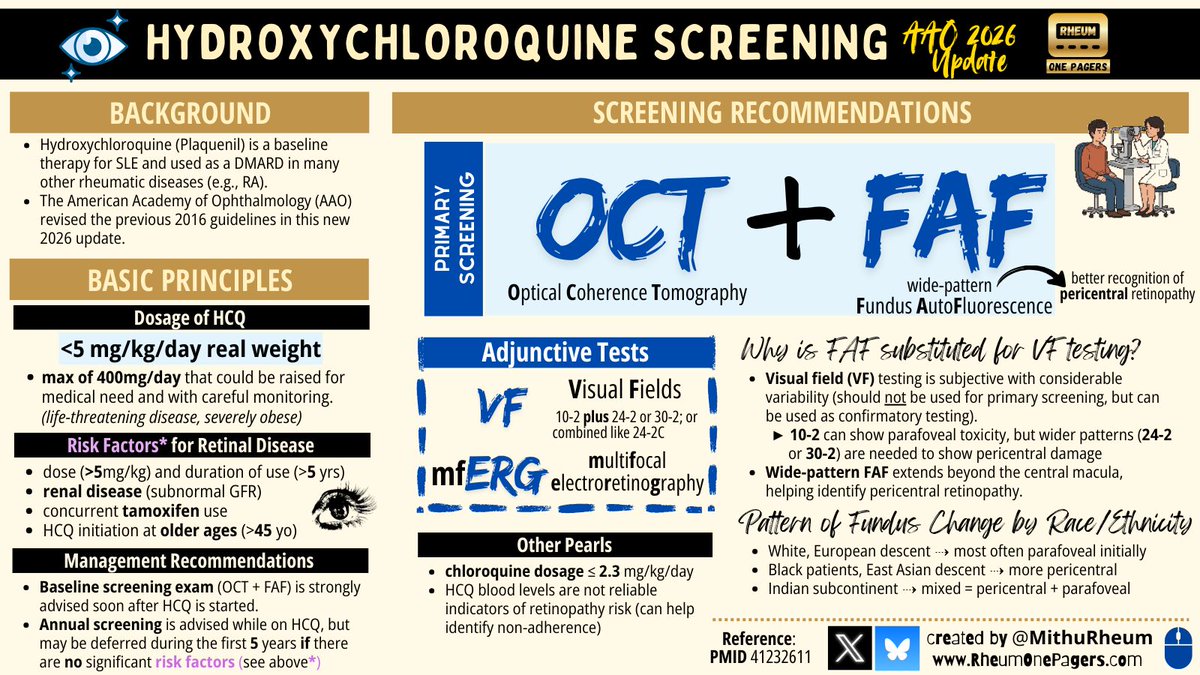
Long-Term Hydroxychloroquine Retinopathy Risk
About one in 18 patients taking hydroxychloroquine (HCQ) for 15 years develop retinal damage, a new meta-analysis indicated.
https://t.co/TBSTIb29Pf
Yet another important reason to use hydroxychloroquine in #SLE#lupus: reduces the loss of kidney function in patients with lupus nephritis! Way to go Garg S et al!
https://t.co/AVfqu7VjgX
Here is a link to a copy of our latest article on how to properly dose hydroxychloroquine.
5 mg/kg/day is NOT the correct dosing for HCQ.
Please share with all healthcare providers so they have a deep understanding on proper prescribing of this important medication.
Link to the pdf article itself: https://t.co/XYhE1ylcpu
Online Link:
https://t.co/vIOKKOOMbk
This is the accepted version of an article published in Arthritis, Care, and Research but has not gone through copy editing. This is a "Full Access" article. This article is protected by copyright. All rights reserved: Arthritis, Care, & Research
Dr. Mithu Maheswaranathan did an excellent job summarizing the AAO 2025 revision. This is so important to disseminate to rheumatologists as very few of us get the AAO's journal (where the guideline was published).
NOTE: many ophthalmologists do not know the guidelines well, and not all ophthalmologists have both an OCT and an FAF machine. Rheumatologists should specific "SD-OCT and FAF" then actually see the results on the visit note. Another option would be to get an SD-OCT + VF 10-2 + VF 24/2 or 30-2, but getting 3 tests yearly is tedious for patients.
Also... use up to 6.5 mg/kg/d initially of HCQ so it works faster! This is in line with the latest @ACRheum SLE Management guidelines. I've done this for over 2 decades with great success.
ALSO... ignore the bottom middle about HCQ drug levels not being helpful. That is the unfounded opinion of the authors. HCQ has a very wide bioavailability. It is ridiculous to dose such a drug by body weight. Drug levels are the only way to go. Keep the level < 1150 ng/mL and you will do your patient a favor. I have many very obese patients who have levels of 2000-3000 ng/mL and need to be on only 200-300 mg daily
🔥 #SLE#lupus and #Sjogrens often occur together. The @SjogrensOrg just posted a very nice summary, patient-education piece on this topic:
https://t.co/45VN7tRGYI
Hydroxychloroquine allows viruses to attack cancer cells while leaving healthy cells alone.
Seems like information the public deserves to know.
Why do you think they tried to obscure this data in the study? Maybe because it would be bad for the cancer industry’s business.
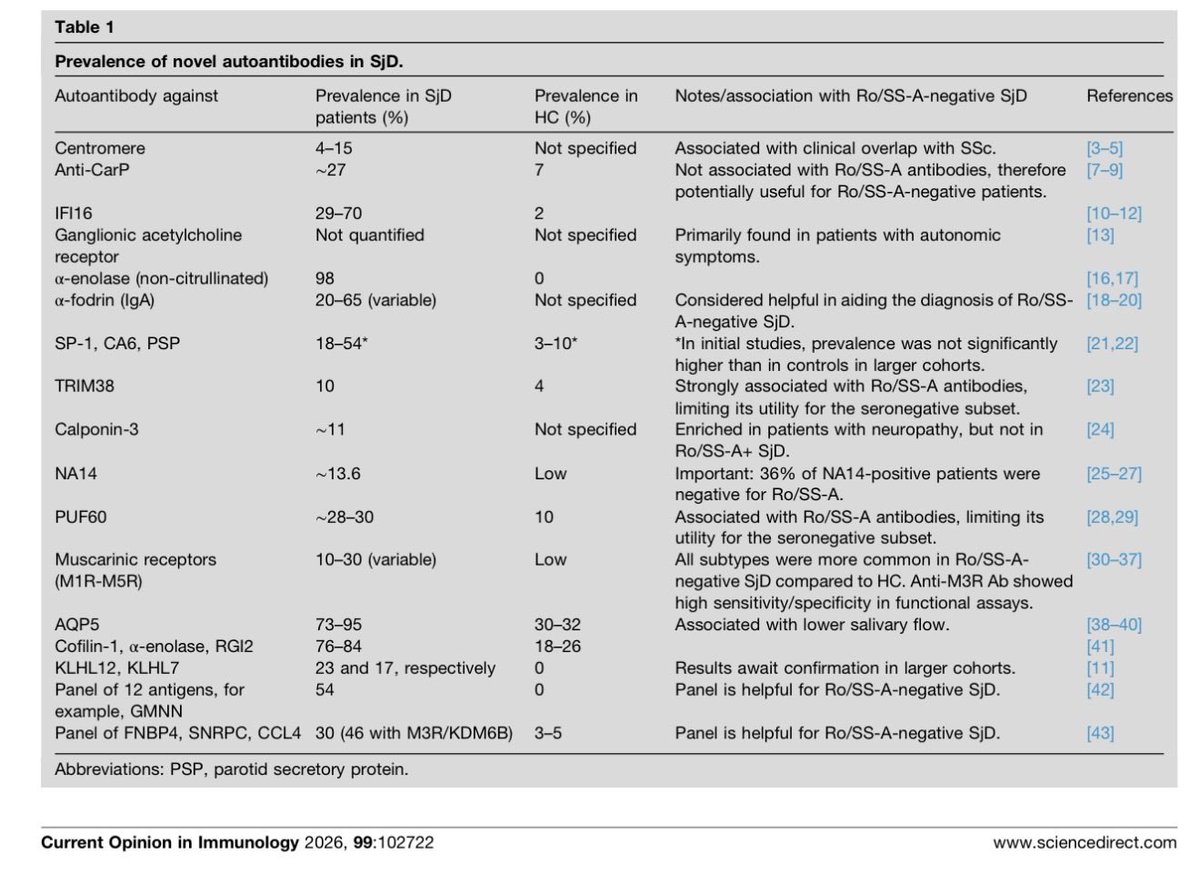
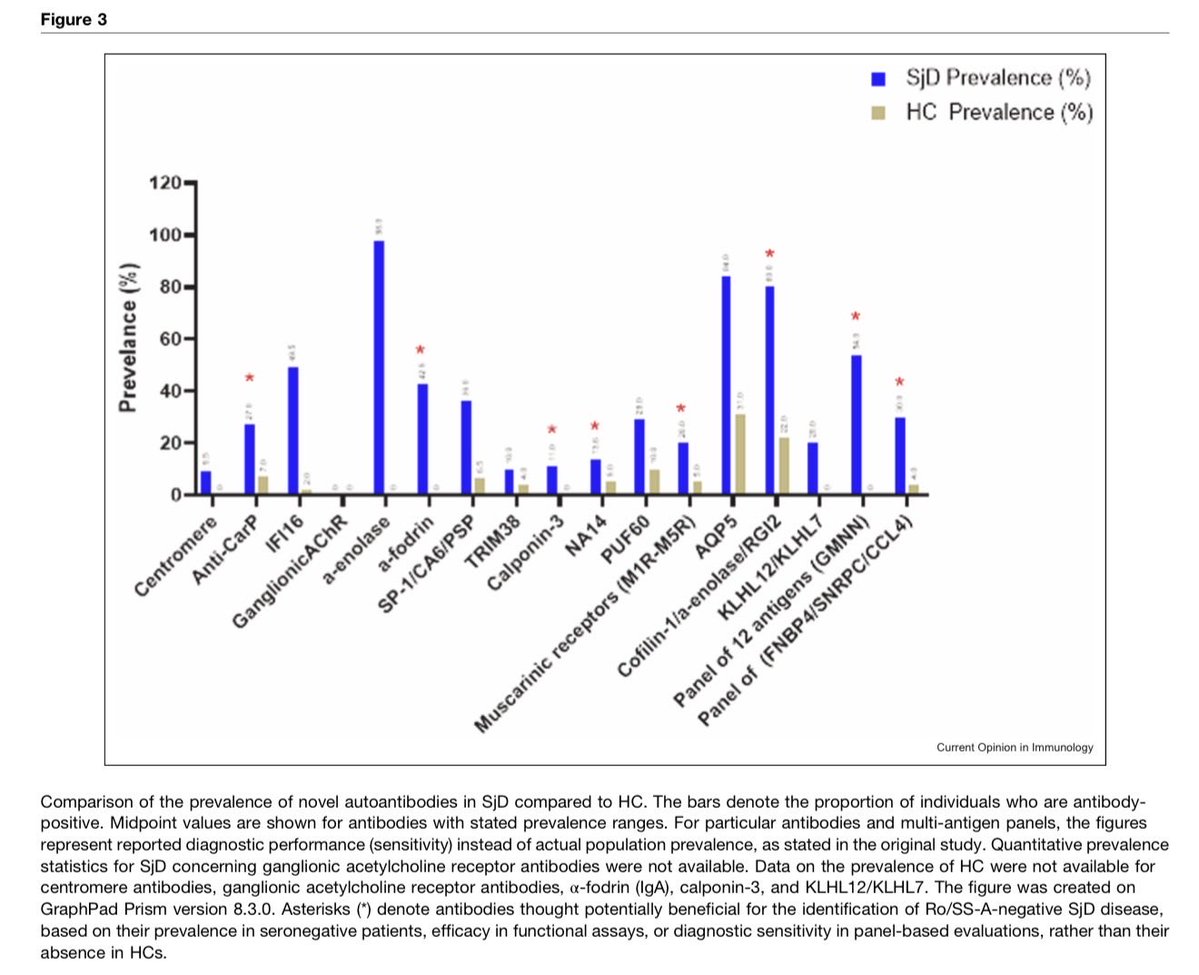
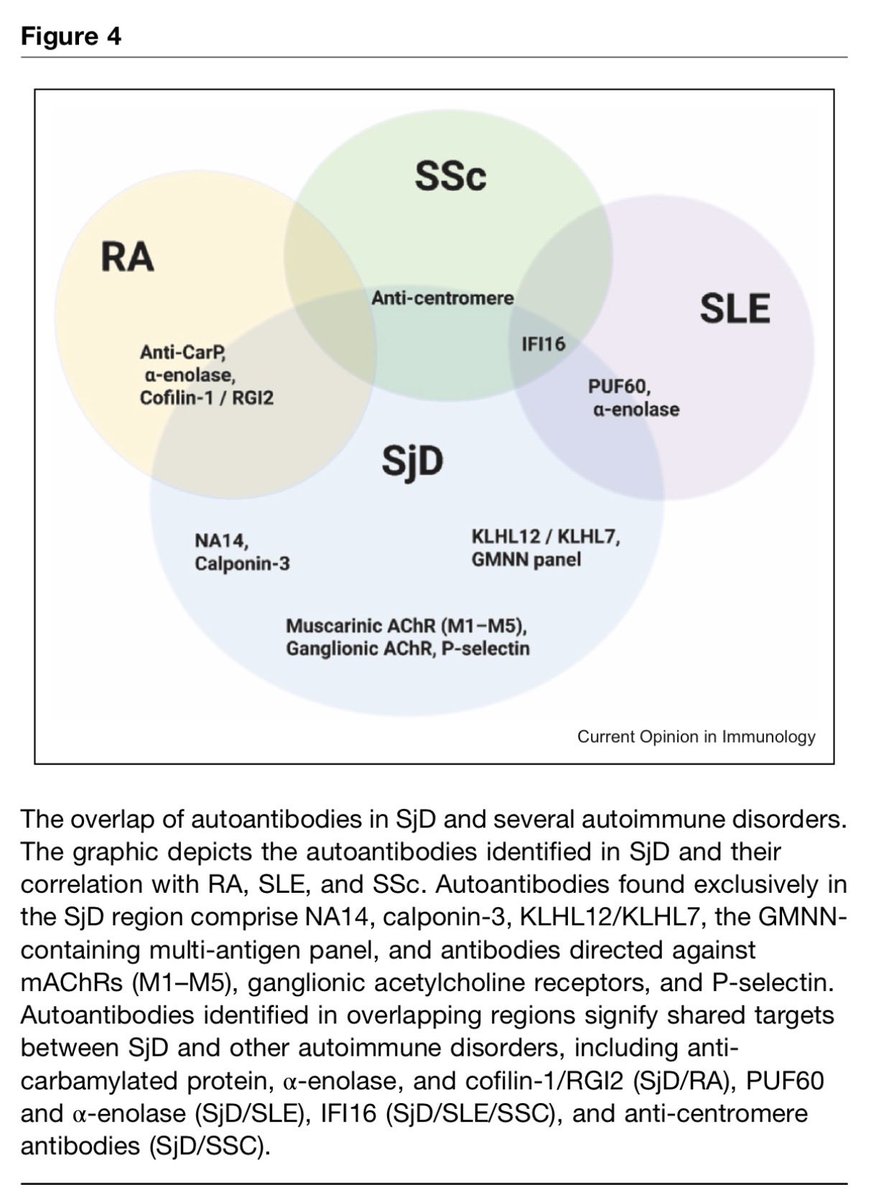
New autoantibodies in Sjögren's disease
#Rheumatology#MedTwitter These findings strongly suggest that a multi-marker panel approach is the most promising strategy for developing a new diagnostic test for seronegative SjD…
⚡️Most #SLE patients will have cutaneous #lupus where it attacks their skin.
CLICK: https://t.co/fCH5q53TzC
Figuring out if a rash is due to lupus or due to something else (like a drug allergy, steroid-induced rosacea, psoriasis, and many other mimics), I recommend that most lupus patients with cutaneous lupus also see a "medical dermatologist" regularly and especially see them for any unusual, new rash.
A medical dermatologist is a dermatologist who focuses their practice on medical skin conditions, such as lupus, rather than cosmetic dermatology.
APPIPRA Study - Benefits of Early Treatment
Treating people who are at high risk of rheumatoid arthritis (RA) can delay the onset of the disease for several years, with benefits also continuing well after treatment has stopped.
https://t.co/hgxj936CWn