Q4: #ESHREjc Until prospective data arrive, what’s a proportionate counseling message for TTC/IVF patients needing analgesia, what alternatives, what timing advice, and how to avoid over-restriction that drives unsafe NSAID substitution? @ESHRE
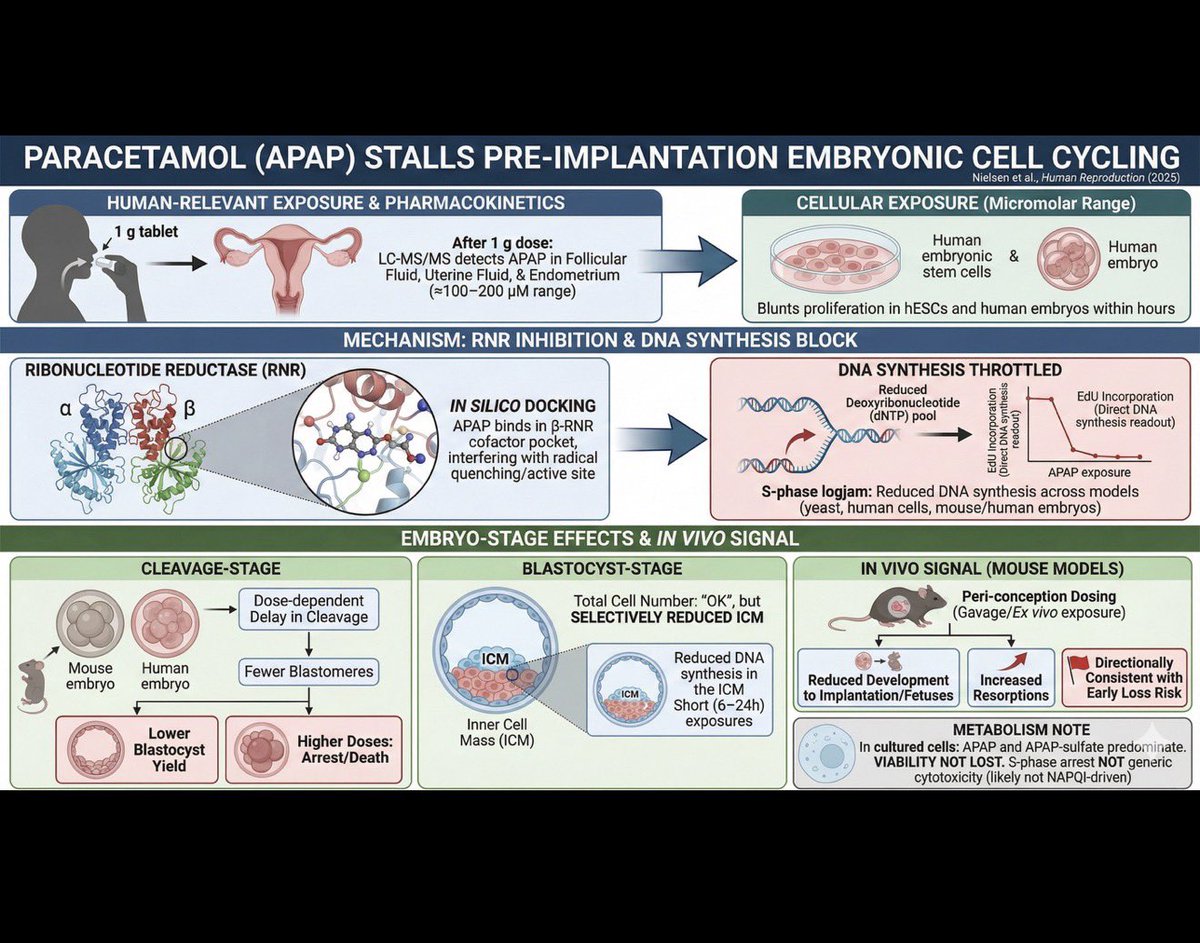
🚨Q1 #ESHREjc The study finds that APAP delays cleavage-stage divisions, while blastocysts keep total cells but show reduced ICM and DNA synthesis. What do these stage-specific vulnerabilities imply for implantation and embryo competence?
@ESHRE
1/ This #ESHREjc we are discussing how a common analgesic Acetaminophen (APAP) may interfere with pre-implantation embryo development.
Study in focus: https://t.co/06gl7eXX2t
A tweetorial to get you up and ready for tomorrow.
#ESHREjc@ESHRE
🚨 Could a common painkiller disrupt the earliest stages of human embryo development?
Join us for the next #ESHREjc
🗓️ 28–29 November
⏰ 17:00 CET start
📍 on @ESHRE
🔗 https://t.co/06gl7eYuS1
🌟 @juliauraji, Thanos Papathanasiou & David Kristensen
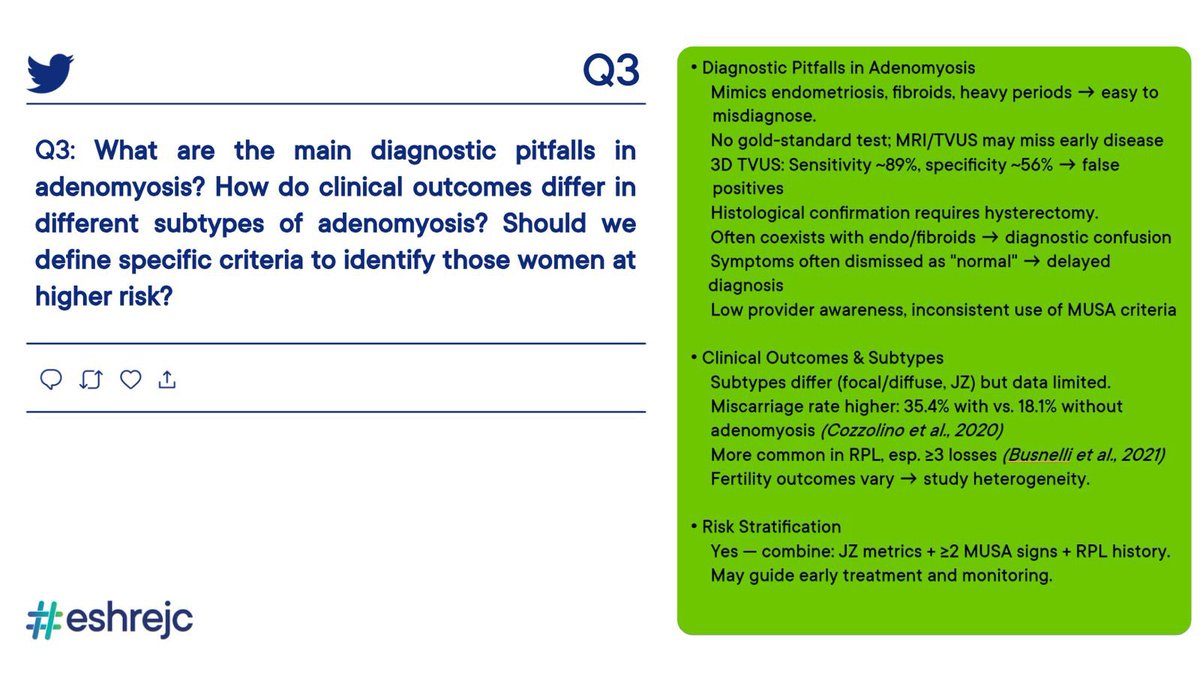
Q3: What are the main diagnostic pitfalls in adenomyosis? How do clinical outcomes differ in subtypes of adenomyosis? Should we define specific criteria to identify those women at higher risk? #ESHREjc@CatenaUrsula@AlexQuaas
Q4: Moving into the “ideal” setting of IVF.
✨LBR after multiple ET reach 60–70% in women <35 years….
🔎to what extent can the remaining failure be explained by uterine factors? could this account for the entire 30–40%? Or are we missing something else? #ESHREjc
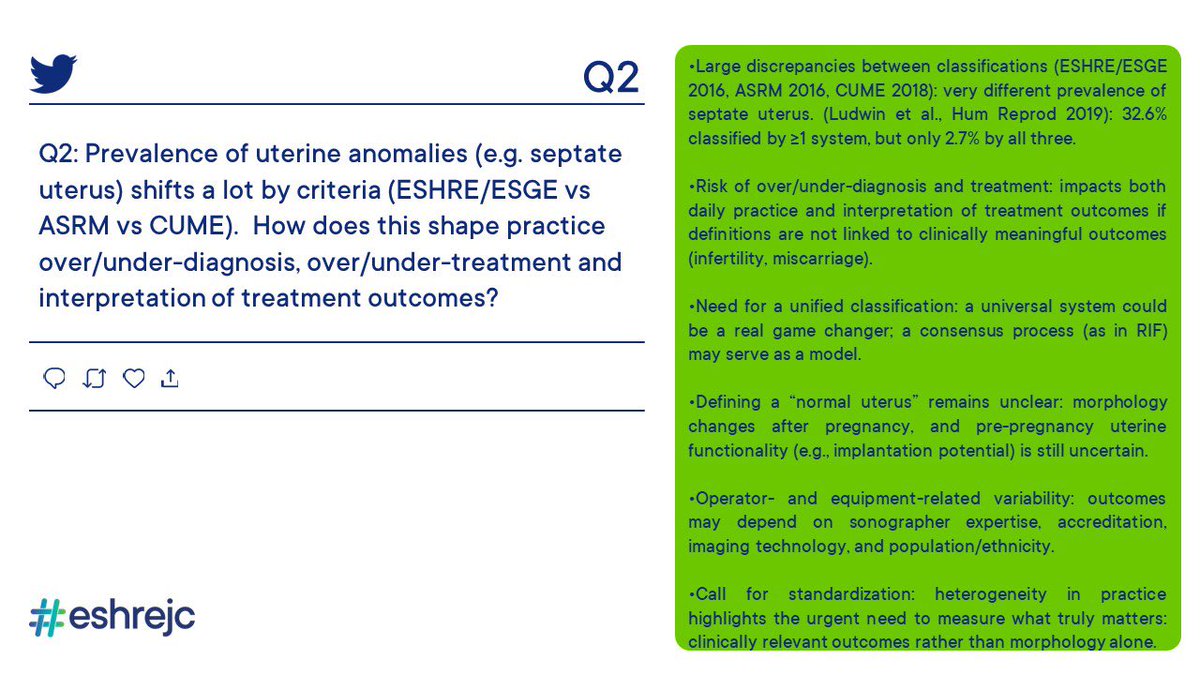
🚨Q2:
Prevalence of uterine anomalies (e.g. septate uterus) shifts a lot by criteria (ESHRE/ESGE vs ASRM vs CUME).
👉🏼How does this shape practice over/under-diagnosis, over/under-treatment and interpretation of treatment outcomes?
#ESHREJC
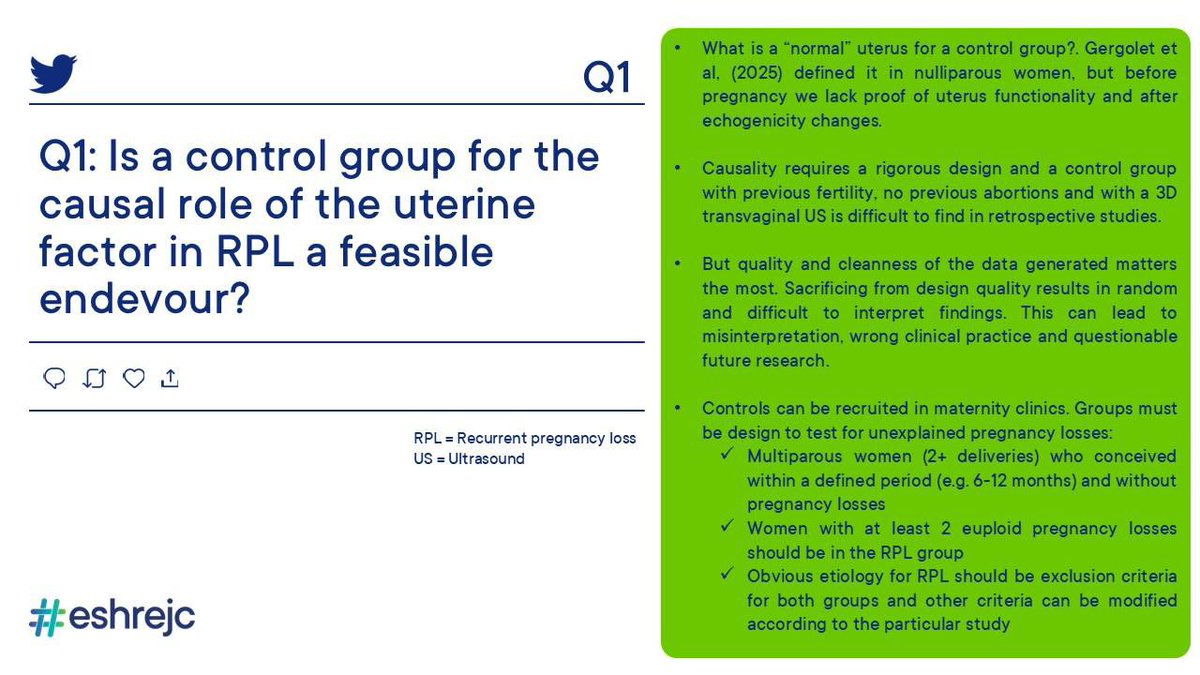
Q1: To demonstrate a causal role of the uterine factor on RPL, a control group of 👭is needed with
-previous fertility
-no previous abortions
-with a 3D transv US
Is this a feasible endevour? Can causality be inferred even if diagnostic guidelines are heterogeneous? #ESHREjc
@GLiperis@ESHRE@CatenaUrsula Adenomyosis is a “shades of gray” rather than “black and white” condition so it is challenging to establish association vs causation and clinical relevance.
@GLiperis@AlexQuaas Should we define high-risk criteria?
Yes — combining:
Quantitative JZ metrics.
Number of MUSA features (≥2 direct signs).
Clinical phenotype (primary RPL, multiple losses).
This could identify women most likely to benefit from early interventions or closer monitoring.
@NoemiSalme30386 According to this systematic review the prevalence of uterine factor infertility varies between 2.1 to 16.7%🤔
Studies are extremely heterogeneous
More questions less answers
#Eshrejc
https://t.co/4ZZhAv2HoM
Q4: Moving into the “ideal” setting of IVF.
✨LBR after multiple ET reach 60–70% in women <35 years….
🔎to what extent can the remaining failure be explained by uterine factors? could this account for the entire 30–40%? Or are we missing something else? #ESHREjc
@GLiperis@CatenaUrsula@AlexQuaas Not every Uterus with Adenomyosis is the same
This is also the reason for high heterogeneity between Studies on Adenomyosis associated infertility.
A classification is needed!