@ALFIEEP1@Koichi16423232 Yes. Single His refractory PVC’s give you the same information as VOP (in essence they are one beat entrainment). Also to your point : you can only see fusion AND entrainment at the same time only in AVRT
Polymorphic ventricular tachycardia deteriorating into ventricular fibrillation during radiofrequency-facilitated left bundle branch pacing lead implantation in complete atrioventricular block
https://t.co/TSHvSDynQY
#acc26 Six reasons why CHAMPION AF should not change oral anticoagulation for AF
I will have a formal post up on @theheartorg but here is a short summary
1) Stroke and Ischemic Stroke went the wrong way.
All S -> 33 vs 50 [HR 1.46 95% CI, 0.94-2.27)]
IS -> 27 vs 45; [HR = 1.61; 95% CI, 1.00-2.59)]
Look at those upper-bounds.
2) NI would not have been met for efficacy had they used a margin with both rate ratio and risk difference, which is standard practice.
The margin of 4.8% is based on event rates at 12%, which is 1.4 in relative terms (40% higher). But when event rates come in lower, as they did: 4.8% vs 5.7%, the 4.8% margin is too lenient.
The 0.9% higher rate of the primary endpoint has a 95% CI of (-0.8-2.6%), so 2.6% is less than the margin of 4.8%. Now do it with relative risk.
It's in table 2. The relative risk is 1.20. The 95% confidence intervals were 0.87-1.66. Note that 1.66> 1.40 so LAAC is not noninferior based on rate ratio margins
3) The primary safety endpoint is flawed because it excludes periprocedural bleeding and uses nonmajor bleeds, such as gum bleeds and bruising. It's open label trial so who which group will complain of more nonmajor bleeding?
4) When counting all events, Watchman barely reduced major bleeds. Also in the main results table is that major bleeds were 83 vs 87 (5.5% vs 5.8%; HR 0.92 95% CI 0.68-1.24)
5) Net Clinical Benefit was also flawed because they used nonprocedural bleeding and nonmajor bleeds.
A normal patient would simply say, there were 17 more strokes and only 4 less bleeds. Hardly a good trade.
6) Bayes: trials don't give answers, they update priors. For Watchman, you have PREVAIL failing against warfarin, CLOSURE AF clearly failing against best med Rx (mostly DOACs) so priors are pessimistic. To go from pessimistic priors to enthusiastic posteriors you'd need hugely positive data. CHAMPION is not that.
Don't believe the stories that CLOSURE failed due to them using other LAAC devices. In the AMULET IDE trial, Watchman and Amulet were similar. Also, if you believe that German operators are worse than US authors, you need to travel more.
Conclusion: Oral anticoagulation for AF is one of the most evidence-based practices in all of medicine. To upend that would take much stronger data.
Don't be bamboozled by this trial, which was designed to be positive before the first patient was enrolled.
#ACC2026
I was told recently by an enthusiastic colleague that how one looks at recent CLOSURE and CHAMPION data on left atrial appendage closure is like a Rorschach test
Meaning (I think) evidence appraisal is in the eye of the reviewer
I disagree strongly. Evidence is evidence
CLOSURE: LAAC inferior to best med Rx
CHAMPION: Ischemic stroke 60% higher in LAAC vs DOAC and total bleeding similar. Not superior.
👆Simple facts. Like the sky is blue.
LAAC is clearly not better than best medical therapy or DOAC—is what the evidence says
MELOS RELOADED adds more weight to a growing question in pacing:
In patients with AV block, preserved or mildly reduced EF, and a high expected pacing burden, should right ventricular pacing still be the default?
After propensity matching, 3,382 patients were studied.
At 4 years, LBBAP showed an absolute survival advantage of 11.8%.
Mortality was lower with LBBAP: HR 0.53.
HF hospitalization or CRT upgrade was also lower: 4.6% vs 11.2%.
And one more key point:
Not all “LBBAP” is equal. Failure to confirm true left bundle capture carried higher mortality.
Lead position is not the endpoint.
Physiologic capture is.
@Marek_Jastrz_EP@HaranBurri@ZacharyWhinnett
#Electrophysiology #CardioTwitter #Pacing
Another beautiful study on PVCs
Transcutaneous Electrical Vagus Nerve Stimulation to Suppress Ventricular Premature Complexes [was no better than sham]
Proves my long-time contention for PVC Rx —> Voltaire approach. Do nothing. Reassure. Wait.
https://t.co/4B5kzrBBIc
Characteristics, Clinical Course, and Cardiac Events of Patients with Previously Asymptomatic Long QT Syndrome
@MJAckermanMDPhD@EllianaRudquist
https://t.co/vLtGKPodCu
⚡ Brugada syndrome is not just a sodium channel disease.
For years, we simplified Brugada as:
👉 SCN5A
👉 sodium current
👉 channelopathy
But here’s the problem:
👉 This explains only 20–30% of patients
🧠 So what about the rest?
This paper pushes the field forward:
👉 Brugada = a multi-layer disease
🔬 New insight: proteomics
Using Mendelian randomization across large cohorts,
they identify novel protein pathways linked to BrS:
• Cytoskeletal regulation
• Stress-response signaling
• Extracellular matrix remodeling
➡️ Not random findings
➡️ A coherent biological network
💥 Key players:
• MMP1 → fibrosis / structural substrate
• HSPB1 → protein folding / stress response
• MAPKAPK2 → inflammation + signaling
• PDLIM4 → cytoskeletal organization
🔥 Translation:
👉 The problem is not only the ion channel
👉 It’s the environment where the channel lives
⚡ This explains what we already see clinically:
• Epicardial substrate
• Fibrosis in RVOT
• Inflammatory signals
• Success of substrate ablation
👉 Hard to reconcile with a “pure channelopathy”
🧬 New concept:
👉 Structural + molecular dysfunction
→ leads to an “acquired channelopathy”
Even normal channels
can behave abnormally in a diseased substrate
⚠️ And this changes everything:
• Risk stratification
• Biomarkers (plasma proteins?)
• Patient selection for ablation
• Future targeted therapies
🎯 Take-home message
Brugada is evolving from:
⚡ channel disease
➡️
🫀 substrate-based cardiomyopathy
💬 Are we ready to stop calling Brugada a “pure channelopathy”?
#Cardiology #BrugadaSyndrome #Arrhythmia
#Genetics #PrecisionMedicine #EPeeps
#CardioTwitter ⚡🫀
https://t.co/qjxHJAvXaV
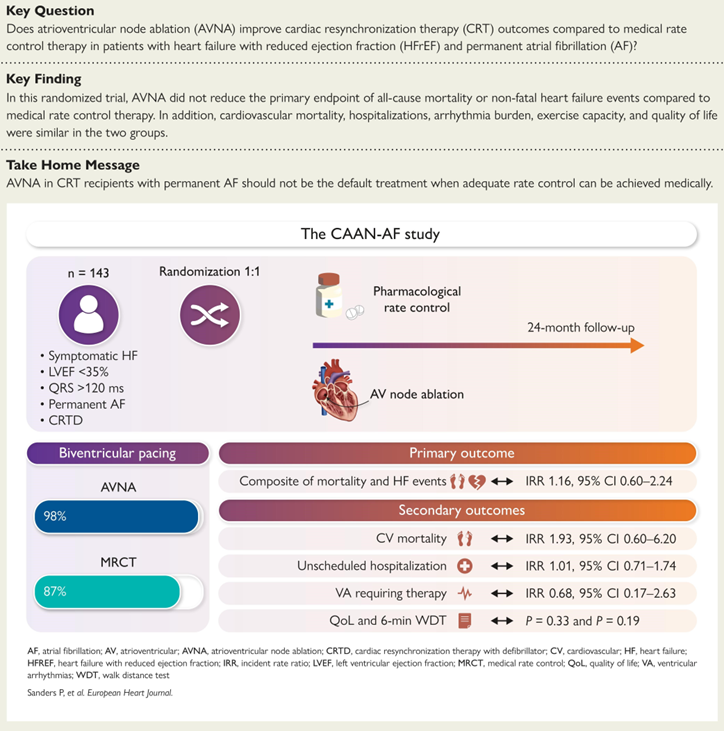
CAAN-AF Trial #CHRD@adelaide87018
Our previous meta-analysis of observational studies suggested CRT patients with AF had a significant 58% reduction in all-cause mortality with AV node ablation - https://t.co/rLbkUhqZLX
We designed the CAAN AF Trial supported by the @nhmrc and critical industry partners - in order of support @bostonsci@AbbottNews@Medtronic@MicroPort - Methodology paper - https://t.co/kZrLVV9G9q
CAAN AF Trial: https://t.co/bMIaH2CPHV
RCT showing no benefit in the routine use of AV node ablation
Clinical Profile and Mode of Initiation of Spontaneous Ventricular Tachyarrhythmias in Patients With Brugada Syndrome (START-BrS) | JACC: Clinical Electrophysiology https://t.co/tokjJsNUDN