Digging deep!
Another example of turning the difficult into routine.
Combining shape-sensing robotic assisted bronchoscopy with integrated 3D imaging to safely sample targets that were close to unreachable in the past.
What’s the diagnosis?
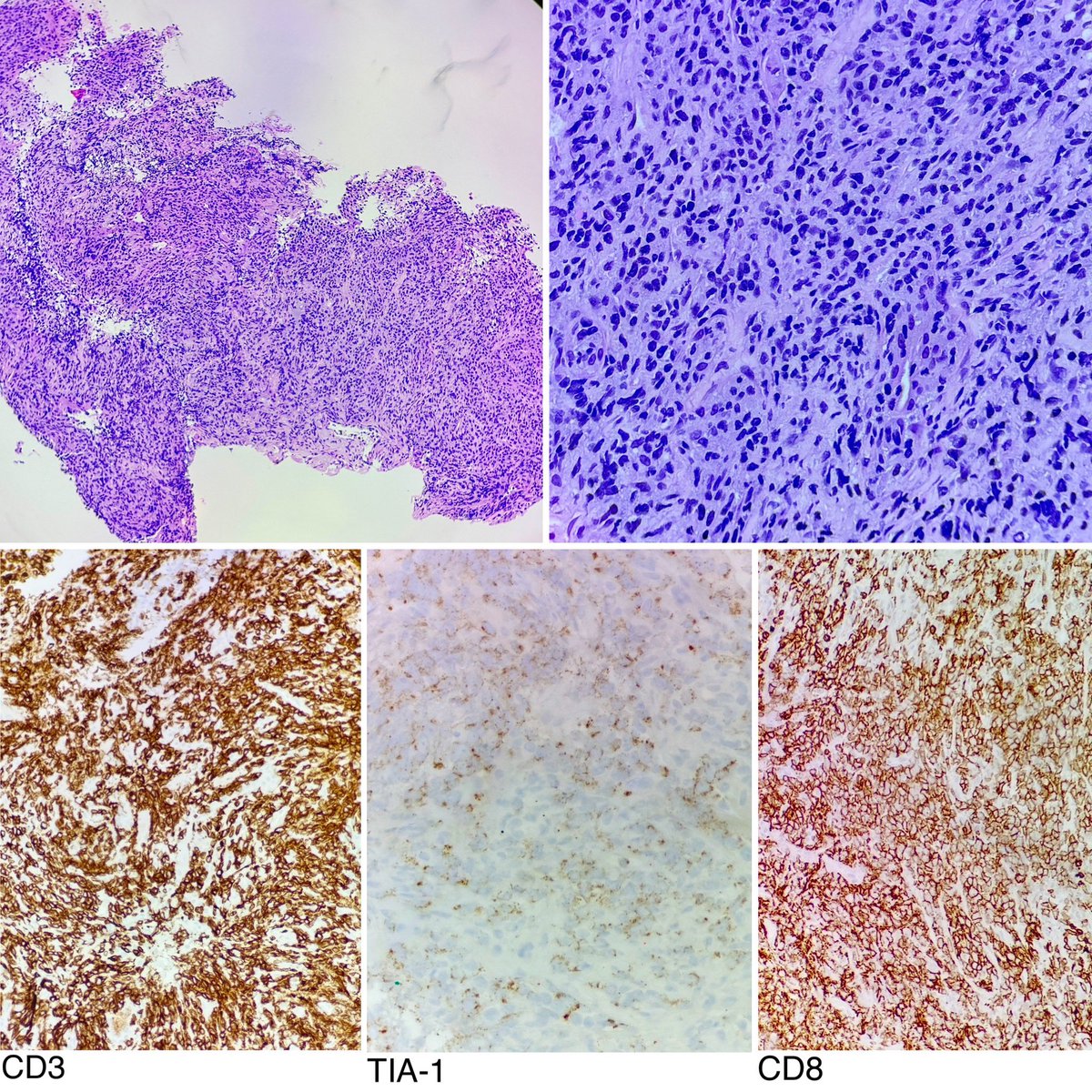
80+ yo man, with cough and multifocal solid to cavitary PET avid lung nodules.
RLL endobronchial mass, smooth but fungating, resected with rigid tools and cryo.
Path slides with sheets of small blue cells and IHC stains as listed.
Simple pleasures.
Said it before, but endobronchial valve treatment for non-resolving air leak due to APF/BPF, in those relatively rare cases when it works instantly and well… easily a top 3 most satisfying IP procedure.
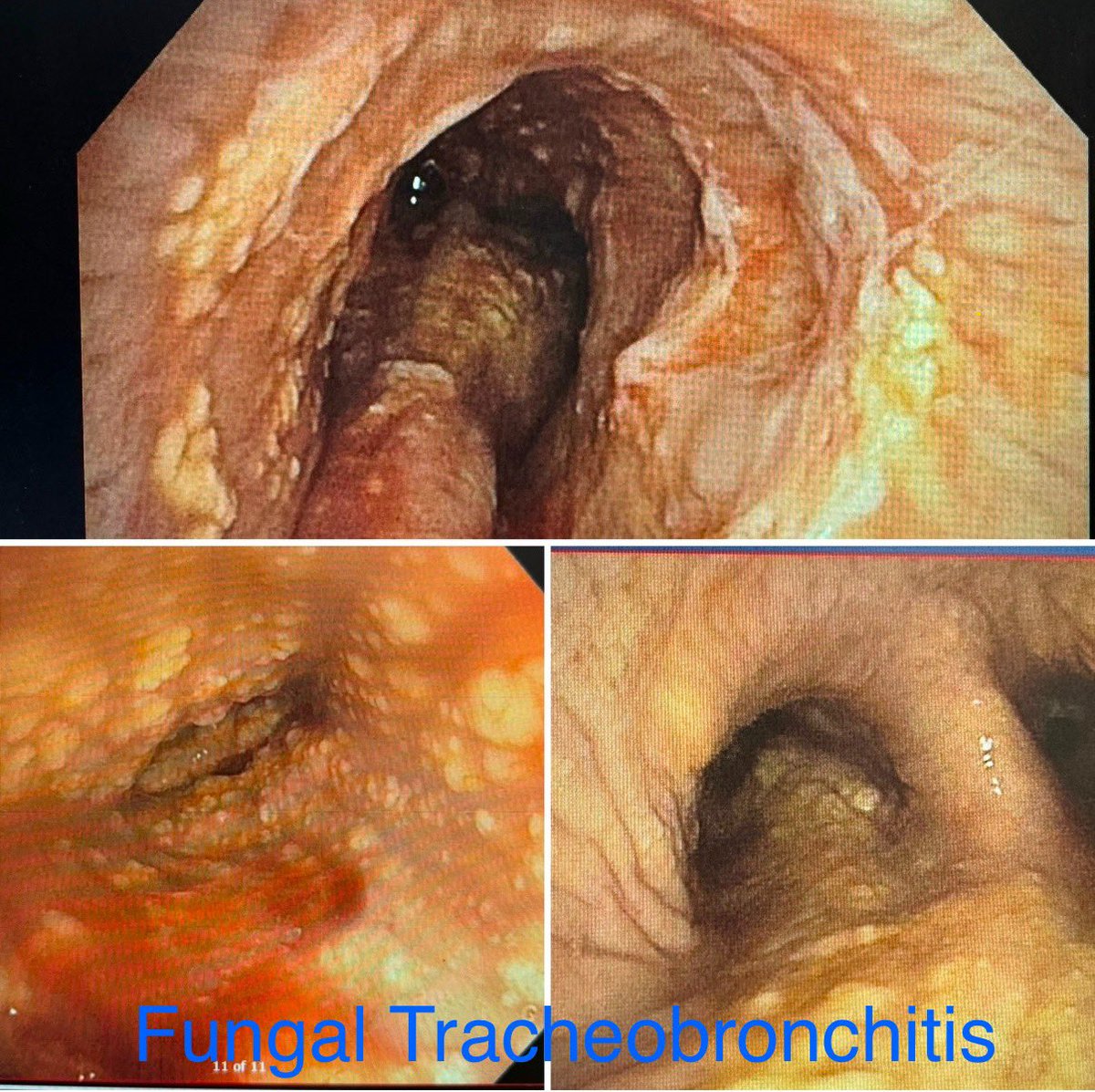
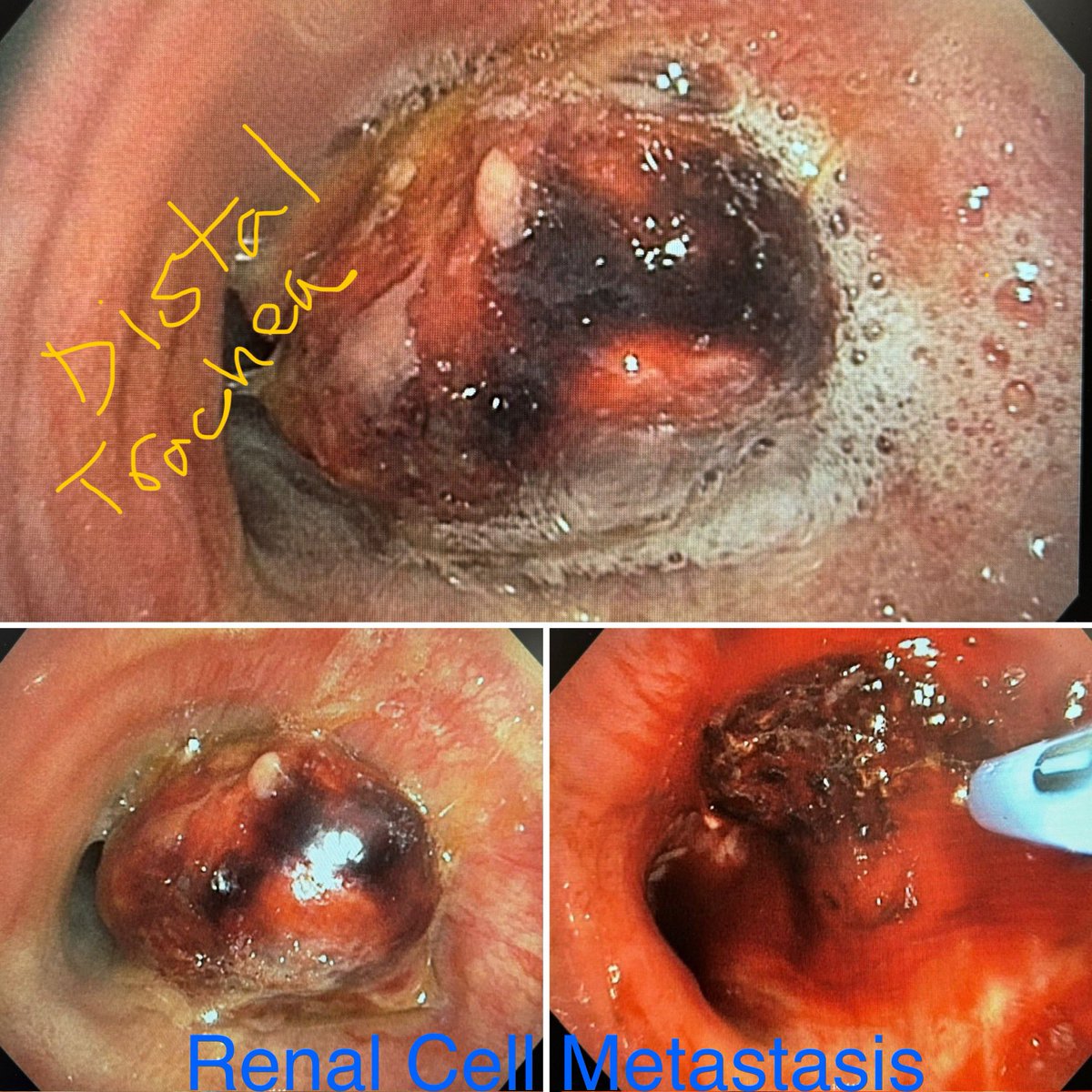
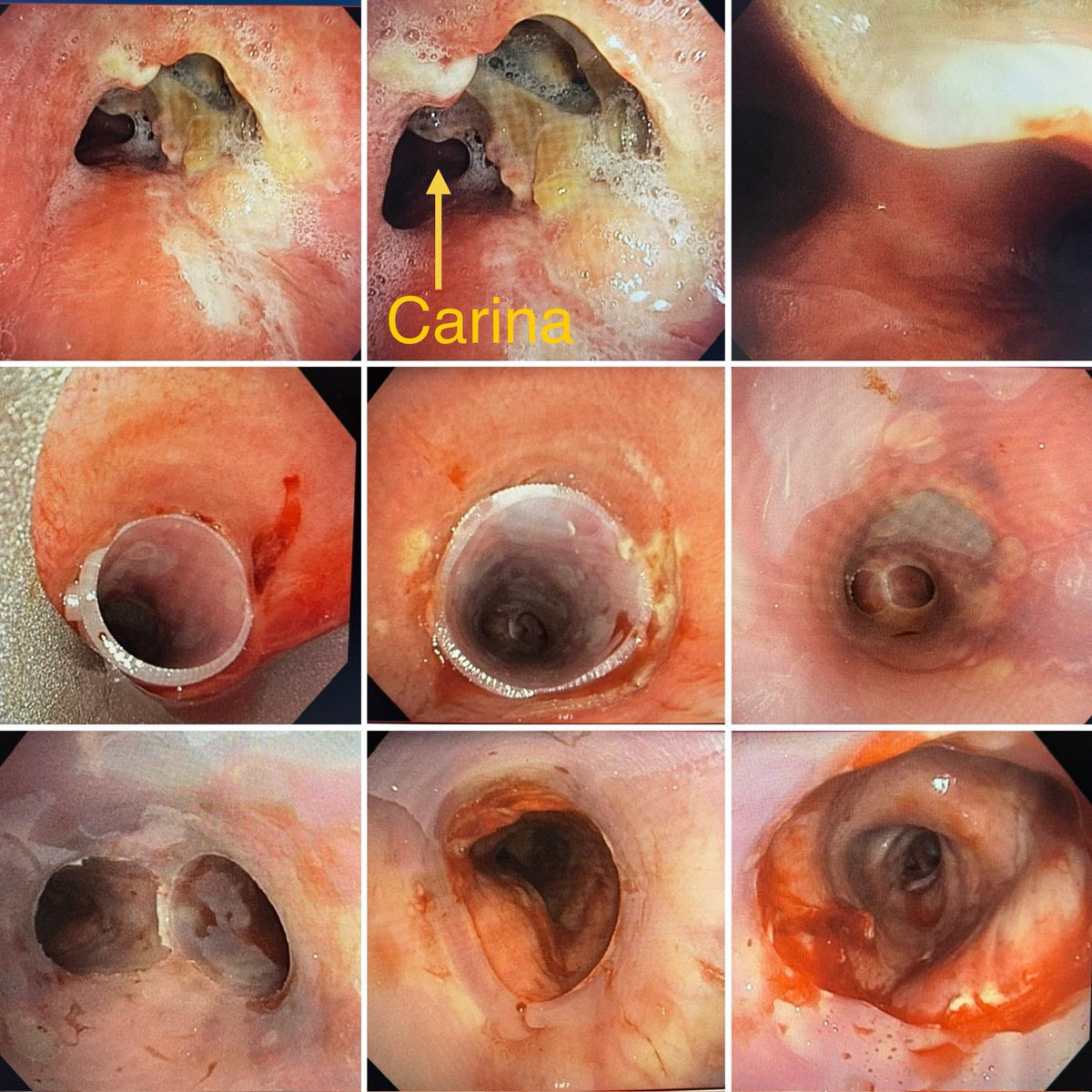
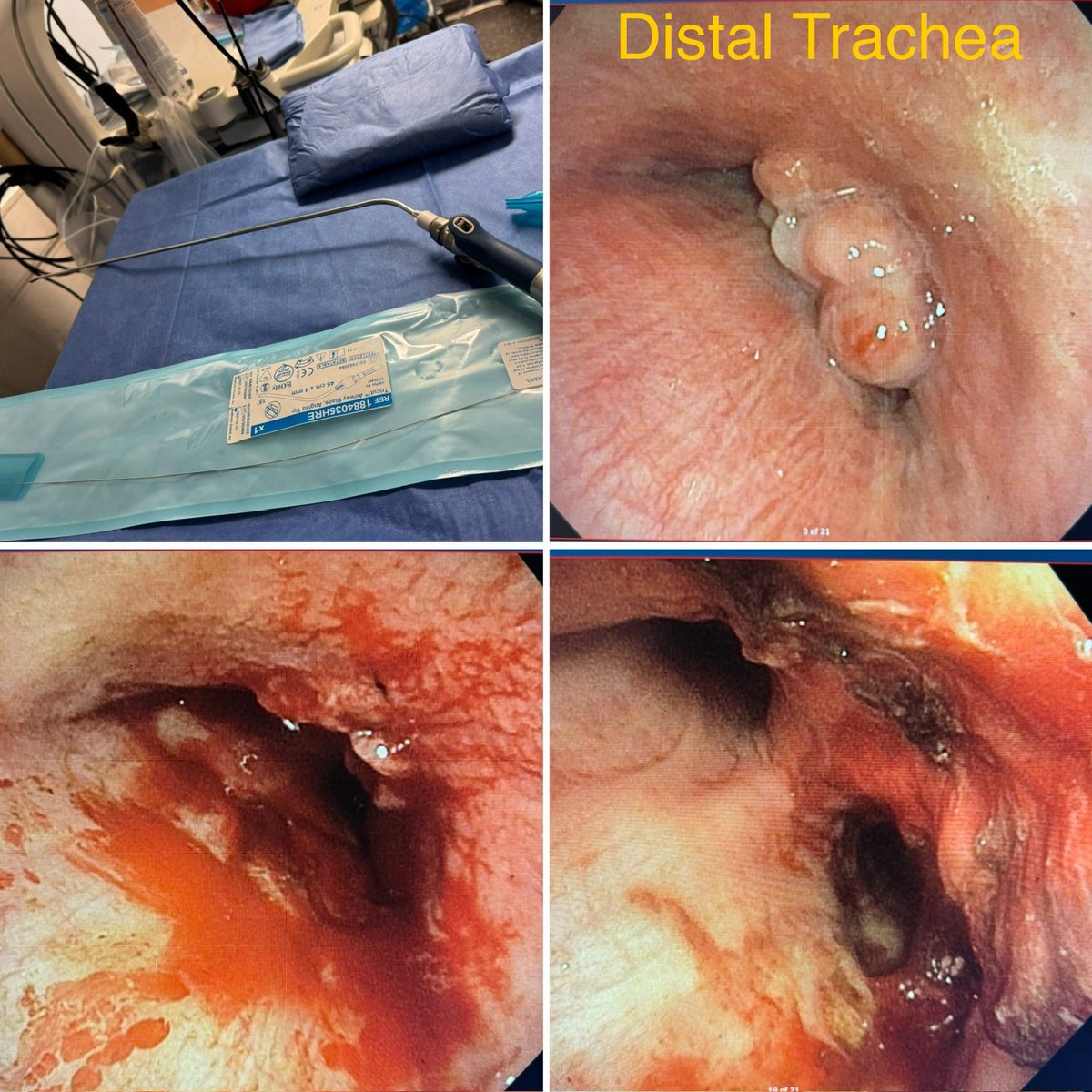
Terrible Things in the Trachea.
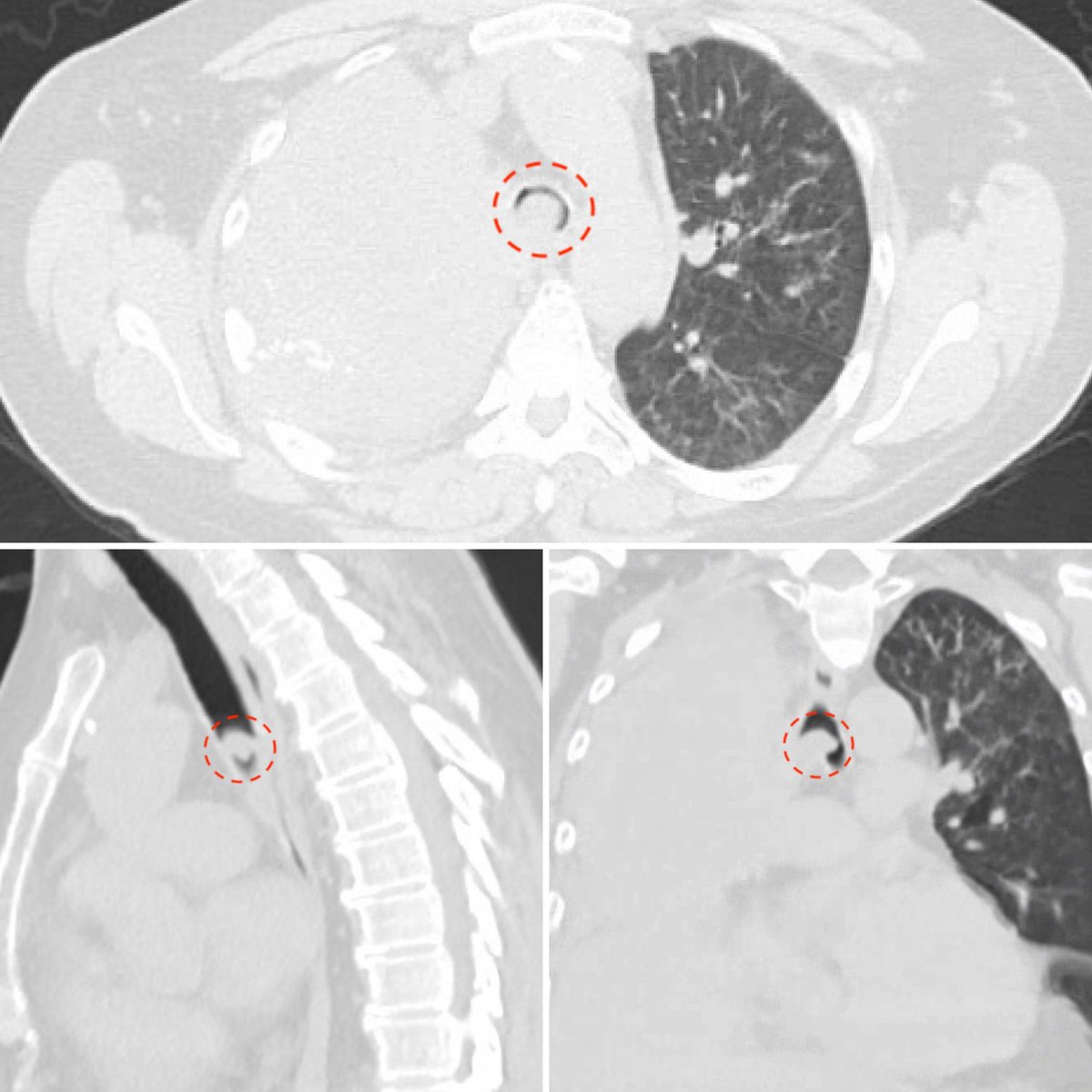
Large necrotic anterior tracheal perforation in setting of metastatic cancer and mediastinal SBRT.
Presenting with mediastinitis and not a surgical candidate.
Palliated with silicone tracheal Y-stent.
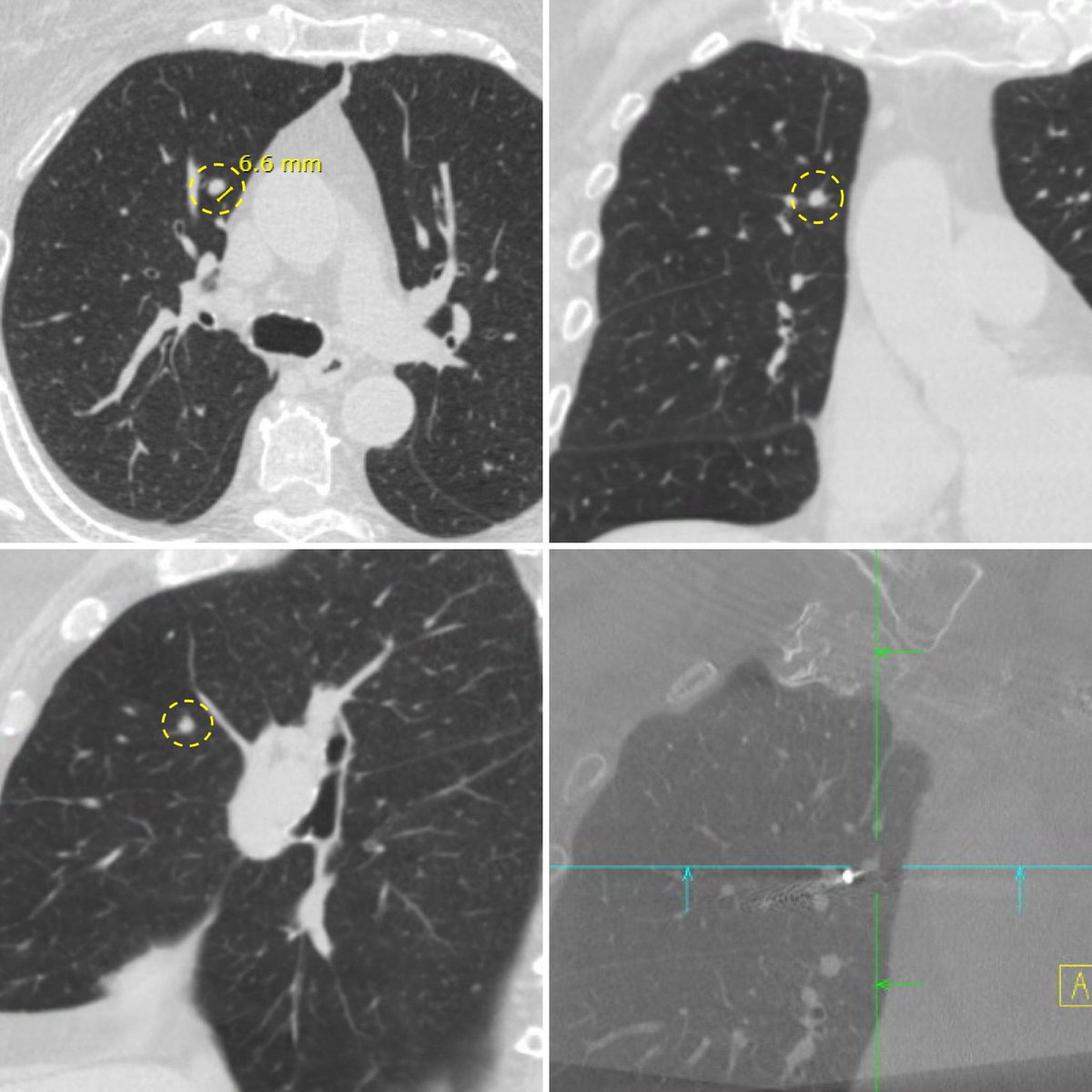
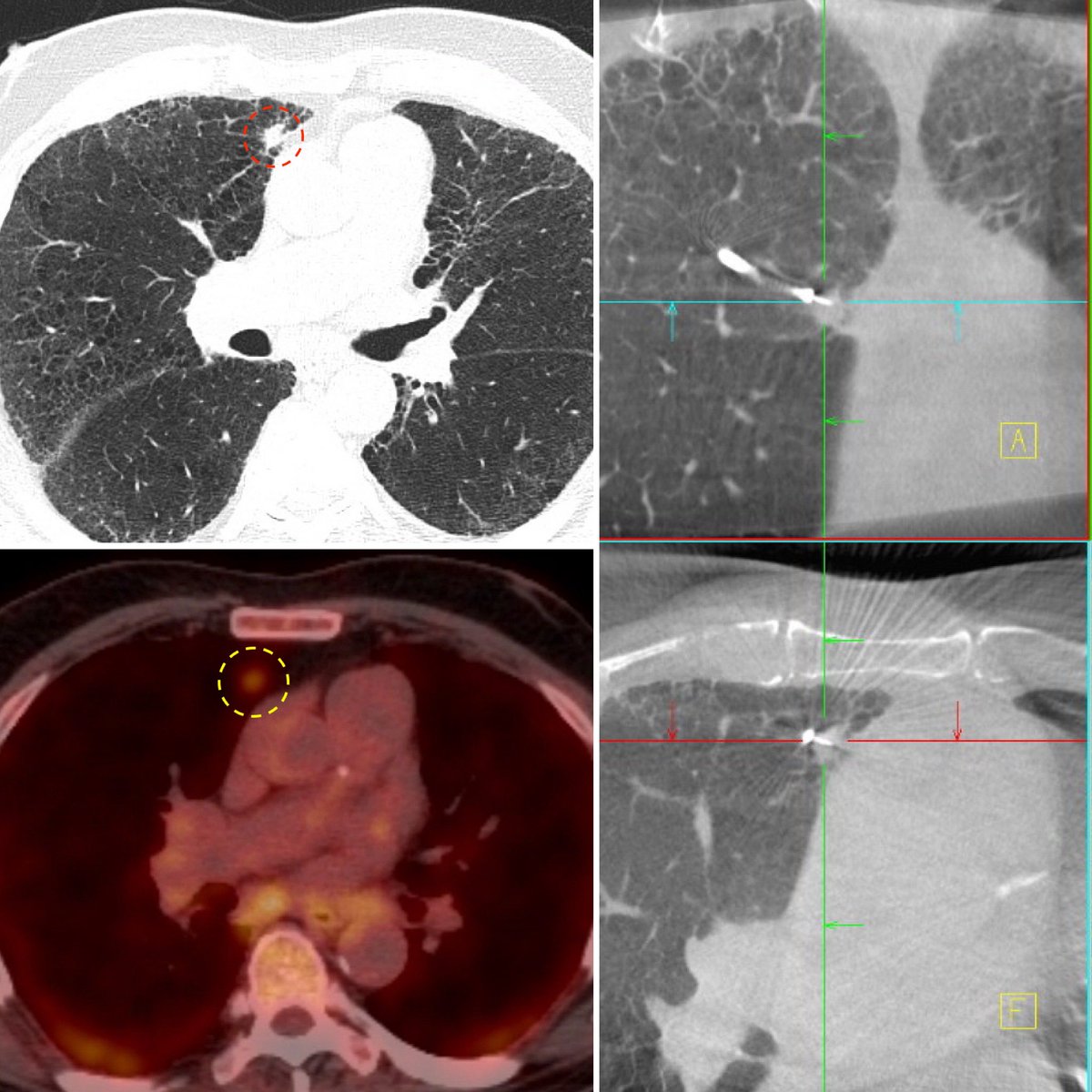
Making the impossible routine!
Shape sensing robotic assisted bronchoscopy, combined with live 3D imaging, allows for unlikely navigational biopsies to become average procedures.
Whether the difficulty is size (6mm nodule), location (above aortic arch), structure (cystic rim), or multiple (size and location)… no target is unreachable, allowing clinical necessity to be the only decision factor in pursuing biopsy. As it should be.
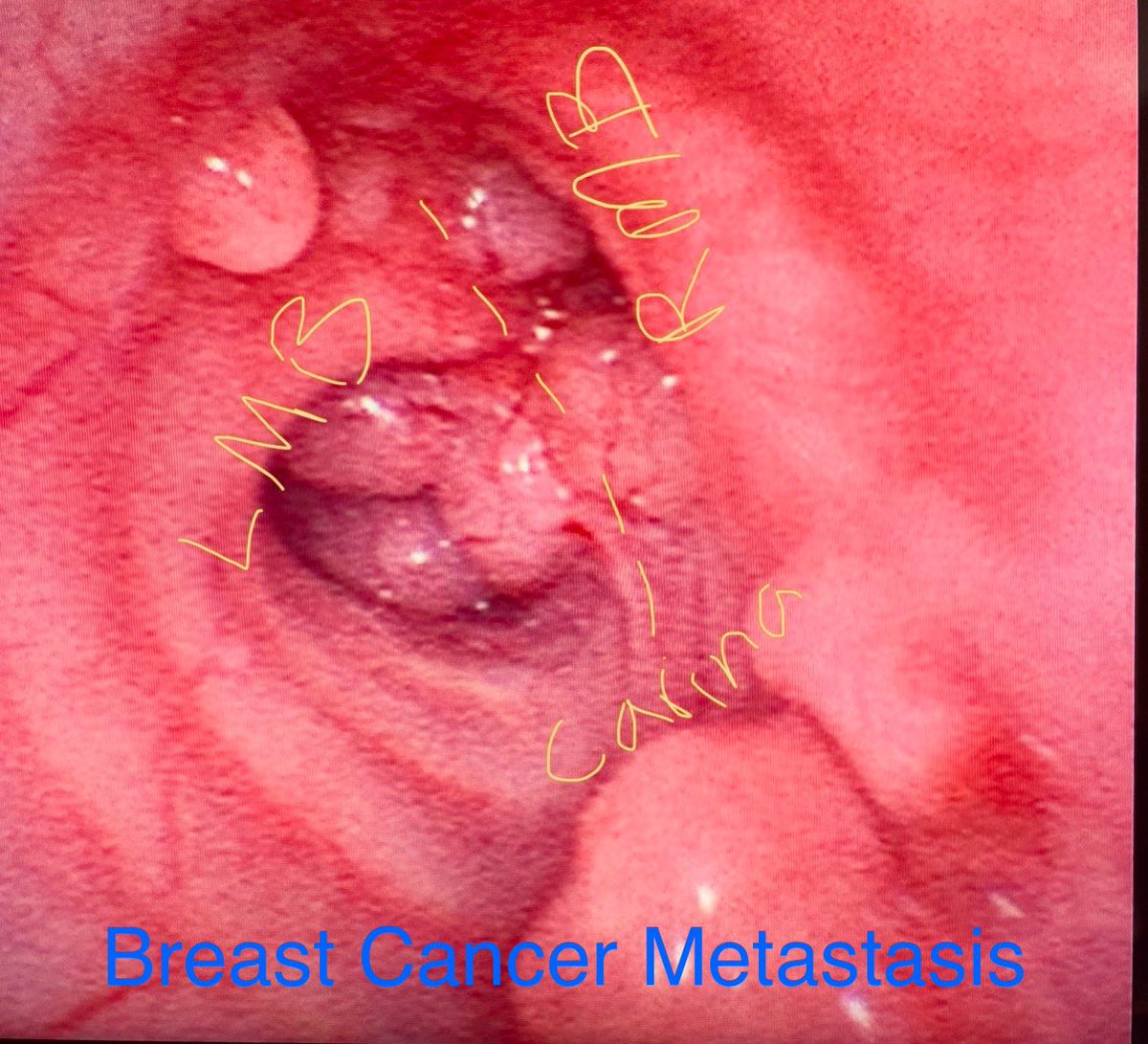
What was the worst thing you found in the airway in 2024?
Was it benign or malignant?
Here’s to a successful 2025 to all you brave airway operators out there!
#InterventionalPulmonology
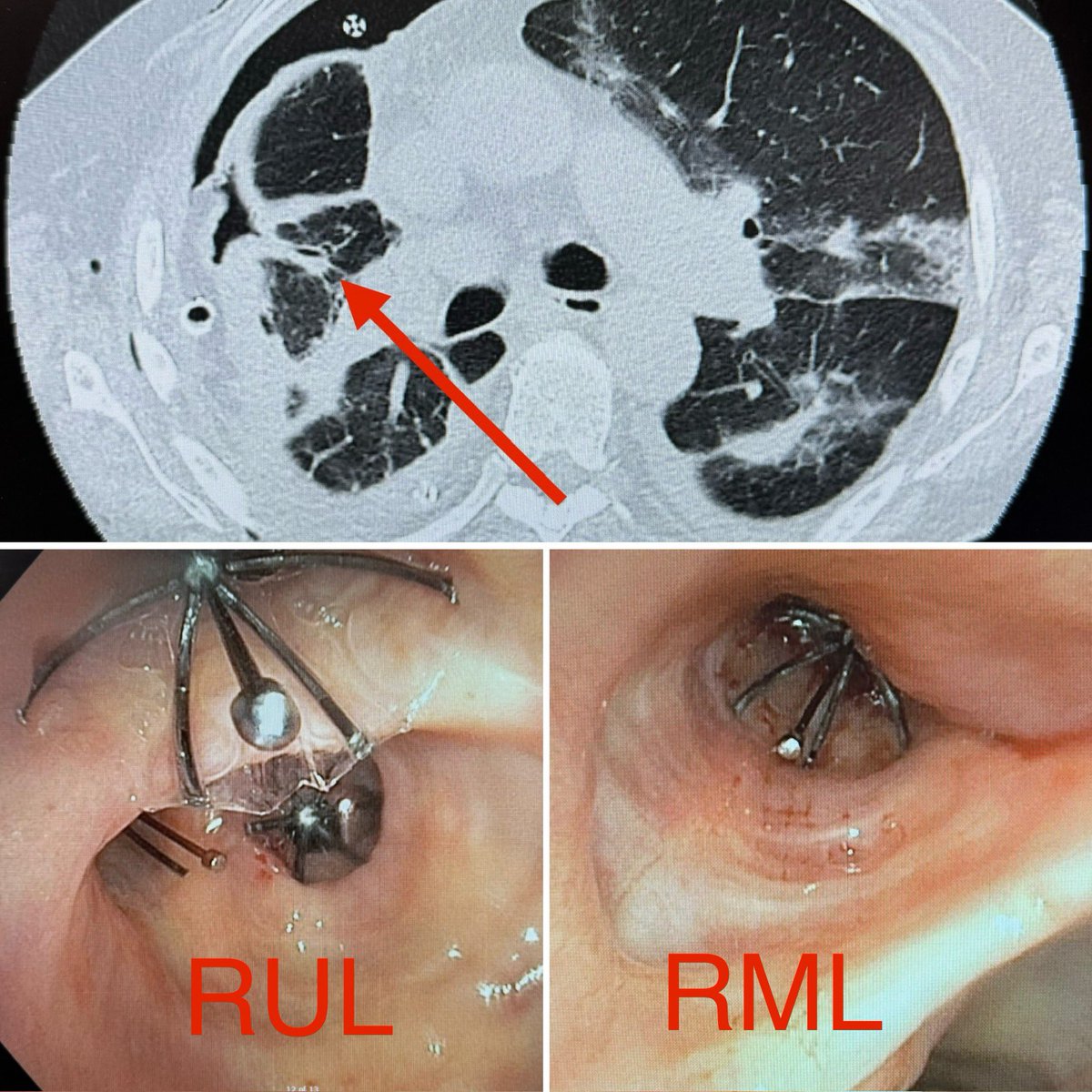
Plugging leaks!
Seems like endobronchial valve treatment for truly significant BPF almost never works. But in those rare cases when it does… good lord is it satisfying!
Patient who already failed surgical repair attempt with wide open air-leak, significant reduction in leak with blockade of RUL + RML and eventual removal of all 3 chest tubes within 1 week.
With @pulmo_dok
The size of the effusion, which wasn’t mentioned in this scenario, makes a big difference in my initial approach.
I agree thora should usually be first step, but I also want to know what’s underneath, and I want effective drainage.
Both of those goals are hard to reach with a single thoracentesis on a large or massive effusion.
The simple pleasures of IP.
Angled Tricut airway microdebrider turning a normally tedious tracheal tumor debulking job into a 60 second breath of fresh air.
Excellent symptomatic response to improve functional status for urgent chemotherapy.
What’s your favorite tool(s) for tracheal obstruction?
With @pulmo_dok
Just needs a good rinse!
Along the zebras and unicorns series…
New diagnosis pulmonary alveolar proteinosis (PAP) presenting in severe respiratory failure, nearing intubation. Treated with VV-ECMO supported bilateral whole lung lavage with excellent response.
With @pulmo_dok
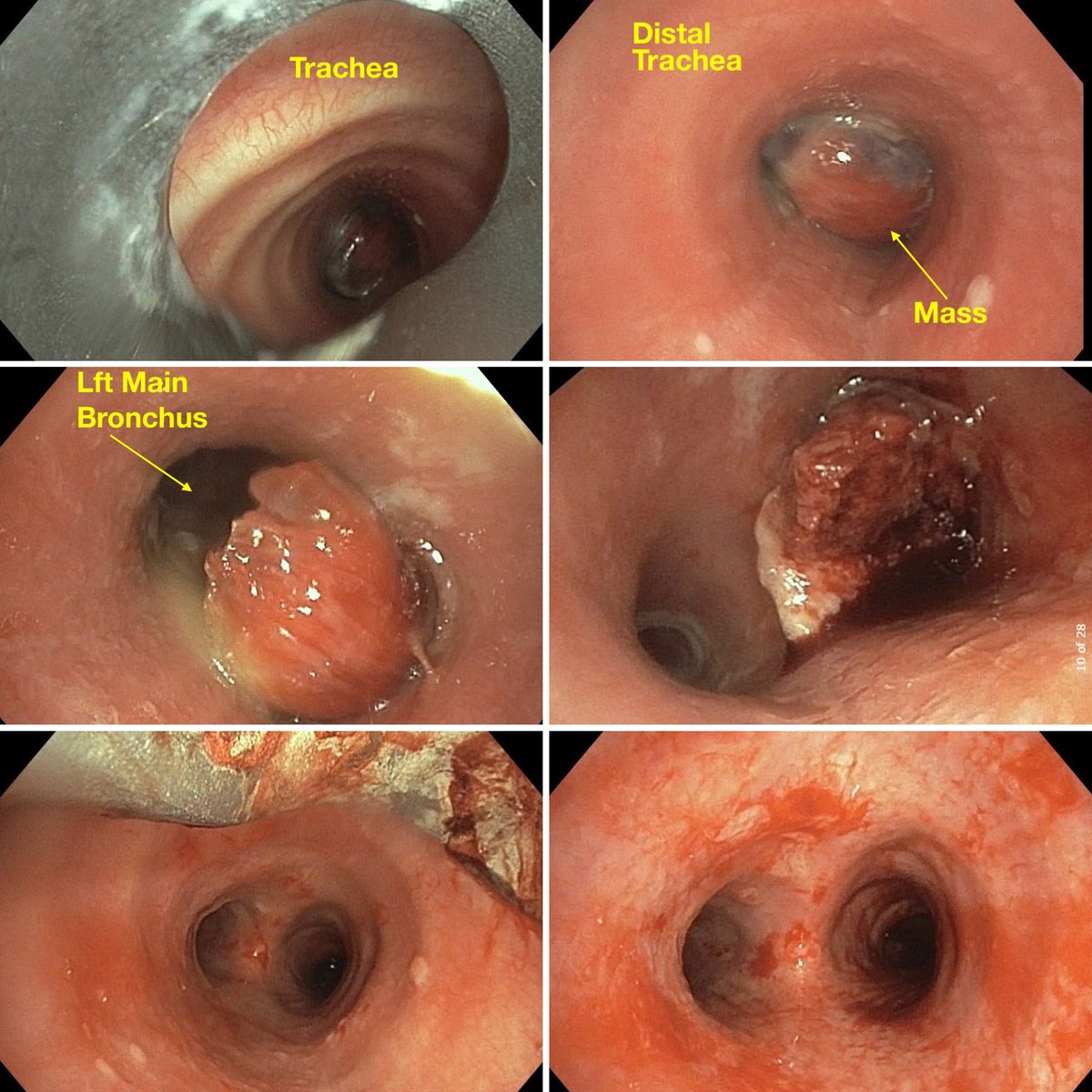
Tunneling. Large right lung mass extending from right main bronchus to create near 100% occlusion of distal trachea.
Resected with snare, cryoprobe, and rigid forceps for complete tracheal recannulization.
With @pulmo_dok
November is Lung Cancer Awareness Month.
Help us spread the word on the importance of lung cancer screening and tobacco use cessation, so we can save as many lives as possible!
#TxIPS#MethodistHospital https://t.co/dj7EDiRiFt