Here is my algorithm:
1) Vasodilator therapy (if hemodynamic allow and pull)
2) Pull Rotawire. This works very effectively, 90% of times. It is frequently overlooked. The 0.014 tip works as a great way to bring back the stuck burr. Make sure wire is free with brake off for maximal efficiency. Pulling the driveshaft is less effective, as it is made of 3 coiled wires which gives some elasticity to the driveshaft.
3) If burr is free beyond lesion, can use short dynaglide runs and then pull. Prinicple is that dynamic friction is lower. Don’t overdo this and also with skipping rope technique, there is risk of driveshaft breakage and burr loss due to torsional forces with a fix s immobile burr!
4) Cut driveshaft and remove teflon sheath
5) Deliver GE over driveshaft to the burr and pull.
6) Intimal/subintimal wire and ballooning to dislodge burr and pull.
7) Re-deliver GE over driveshaft and pull.
8) Obtain second access and adding a ping-pong guide. Remember a ping-pong guide is not required in most cases. Once Teflon sheath is removed, a 6F guide can accommodate: Driveshaft + coronary wire, Driveshaft + Caravel microcatheter, Driveshaft + Corsair/Turnpike LP microcatheters, Driveshaft + 2.5-4mm balloons
9) Combine subintimal ballooning and GE over driveshaft and pull. Only these maneuvers requires ping-pong guides.
10) Call surgeons.
We had a case of abrupt vessel closure after DCB. DCB is a hot topic, but we should prepare for complications. we went with a hybrid DES & DCB strategy. Post-DCB results were good, but when we removed the wire, there was acute vessel closure. We weren’table to cross into TL.
Summary of all Late-Breaking Trials at #ACC2026 – take home points
@ACCinTouch@ACCmediacenter@JACCJournals
1. HI-PEITHO: Ultrasound-facilitated catheter-directed thrombolysis led to a lower risk of PE-related death, cardiopulmonary decompensation or collapse, or recurrence of PE. vs anticoagulation alone in intermediate-high risk PE.
5th cardio ICU with 15 beds dedicated for treatment of Decompensated Heart Failure only. opd follow up also will be here. They get enlisted for transplant from here. During acute decompensation they can bypass emergency department queue and come straight here. Awaiting ECMO
1/ 🚨 Heart attack fact that could save lives: Most people think if chest pain started >12 hours ago, it's "too late" for emergency angioplasty (primary PCI).
WRONG.
Evidence shows PCI STILL helps many late presenters (12-48h). Don't give up!
#STEMI#CardioTwitter
#JADEL
I've read about this.
I know this exists.
But, I still never thought I'd see it:
Now in CASE @CASEfromASE (now in SCOPUS)
Must read: https://t.co/e8zOOfwENY
A. Bridge
B. Anomalous
C. SCAD
D. Other
Follow thread for the Echo, CCT, CMR & OR findings ...
@ASE360
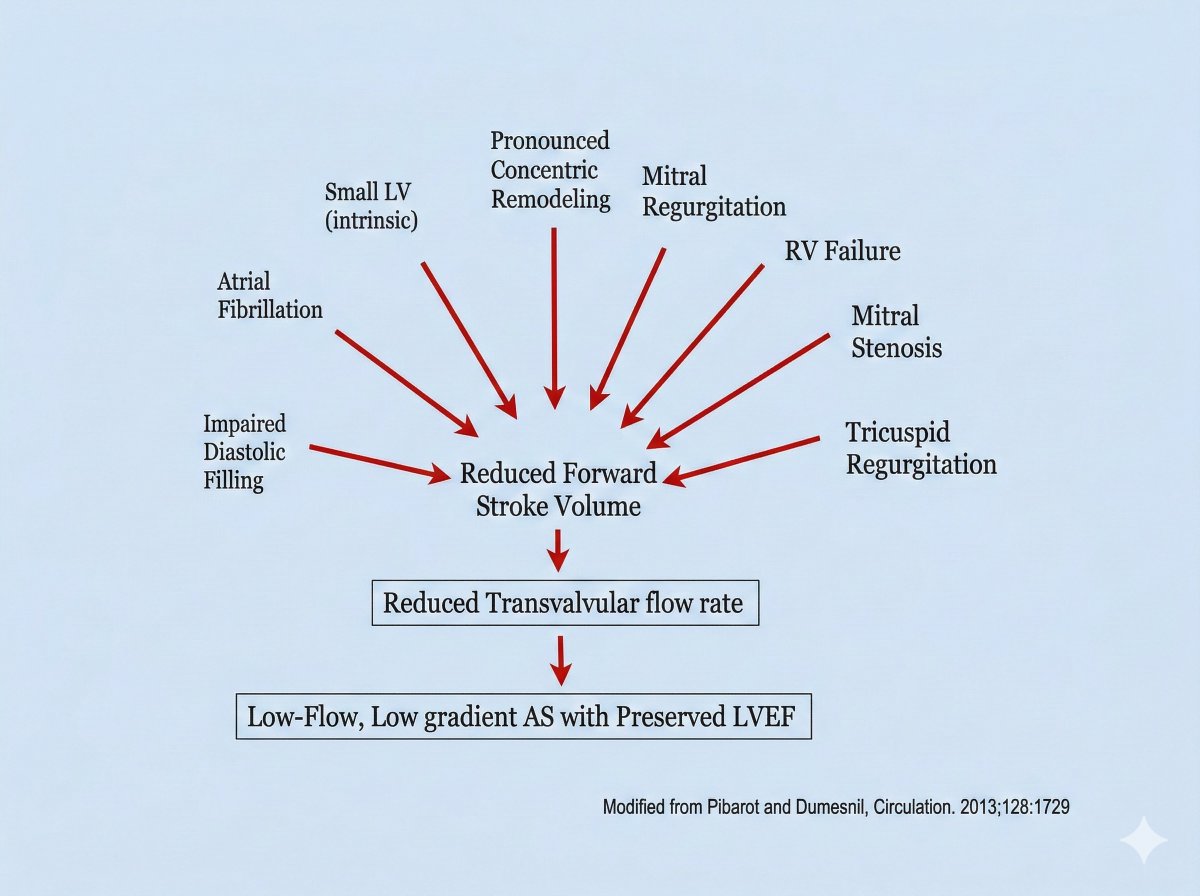
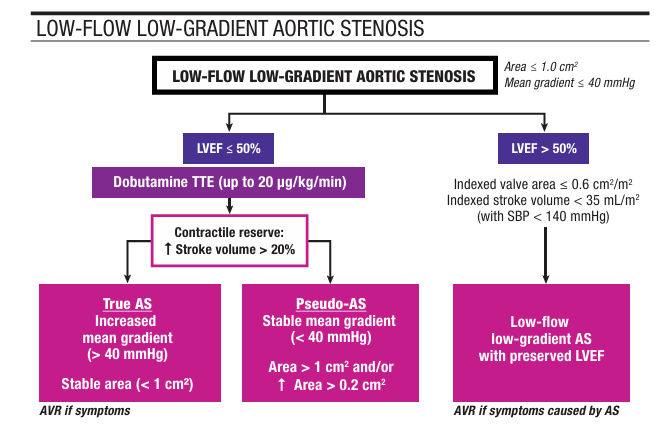
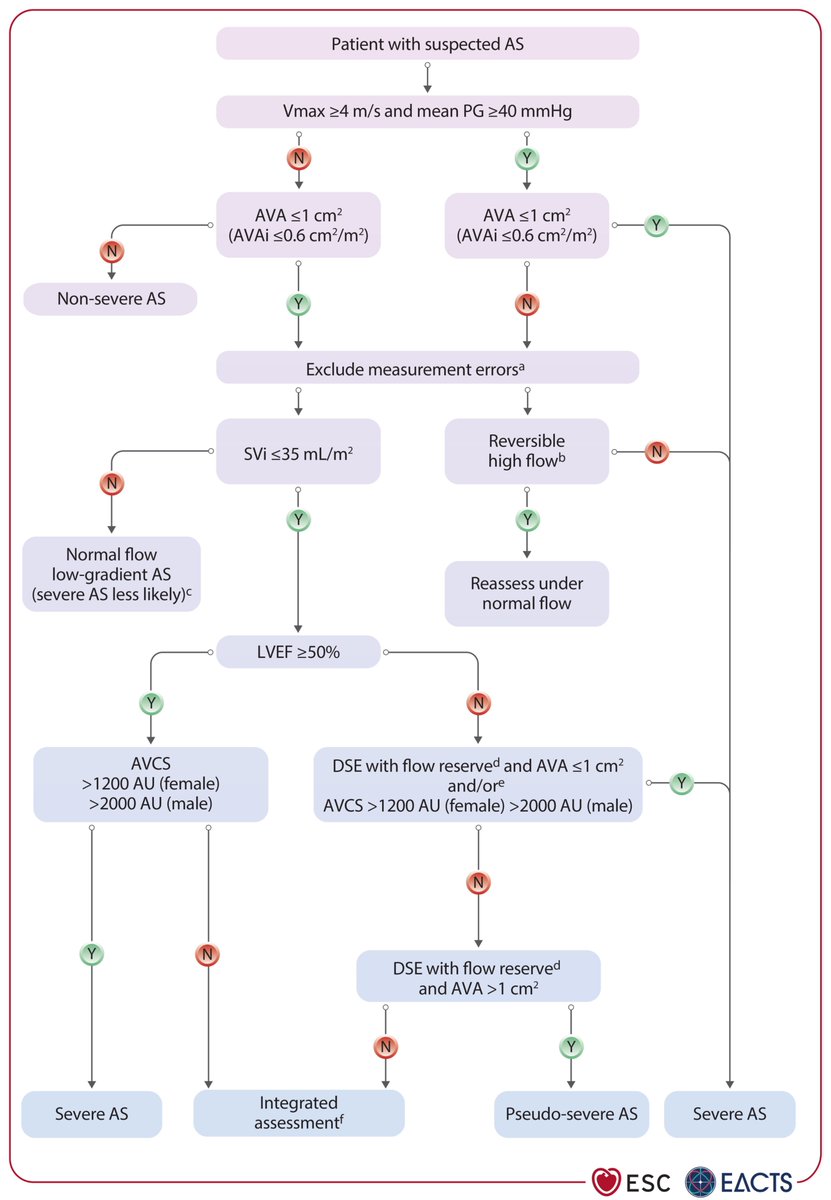
Simplified evaluation of Aortic Stenosis by @escardio including few tips!
1. Grading rely on gradient, velocity, stroke volume index (SVi) and effective AVA.
2. Concordant: High gradient = Severe AS.
3. Discordant:
🔹Low flow, low gradient (LFLG) AS with reduced EF ➡ DSE to discriminate between pseudo/ true severe AS.
AVCS also helpful for those who do not (or cannot) exhibit increase flow on dobutamine echo).
🔹LFLG with preserved EF
Check for measurement errors,
index AVA to BSA (Severe AS: AVAI<0.6cm2/m2),
look for other causes of symptoms (why low flow?).
🔹Normal flow, low gradient AS with preserved EF = usually moderate stenosis (severe AS less likely).
Find out how to scan patients with AS here: https://t.co/S8DMSwKQSA
Now You See It, Now You Don’t! 😳🤔😀
70 M with AW MI last summer. Referred for proximal LAD #CTOPCI.
Our #contrast1st injection showed a microchannel → #HDR not needed! We crossed with an XT and an MG.
What is going on with the LAD here? 🧐
Poll below. Comments welcome!
Uncrossable lesions – my practical pearls
•When the wire crosses but nothing else does, think tight calcium ring + inadequate support (most common issue). If a guidewire has traversed the lesion, a true channel likely exists.
•Grenadoplasty / contrast injection through the microcatheter (after 014 sacrificing if you decided for it) can help to
a) document the wire path,
b) lubricate the channel, and
c) clear loose debris often enough to convert an uncrossable lesion into a crossable one.
d) dig MC inside the lesion (uncrossable point), quickly sacrifice your 014 wire position and get Rotawire down quickly just after 014 removal (incredibly Finecross is great to align Rotawire with virtual channel created by your 014 passage)
Rotational atherectomy tips (when appropriate):
•Prefer Rotawire Floppy (Floppy has a shorter radiopaque marker 22mm vs 28mm - ES version) you just need pass radiopaque segment and enable burr to reach uncrossable point. Better now with Rotawire Drive 1:1 torque response.
•Cut/shorten the radiopaque segment if needed → sometimes all you need to enable burr to reach uncrossable point
•Keep the wire straight or with a very gentle tip, avoid aggressive bends.
•Rotate the wire during advancement (I like drilling technique to advance rotawire).
•Start with a 1.25/1.5 mm burr in most uncrossable CTO scenarios often sufficient to crack a circumferential Ca ring and allow device passage (maybe the last indication for 1.25 burr in my lab). Sometimes if wire isn’t totally deep inside, ablate uncrossable point and retry MC and balloon, then after device crossing re-do a more extensive ablation.
🧵 Perioperative Anticoagulation
This is one of the hardest decisions in medicine.
Stopping too early increases clots.
Stopping too late increases bleeding.
This thread simplifies everything.
#MedTwitter#FOAMed