🩸 Bleeding on anticoagulation is NOT a complication… it’s a turning point
⚠️ The problem
We prescribe anticoagulants to prevent:
👉 Stroke
👉 MI
👉 VTE
But the most frequent complication is:
👉 Bleeding
And here’s the uncomfortable truth:
> Bleeding often determines prognosis more than thrombosis
🧠 Why this matters
Bleeding is NOT just an event.
It triggers:
❌ Treatment interruption
❌ Fear-driven underdosing
❌ Permanent discontinuation
👉 Leading to ↑ stroke, ↑ MI, ↑ mortality
🔥 Key clinical reality
📊 Major bleeding:
~1-3% per year
30-day mortality >15%
1-year mortality >25%
👉 That’s NOT benign
⚖️ The real battlefield
Every anticoagulated patient lives here:
👉 Thrombosis vs Bleeding
And we often focus on only one side.
🧠 What experts are telling us (ESC)
This is the new paradigm 👇
1️⃣ Risk is dynamic
Bleeding risk is highest:
👉 Early after starting anticoagulation
👉 In elderly / multimorbid patients
👉 Reassess continuously, not once
2️⃣ Not all bleeding is equal
🚨 Critical sites = high mortality:
Intracranial
GI
Retroperitoneal
Pericardial
👉 Even small volumes can kill
3️⃣ Combination therapy is dangerous
👉 OAC + antiplatelet = 2–3× ↑ bleeding
✔️ De-escalate EARLY
✔️ Avoid triple therapy when possible
4️⃣ Prevention is powerful
Simple interventions:
✔️ PPI for GI protection
✔️ Avoid NSAIDs / SSRIs when possible
✔️ Correct dosing (DOAC underdosing = worse outcomes)
👉 Most bleeding is preventable
🚨 When bleeding happens
Think in 3 steps:
🩸 1. Stabilize
Stop anticoagulant
Airway, oxygen, access
Fluids + transfusion
🧪 2. Reverse (if needed)
VKA → PCC + Vitamin K
Dabigatran → Idarucizumab
FXa inhibitors → PCC (± Andexanet)
🔎 3. Find and control the source
Endoscopy
IR embolization
Surgery
⚠️ The biggest mistake
> “Let’s stop anticoagulation and never restart”
🧠 The evidence says:
👉 NOT restarting = ↑ stroke + ↑ death
✔️ Restart early when safe
✔️ Individualize timing + dose
🔄 The future
We are moving toward:
👉 Personalized anticoagulation
👉 Dose tailoring
👉 Drug selection based on bleeding profile
🎯 Take-home message
Anticoagulation is NOT binary.
It is:
👉 A continuous balance
👉 A dynamic decision
👉 A personalized therapy
🤓 Final thought
> The goal is not to avoid bleeding
The goal is to survive both bleeding AND thrombosis
📚 Reference
Galli, M., Simeone, B., ten Berg, J., et al. (2026). European Heart Journal: Acute Cardiovascular Care.
https://t.co/dovWgN9BEu
Exciting news — Registration is now open for PERT Consortium's 12th Annual Pulmonary Embolism Scientific Symposium 2026 Annual Meeting
Thursday, October 1 – Saturday, October 3, 2026
Join us at the Marriott Copley Plaza in Boston, Massachusetts — we can't wait to see you there!
Register by May 1 to secure the Early Bird Special pricing. 🐦 https://t.co/UM2sMEOTZN
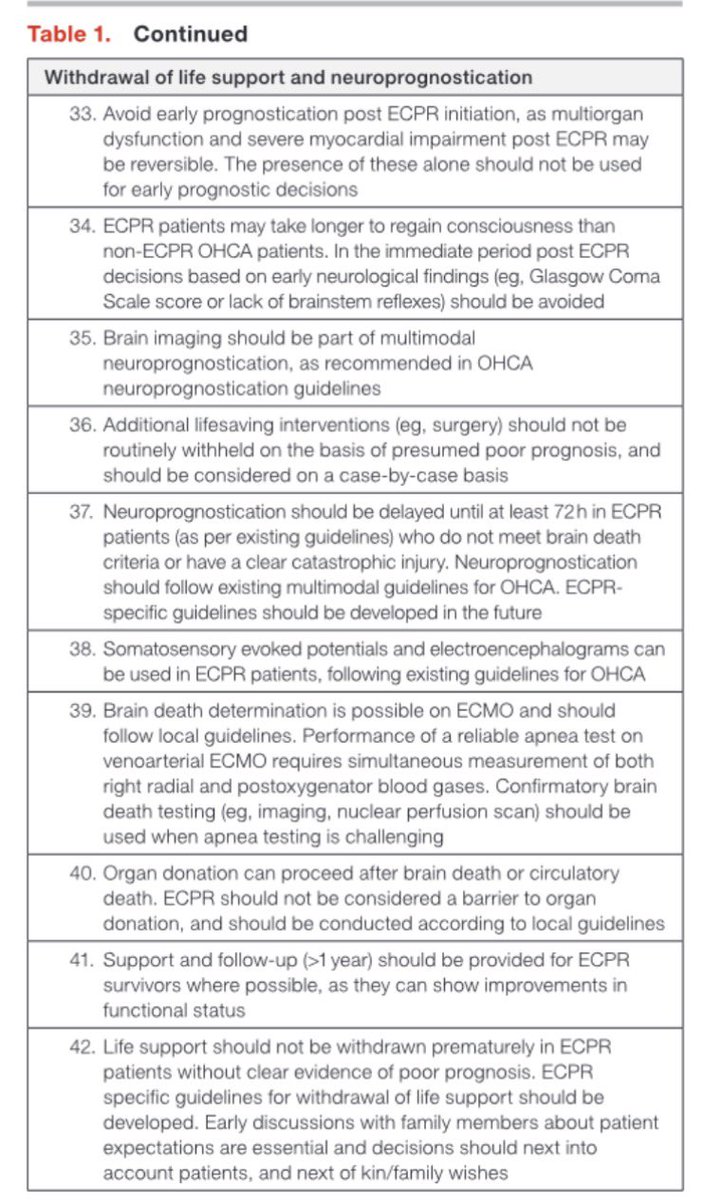
Post-resuscitation care after #ECPR is a key frontier in extracorporeal life support. This new international consensus in @JAHA_AHA provides structured guidance for this complex phase of care. Glad to have contributed as a member of the expert panel #ECMO
https://t.co/1rdGBREyHQ
Join the PERT Consortium Trainee Council!
If you're passionate about shaping the future of VTE care, collaborating with PERT leaders and driving meaningful change, apply today — Deadline is March 2nd!
https://t.co/znJ70ioE0C
@NaviKaurMD@accpchest Had a fantastic first time at #CHEST2025 with my mentor and coresidents! Super grateful for the opportunity to present some interesting cases this year
#CHEST2025
✅ Great sessions on PoPH
💡HPS can be cured by liver transplantation
💡With current era’s PH mgmt, non-severe PoPH (mPAP<45 mmHg) pts can be optimized for liver Tx
💡Dr. @OSitbon - perhaps a future for liver transplantation for mgmt of POPH..?
Dr Namita Sood presented such an interesting clinical case of a patient with PE causing hemodynamic collapse needing VA ECMO. To wrap up the PERT session. The patients journey was a rollercoaster! It was such an engaging discussion, loved how involved the crowd was at #CHEST2025
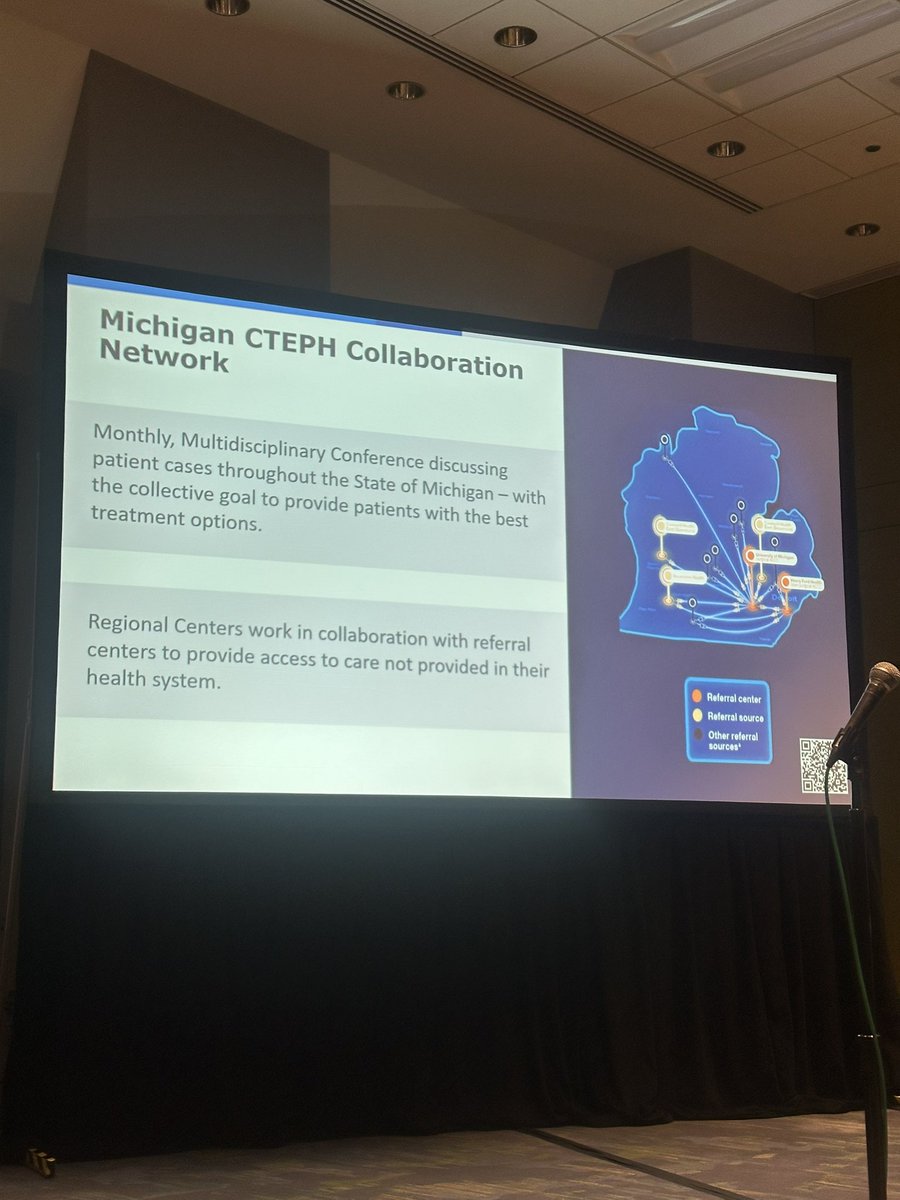
@DrHooksDO shared a fantastic infographic at #CHEST2025 PE is the third leading cause of mortality worldwide, his work with the Michigan CTEPH collaboration network is inspiring for #PERT programs!
@DrHooksDO sharing a fantastic infographic slide at ##CHEST2025 PE is the third leading cause of mortality, his involvement in the Michigan CTEPH collaboration network is an inspiring addition for #PERT programs nationwide