Proud to share ARCH-ARC out today in Circulation 🔥 The endo arch world is moving FAST — branched/fenestrated devices, ascending endografts, total arch without sternotomy. We needed a framework to keep up. First-ever standardized endpoints for thoracic aortic arch trials: new aortic-specific neuro endpoints including structured neurocognitive testing, delirium protocols & spinal cord injury grading. A modified Type A Dissection Classification system to clarify arch involvement. A framework for multi-specialty collaboration. Real outcomes for real patients. It was a privilege to lead this alongside @AWBeckMD and couldn't be prouder of what this incredible international team built together 🫀🚀 #AorticSurgery #TEVAR #ArchARC
https://t.co/yztyom2U6X
Until now, physicians using AI in clinic had to assemble the patient’s context themselves. Allergies, comorbidities, medications, prior procedures, copy-pasted in from the chart.
Today we’re announcing a partnership with @CedarsSinai. OpenEvidence now works directly inside Epic, drawing on the patient’s full record and interpreting the medical literature through the lens of that specific patient.
Cedars-Sinai is the first academic health system to deploy patient-aware clinical intelligence at enterprise scale. The clinician asks a complex question in natural language. The answer reflects both the best available evidence and the patient in front of them.
Patient data is never stored after the clinical session or used for any other purpose.
🤖 AI in ruptured AAA repair?
This case shows Cydar Maps successfully integrated preop CTA with live fluoroscopy during emergent EVAR for ruptured AAA, with potential to reduce contrast, radiation, and procedure time
👉 https://t.co/VWtIkkH60Q
#AortaEd#EVAR#AI#RupturedAAA
George Tolis: TAVR, Broken Training, and What's Really Wrong With Cardiac Surgery.
Dr. George Tolis, section chief of coronary and general cardiac surgery at Brigham and Women's Hospital, joins Drs. Koka and DiGiorgio for a wide-ranging conversation on the state of cardiac surgery. He makes the case that TAVR — while genuinely transformative for the right patient — is being systematically applied too broadly, driven by industry incentive and the erosion of meaningful surgical consent. He discusses his collaboration with John Ioannidis that found no statistically significant mortality benefit for any new cardiac surgery technique introduced over the past 35 years, the paper's rejection by every major surgical journal, and what he paid out of pocket to make it open access. The conversation moves to the collapse of surgical training — fragmented pathways, work hour restrictions that leave residents unprepared for attending life, an academic promotion system that ignores teaching, and a culture that routes incompetent trainees around rather than out — and closes with a brief on Vasily Kolesov, the Soviet surgeon from Leningrad who performed the world's first documented coronary bypass years before Favaloro, and whose work was buried by the Cold War.
Chapter Markers
00:00 Introduction
01:02 Air-cooled VWs, concert piano, and how Dr. Tolis got here
02:40 TAVR: genuine breakthrough or being abused?
08:02 Finding the TAVR threshold — and why informed consent is the real problem
11:46 Collaborating with John Ioannidis: no mortality benefit for 35 years of new techniques
20:02 Why the major surgical journals wouldn't touch the paper
21:52 Minimally invasive surgery: minimal access vs. minimally invasive
26:24 When do CABG survival curves diverge — and what does it mean?
30:05 Surgeons signing off on TAVRs in young patients
33:51 Health system economics and the heart team dynamic
37:50 How to actually pick a good surgeon (ask the scrub nurses)
40:36 Cardiac surgery training: the three pathways problem
44:04 Work hour restrictions and the residency simulation gap
51:16 General surgery is like MTV — they don't operate anymore
53:21 A resident who finished training without ever applying a cross-clamp
56:34 How to evaluate if a program actually trains
59:27 Academic promotion has nothing to do with teaching
01:01:33 Dr. Tolis's resident outcomes database and three papers nobody cared about
01:05:32 The training timeline: finishing at 49, no runway left
01:07:08 One-size-fits-all RRC rules for cardiac surgery and psychiatry
01:09:16 Cardiac surgery as a disposition, not a therapy
01:12:24 When ECMO becomes the final common path
01:13:38 How you become nationally recognized without being a good surgeon
01:17:16 Vasily Kolesov: the Soviet surgeon who did the first bypass
Co-Host Handles
@anish_koka and @drdigiorgio
Show Handle
@drsloungepod
Subscribe Links
Spotify: https://t.co/kjCqkhbBII
Apple Podcasts: https://t.co/n4BVmyAo9p
YouTube: https://t.co/p6yg15EQrw
"Despite similar access to advanced medical
technology, the US has experienced persistently higher death rates than other high income countries"
https://t.co/iIe8UJbUCs
#TechniquesThursday: Robotic-assisted bronchoscopy in dye localization in thoracoscopic pulmonary nodule resection. Read the promising results that researchers say warrant further validation in larger randomized trials in #JTCVS Techniques: https://t.co/DKBq3mGNPk
In a new Perspective, Jatin M. Vyas, MD, PhD, argues that today, the covenant between U.S. academic medical centers (AMCs) and society is under strain: corporatization and the mandate to maximize profits threaten the AMC ecosystem and harm medical training. Read the latest Perspective in the Corporatization of U.S. Health Care series: https://t.co/5dOZmmeC6l
This article discusses a #vascularsurgery resident's efforts to develop a computer vision–based AI training platform designed for environments where traditional surgical education models are simply not feasible. Read more here: https://t.co/7qvb0PoxdI
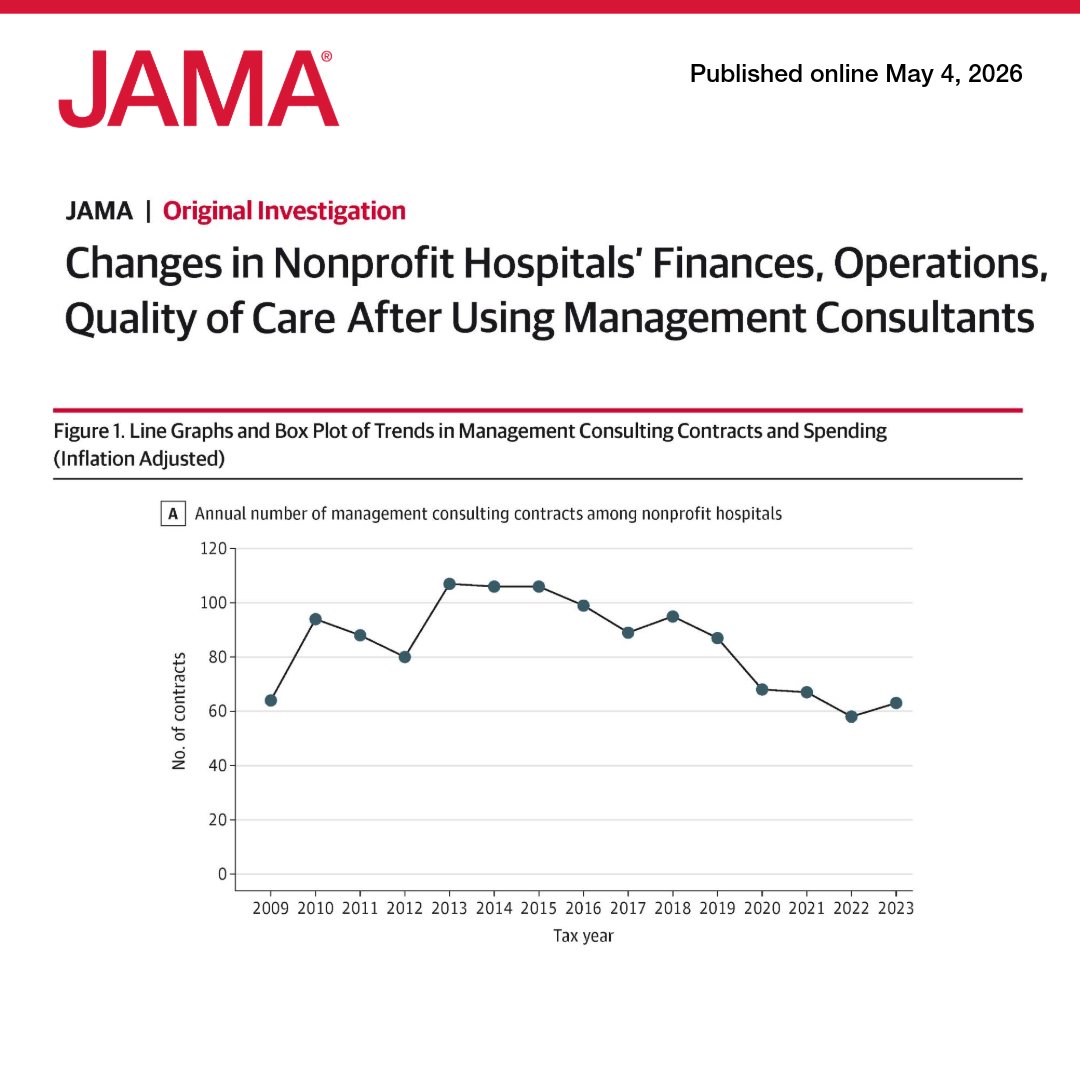
US nonprofit hospitals spent $7.8 billion on management consultants from 2009 to 2023, but contracts were not associated with meaningful changes in finance, operations, or quality of care. 🧵
https://t.co/QQswMYxrG8
A Mayo Clinic-developed artificial intelligence (AI) model can help specialists detect pancreatic cancer on routine abdominal CT scans up to three years before clinical diagnosis. It identifies subtle signs of disease before tumors are visible, when curative treatment may still be possible. The findings, published in Gut, mark a milestone in Mayo Clinic's multiyear research effort to enable earlier detection of one of the deadliest cancers.
Learn more: https://t.co/EJySSkaW3P
Who has the best understanding of the health care system? A physician.
@DrDiGiorgio, a California neurosurgeon, told the Texas Legislature today about some of the greatest inefficiencies facing our health care system:
✔️Fifty-seven clicks to order an MRI.
✔️Clicking through five warning screens to look at a patient's image.
✔️ Two hours on the computer for every hour of patient care.
"Death by a thousand paper cuts."
Thanks to the Texas Legislature for listening to the experts like @DrDiGiorgio. We look forward to the next steps on affordability.
Superhuman interpretation AI for medical images, such as mammography and endoscopy, has been proven to improve diagnostic accuracy in multiple randomized trials but mostly not implemented.
But LLMs for clinical decision support have little real world medicine proof, but are getting widely used.