1/
A 45 yo W presents with a headache that is worse with lying down.
MRI 👇
She is becoming progressively more somnolent.
What do you do:
Drop a stat EVD?
Give some mannitol?
Start Dex 4Q6H and call it a day??
A #ContinuumCase
@msiuba discusses all things pulmonary hypertension at #HR24
Here are some of my biggest take homes including a simple management approach he beautifully outlines👇
My favorite point though... most (almost all!) PH patients do NOT need fluids and need fluid removal when decompensating.
---------------------------------------------------------
2022 Classification of PH
mPAP>20
Precap PVR > 2
Postcap PAWP > 15
Combined: elevated PVR and PAWP
Lecture's Focus - not on the garden variety group II/III
Focus on severe precapillary (PVR > 5) or
any PH with significant RV dysfunction or
patients on vasodilatory therapies.
Cautionary Notes
1. Rare diseases often need expert opinions - contact their PH provider/center.
2. You CANNOT stop the pulmonary HTN therapies, even if hypotensive and hypoxemic. Talk to a PH specialist. If on IV/SubQ therapies you need to get this sorted with pharmacy. No oral intake, need an enteral tube.
Early Goal Directed Palliation Consideration
Where are they on their disease process? Functional?
High risk of PPV
CPR unlikely beneficial
Candidacy for transport and ECMO?
Partial List of Causes of Decompensation
1. Volume overload part of the problem until proven otherwise
2. Infection (indwelling lines?)
3. Arrythmias - 30% of CO from atrial kick can be devastating for this population
4. New VTE
5. Treatment nonadherence
Diagnosis
Physical Exam Features to look for
On IV therapies might have a lot of blushing and asymptomatic hypotension (SBP 80s). Ask what is your baseline?
Perfusion exam is the most important - cap refill, UO, mental status. Can be confounded a little bit by flushing of the skin.
Filling pressure - JVP vs. ultrasound
Peripheral Edema
POCUS Parameters to focus on
LVOT VTI, Portal vein pulsatiity, and RVOT VTI valuable as these reflect the current state of affairs, and not chronic features (e.g. chronic RV dilation). Portal vein pulsatility a reliable marker of congestion in PH patients (@ArgaizR has done some of this work)
Don't rely on.... IVC or TR severity. Not really helpful!
Management and Treatment Goals
Many PH patients will never have a normal LVOT VTI... hard to normalize often.
1. Preload optimization --> almost certainly reduction. The idea that PH needs volume as a rule is FALSE. MOST NEED REDUCTION.
2. Afterload optimization - keep normal pH, SpO2, CO2 etc. Inhaled pulmonary vasodilatiors.
3. Contractility optimization. They love sinus rhythm. Consider cardioversion early. Maintain SBP > RV systolic pressure (to maintain coronary prefusion). . Inotropes as needed.
Keep in mind transplant candidacy throughout.
#medtwitter #echofirst #cardiotwitter #cardio #meded #foamed
(1/6) Goals of care conversations look different depending on your setting (e.g. ED vs ICU) but all share some common features.
A 🧵 on my approach to goals of care conversations that explores functional status, patient values, and then uses clinician medical expertise to provide a recommendation.👇
#medtwitter #foamed #foamcc #meded #education
What were the top papers in Emergency Medicine in 2023? Here is summary from Vancouver General Hospital Grand Rounds w/ Dr. Shari Li. 🧵 to follow! Let me know what you think, and which papers we missed! #FOAMed#FOAMcc@EmergencyCareBC@CAEP_Docs@EMResUBC@WeAreCanadiEM
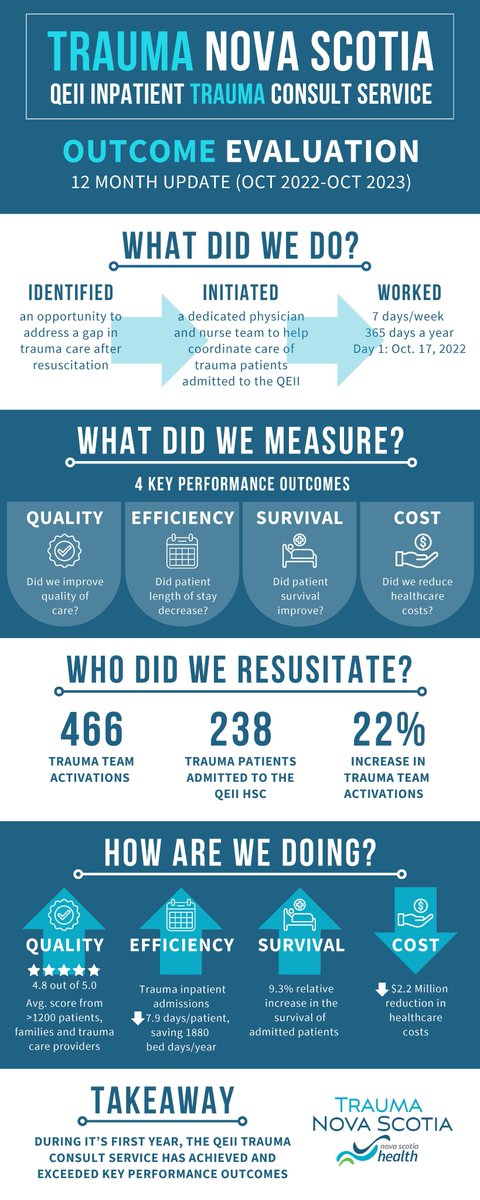
We are 1 year old! Our Trauma Consult Service just passed the 12 month mark, and our outcomes are better than expected. Very thankful for the dedicated work from our clinicians who have made this happen.@nshealth@Doctors_NS@HealthNS@TACTraumaCanada
Thank you #EACEM2023 for the opportunity to speak on the management of the massively bleeding trauma patient.
While I could only join virtually, I hope to join you all in Turkey in the near future.
In case you missed it...here's some highlights:
1/
“CPR has become an expectation rather than an exception, a treatment meant for a few but applied to all,” @SunitaPuriMD writes. https://t.co/1QS6i9YbMM
Very well written! IMO, We must role model excellence, #Payitforward Being valued for our excellence as a clinician/researcher/educator/leader, being authentic in the pursuit of life-long learning, being brave & choosing not to do something merely to check a box & holding one another accountable particularly as we rise to positions of power…these are some antidotes to #Burnout
As an intern, one of the highest-yield schemas I learned was for persistent fevers despite treatment with abx.
I use it all the time as a resident, especially when working with cancer patients.
Let's go through it!
- Thread -
#MedTwitter#MedEd#FOAMed#tipsfornewdocs
1/24
A man comes to the ICU after uncomplicated cardiac surgery. He is hypertensive and a nicardipine infusion is started. 10 minutes later he becomes hypoxemic. A chest radiograph is obtained.
What happened?
1/
I understand why this necessary WAITING space has been added…. And it is good that it has.
But ultimately not having admitted pts in the Peds ED (rather up on dedicated resourced wards) and LESS kids waiting for care should be the goal.
Way back Wednesday!
We see a lot of hypertension in the ED, especially as access to GPs becomes harder. What should the standard approach be? When do patients need investigations?
Dr. @emmaksferguson has an EXCELLENT approach to refine your practice: https://t.co/Oan0fBQ7fD