Terlipressin is to the portal circulation what norepinephrine is to the systemic one — precise, powerful, and now, with continuous infusion, safer and smarter than ever.
Terlipressin – Old Molecule, New Directions in Cirrhosis Care
(Based on Hepatology Communications, April 2025)
🧬 Essence
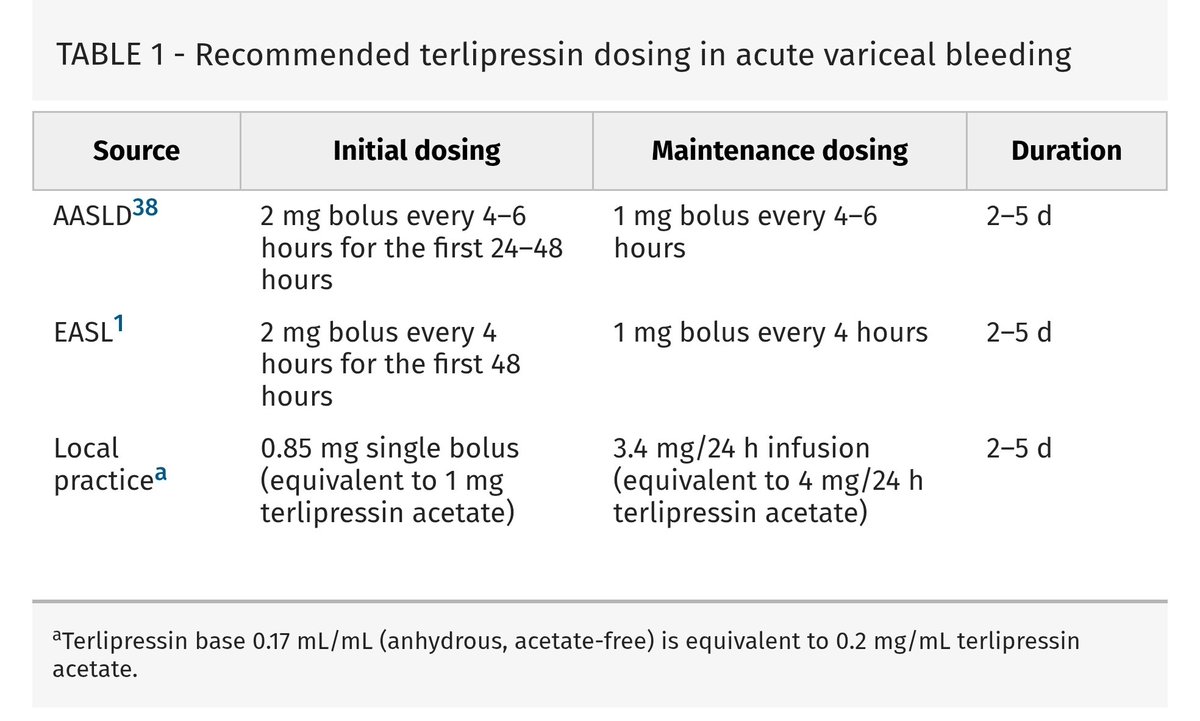
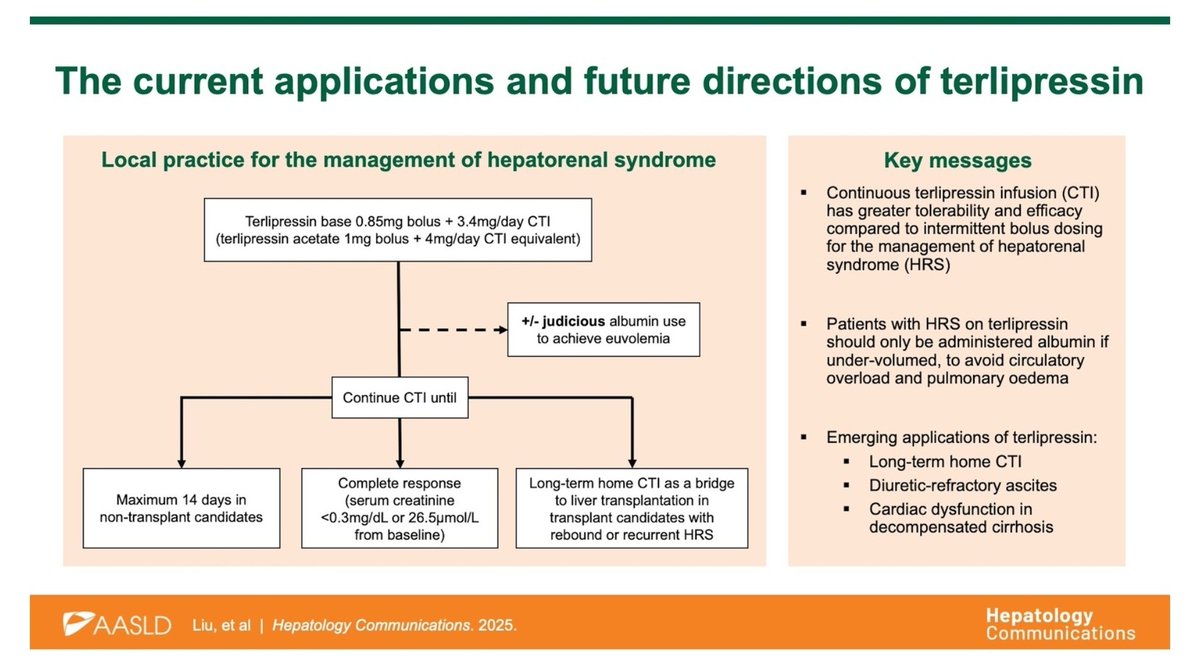
Terlipressin is a potent vasopressin analog that selectively constricts the splanchnic circulation, reducing portal inflow and pressure. It is well-established for portal hypertensive bleeding (PHB) and hepatorenal syndrome–acute kidney injury (HRS-AKI). The modern shift toward continuous terlipressin infusion (CTI) has demonstrated superior hemodynamic stability and a lower risk of ischemic side effects compared to traditional bolus dosing.
⚙️ Mechanism and Hemodynamics
Terlipressin produces a more sustained fall in hepatic venous pressure gradient (HVPG), a rise in mean arterial pressure (MAP), and a reduction in heart rate, compared to octreotide. In contrast, octreotide’s initial HVPG reduction rebounds within minutes, likely due to rapid desensitization of somatostatin receptors.
Hence, terlipressin maintains prolonged portal pressure control, a key factor in preventing variceal rebleeding and improving systemic perfusion.
🩺 Clinical Roles
Terlipressin remains the cornerstone in acute variceal bleeding and HRS-AKI.
However, emerging evidence supports its use in refractory ascites, hepatic hydrothorax, and as a bridging therapy for liver transplant candidates requiring long-term circulatory support to control HRS recurrence and fluid overload. Continuous ambulatory terlipressin infusions are now being explored as part of home-based management programs for decompensated cirrhosis.
⚖️ Terlipressin versus Octreotide
Octreotide, a somatostatin analog, causes transient splanchnic vasoconstriction by inhibiting vasodilators, but its hemodynamic impact is less durable. Terlipressin, through direct vasopressin receptor stimulation, achieves a greater and longer-lasting reduction in portal pressure and better systemic circulatory support.
Randomized trials involving over 700 patients have shown comparable control of bleeding and mortality between terlipressin, octreotide, and somatostatin when used alongside endoscopic band ligation. However, terlipressin provides stronger immediate control of active bleeding at endoscopy.
Importantly, no study has yet compared continuous terlipressin infusion (CTI) with octreotide for acute variceal bleeding, although CTI is expected to outperform bolus therapy due to steady portal pressure reduction.
⚕️ Safety and Monitoring
Terlipressin can cause hyponatremia, abdominal pain, and ischemic complications in the heart, bowel, or extremities. Continuous infusion minimizes these peaks and troughs in vasoconstrictive effect, thereby reducing ischemic risks.
Close monitoring of serum sodium, urine output, mean arterial pressure, and ischemic symptoms is essential during therapy.
💡 CME INDIA Take-Home
Terlipressin remains the most potent and physiologically rational vasoactive drug in portal hypertension.
Continuous infusion provides stable hemodynamics and improved safety compared to bolus dosing.
Evidence is expanding for its role in refractory ascites and bridging to transplant.
Future trials must compare CTI directly with octreotide to confirm superiority in acute variceal bleeding.
In experienced hands, terlipressin is transforming from a rescue agent to a strategic long-term therapy in decompensated cirrhosis.
🧠 CME INDIA Insight:
Terlipressin is to the portal circulation what norepinephrine is to the systemic one — precise, powerful, and now, with continuous infusion, safer and smarter than ever.
https://t.co/Hwd84Ajuut
Save the date!
Saturday February 28, 2026
The third annual ACTER Advanced Liver Disease Symposium at Austin Health.
By popular demand the theme of next year’s event will be critical care hepatology.