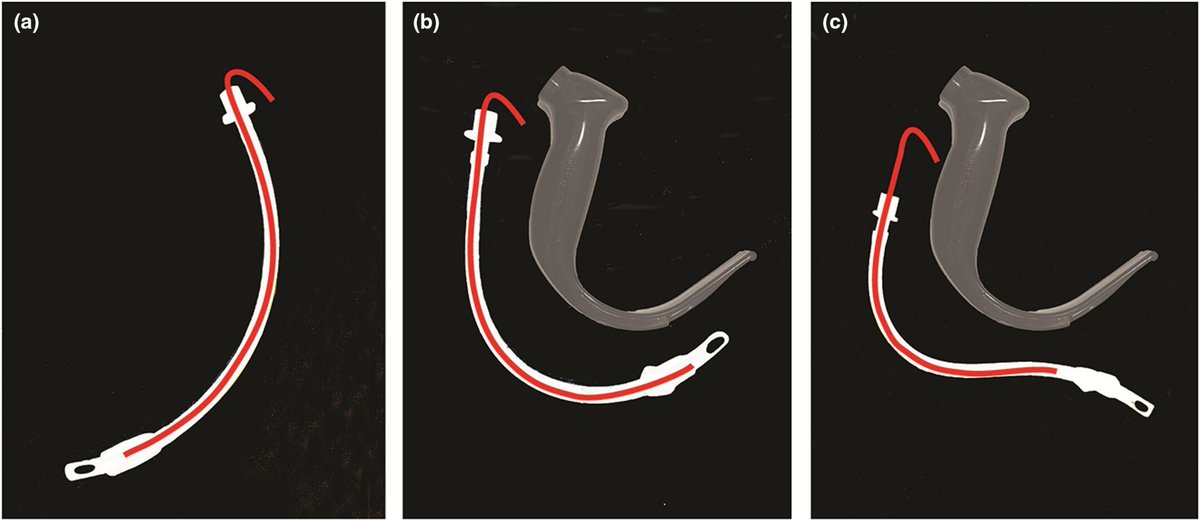
When using a hyperangulated videolaryngoscope have you tried "reverse loading" a tracheal tube on to a preformed stylet?
The stylet & tracheal tube are shaped forcibly in the opposite direction to the normal curvature and to match the shape of the blade.
#anaesthesia #MedTwitter #airway
https://t.co/wOF4wgCXf7
@Shr_Nottingham Pressure and flow. Not great if you have a stonking BP but bugger all flow due to hypovolaemia/vasoconstriction. But broadly agree, as I have a very low threshold for adding vasoactive drugs into the mix. In paeds I think this is far more important than anaesthetic neurotoxicity
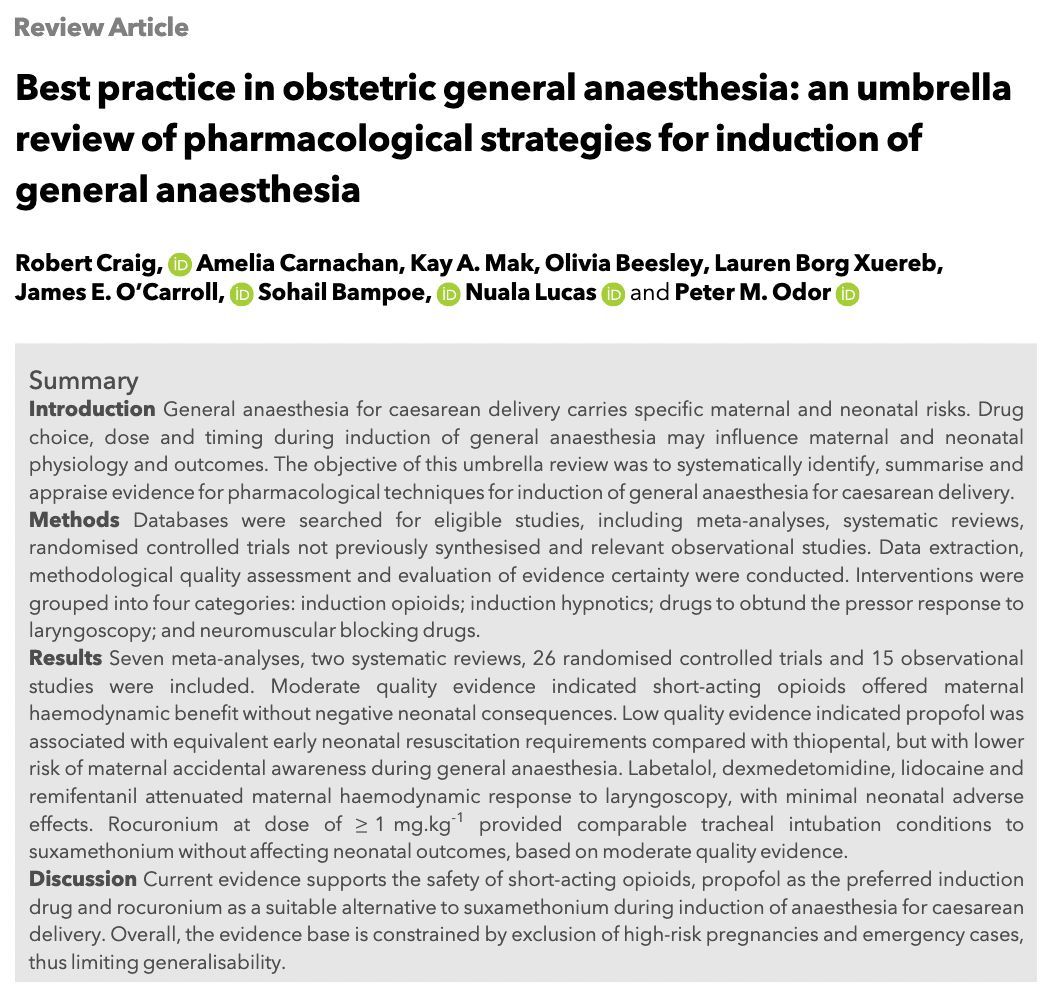
Best practice in obstetric general anaesthesia: an umbrella review of pharmacological strategies for induction of general anaesthesia
#anaesthesia#MedTwitter#obstetrics
https://t.co/IhipO2CnbC
Read a summary of "Intraoperative driving pressure–guided high PEEP vs standard low PEEP for postoperative pulmonary complications," published in JAMA, in the May 2026 Science, Medicine, and the Anesthesiologist: https://t.co/5O1UwTHYJQ
Pressure Volume loops have so much great physiology!
I built a little app to simulate cardiac PV curves and demonstrate how different MCS devices (IABP, Impella, VA-ECMO) alter them.
Try it out: https://t.co/XwBwUL53nE
I'd love to hear your feedback & ideas for improvement!
New guidance on sterile gown use during spinal anaesthesia aims to reduce unnecessary waste while maintaining high standards of patient safety.
Consensus guidelines published in @Anaes_Journal now https://t.co/2gwiMJ3EVJ
With @RCoANews, @OAAinfo, @RegionalAnaesUK, CAI, ANZCA
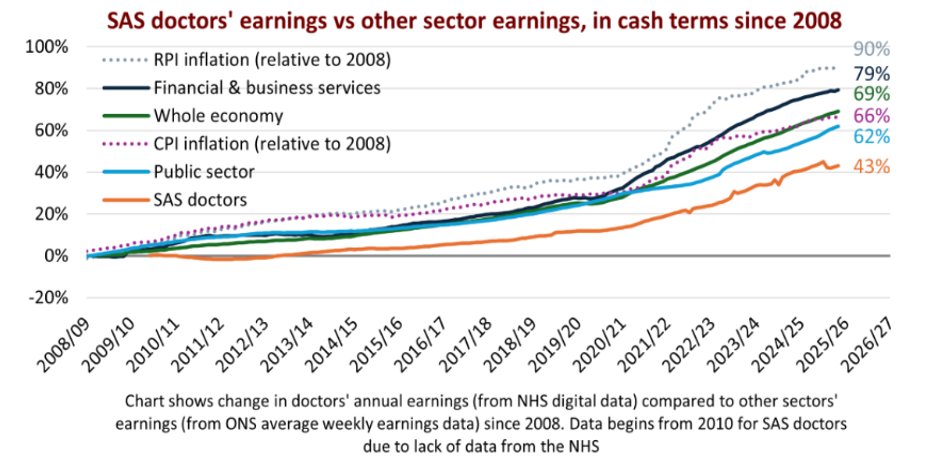
This is why SAS doctors are feeling the pinch. Our pay has not kept up with either the cost of living or with the rest of the economy or the public sector. What felt affordable 10-15 years ago no longer is.
#Ballot#VoteYes@TheBMA@BMA_SAS
@maffygirl@LiangRhea I see, not from Saturday 8am, from Sunday 8am. Similar to what I did during my training and early career. Awful and unsafe if the night is tough (60-70% chance where I worked)
@maffygirl@LiangRhea Well, the longest one I did was 36 hours - from 8am until 8pm next day, but from Sutarday to Monday evening it's 58 hours which beyond crazy. Why 33?
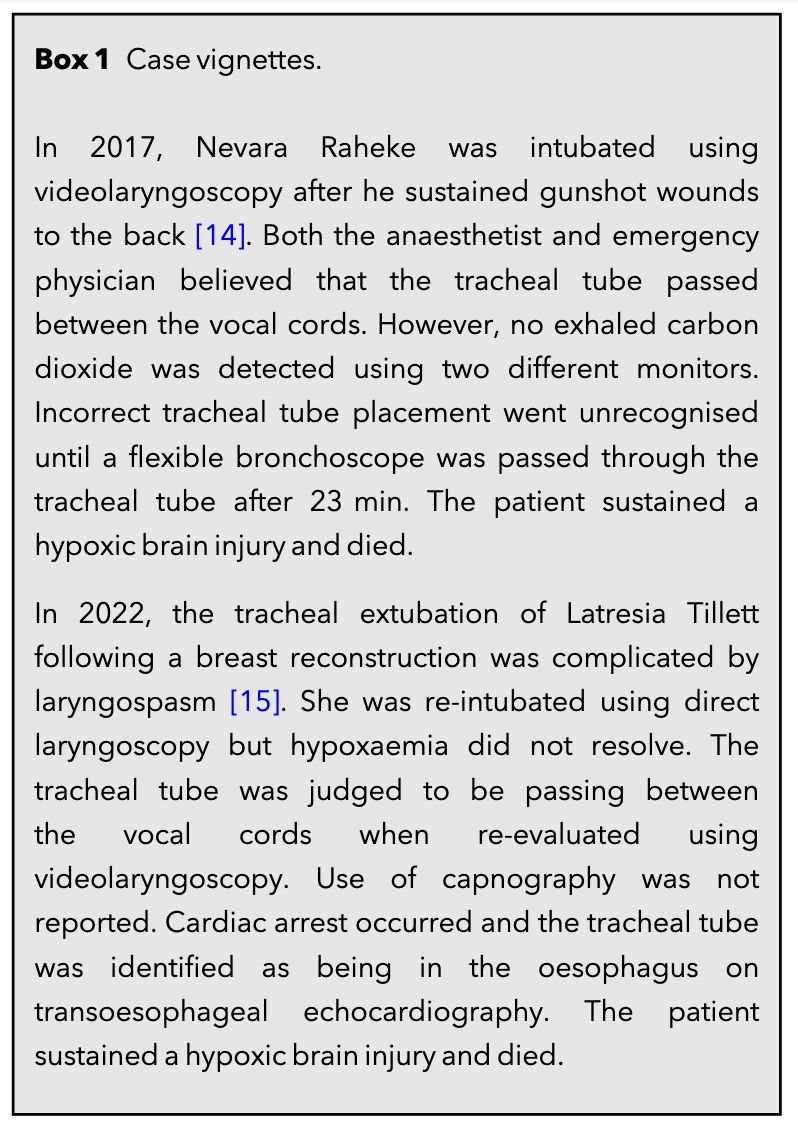
Should you use videolaryngoscopy to confirm tracheal tube location?
Further use of VL to evaluate location could lead to ongoing misinterpretation.
#anaesthesia#MedTwitter
https://t.co/JV9zl4NQee
Medicine is a distinct & elite profession & I’m getting tired of people trying pretend that there’s a shortcut to the years of hard work it takes to become a doctor
Tiered rotas are nothing more than gaslighting patients into worse care
I’m glad it’s being called out publicly
🗳️ RA-UK Council Elections are now open — have your say
6 candidates. Vote for up to 4.
Deadline: 12pm, 8th April
🔹 Dr Toby Ashken
🔹 Dr Boyne Bellew
🔹 Dr Bis Das
🔹 Dr Jenny Ferry
🔹 Dr Kiran Koneti
🔹 Dr Xiaoxi Zhang
Members: check your inbox for your voting link 📩
“How to Survive in Anaesthesia … is a practical companion for anyone interested in, or already navigating, a career in anaesthesia” – new #BJA#bookreview
https://t.co/krtk0bZxBW
When a patient is in the hospital, doctors used to use paper notes to communicate with one another.
In the EHR era, the note stopped being a clinical communication tool and became a billing and compliance artifact. The results have been a disaster.
One JAMA study found notes got 60.1% longer from 2009 to 2018, while redundancy rose 22%. ONC has explicitly acknowledged that clinicians use templates to stuff notes with unnecessary information into the chart to meet billing requirements, creating note bloat.
The clinical note was no longer a method of communication. It was a billing document.
So hospitals layered secure chat on top just to communicate the actual plan of care. And even that workaround is not working.
A 2024 JAMA study found more secure messaging was associated with more time on the phone, not less. Doctors needed to call to clarify the now constant message stream.
Another study found higher messaging volume was associated with higher odds of errors. More messages means a higher cognitive load with most of the information being low-importance. This increased cognitive load leads to more errors.
We took what should have been efficiency improving technology, a computerized chart, and so over-regulated it and misaligned incentives that it has led to harmful downstream effects.
Now, please don't do this with AI...
What’s new in #PaediatricAnaesthesia?
🎙️ Listen to Eva Roofthooft and Arash Afshari discuss the 2025 ESAIC and ESPA Guidelines on neuromuscular block in anaesthetised children, covering indications, monitoring and safe reversal.
https://t.co/UdGMyW3zeZ
#EJApodcast
Speaking about the attacks on a Jewish community ambulance service in Golders Green, BMA council chair Dr Tom Dolphin said: “We are appalled to see this attack on ambulances that provide an important service to people in North London. Anti-Semitism is abhorrent, and deliberate attacks on healthcare services are reprehensible, and this horrendous incident involves both. It is a relief that no one was injured, but this makes the attack no less sickening. Our thoughts are with the Jewish community in North London and across the UK.”