#WATCH | Bengaluru, Karnataka: Dr Devi Shetty, Founder and Chairman, Naryana Health says, "Every Indian, at the age of 17 must get the blood test done. This is the guideline now issued by the Cardiology Society of India because if the cholesterol level is high, they can manipulate the diet and all the men at the age of 35 to 40 should undergo a routine test along with CT scan of the heart. Anyone with the family history of heart disease must go for the checkup at the age of 30 itself, not wait for long time. All the diabetics should go for the checkup even earlier than 30 years. It is important that everyone should know their numbers. They should know what their blood pressure is, cholesterol number is, their heart numbers are. Today we find large number of young people getting into extreme sport. Even if you are very young, 17 or 18, if you are going for extreme sport, you must go for a checkup... The best way to know what the cardiac problems are to the test done. As I said, simple tests which can be done within one hour, once a year. If the CT scan is normal, for the next seven years or ten years you don't need to bother..."
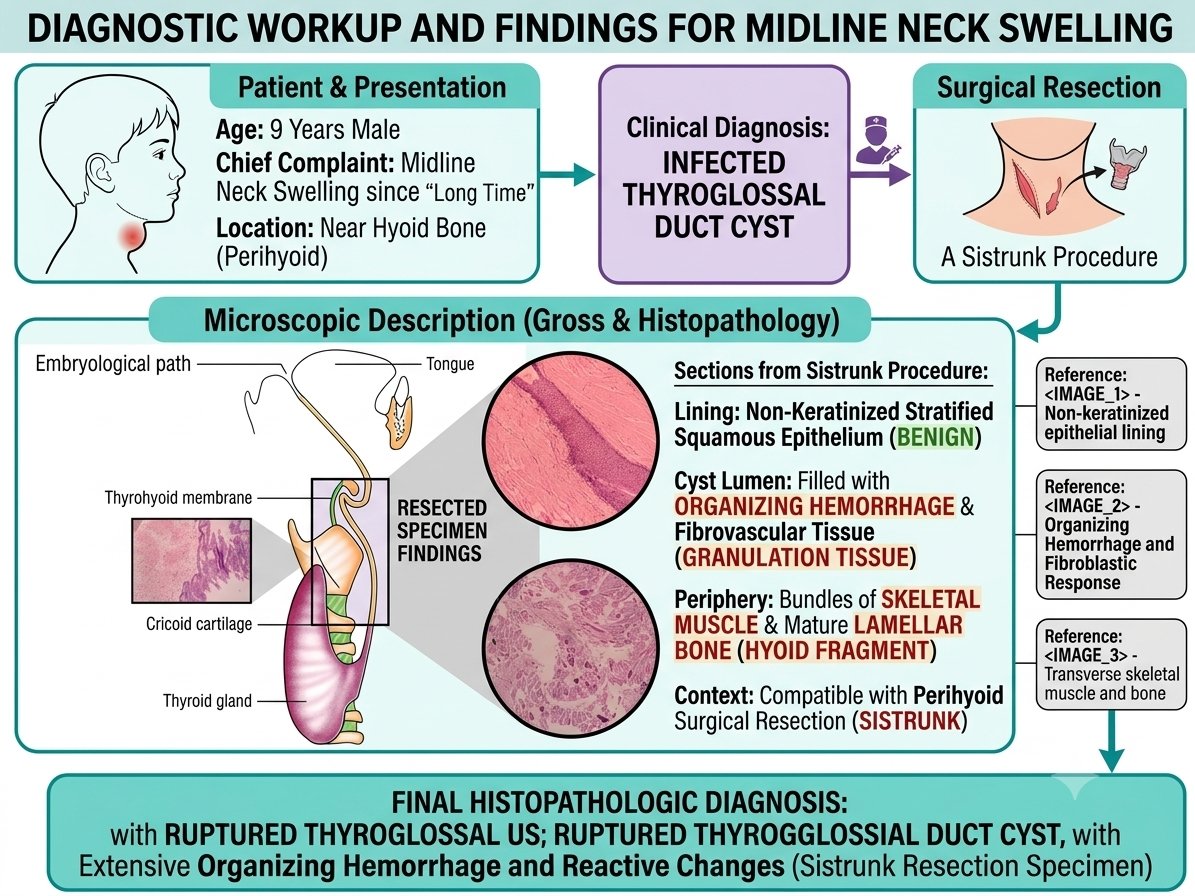
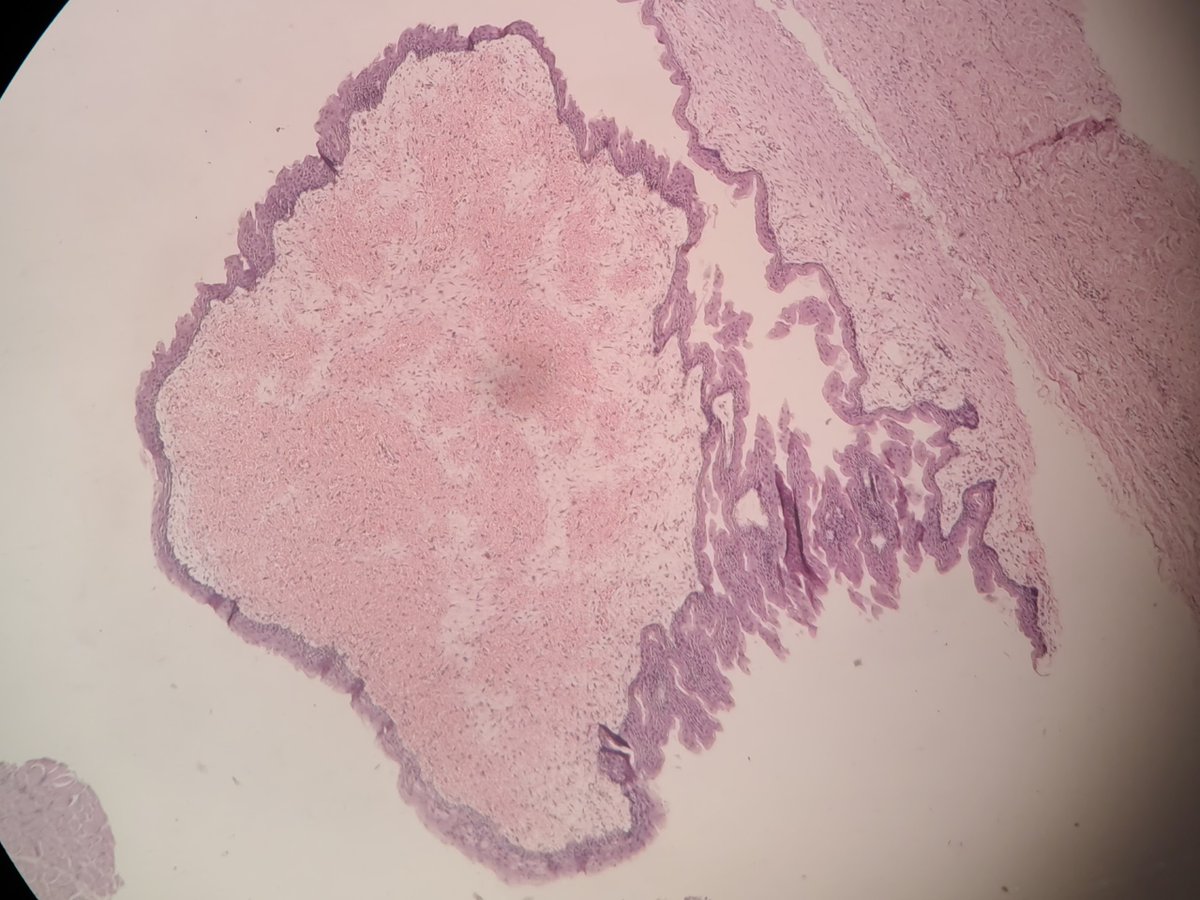
Adjacent fragments of skeletal muscle and mature lamellar bone perfectly correlated with a complete perihyoid surgical resection.
The final histopathological diagnosis was a ruptured thyroglossal duct cyst with extensive reactive changes.
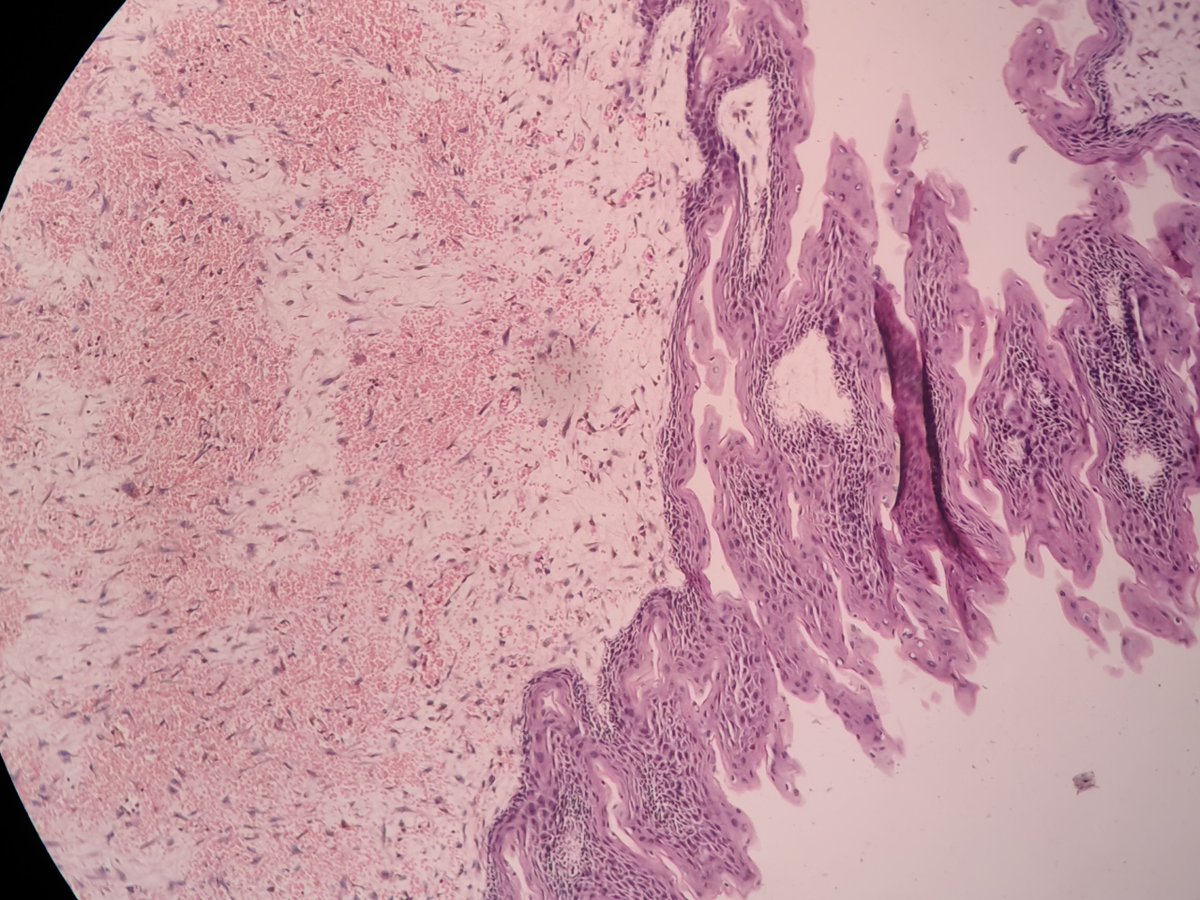
Microscopic examination confirmed a benign, non-keratinized stratified squamous lining. The cyst lumen contained organizing hemorrhage and reactive fibroblastic granulation tissue, indicating a past rupture or chronic inflammation.
#100_करोड़ की लागत से बने रीवा-सतना बाईपास का हाल देखिए
इतनी पतली छड़ डाल दी गई की पूरा बाईपास ही धस गया है 📌
पर इसके बावजूद टोल टैक्स के नाम पर बदस्तूर लूट जारी है
क्या किसी की कोई अकाउंटबिलटी नहीं है 👆
क्या 10 mm की छड़ से बाईपास का ब्रिज बनता है
कहाँ है संबंधित अधिकारी कितने पैसे लेकर लोगो को मौत के मुँह में धकेल रहे है
ये सब कब तक चलता रहेगा हमारी चुप्पी हमारी जान लेकर छोड़ेगी
Car 24 करके एक यूट्यूब चैनल द्वारा एक वीडियो बनाया गया था 0 एथेनाल और E20 तेल डलाकर।
जिसमें साफ दिखा कि E-0 पेट्रोल से गाड़ी का एवरेज 22km/l के आसपास था और E20 पेट्रोल में 14km/l था।
लेकिन अब उन्होंने यह वीडियो गड़बड़ी मंत्री जी के दबाव में वीडियो डीलिट कर दिया है।
Today is National Doctors Day in India. And the best day for me to discuss this very important paper. I will tell you why, at the end of this post.
The BMJ invited me to lead and write an invited editorial with a niche group of medical science communicators on an important topic.
https://t.co/kWPdRNSUbp
One of the most common arguments from the traditional medicine industry to prove the "legitimacy" of their (untested) products and (unscientific) practices in healthcare was that they had been "recognised" by WHO.
Large scale global meetings were conducted by WHO. And countries with emotional appeal towards traditional medical care, while others with political, religious and cultural stakes in the form of business oppurtunities were all part of these WHO-driven meetings were public funds were utilized to plan strategies to justify alternative medicine and promote it.
In this invited review, me, along with fantastic and brilliant medical science communicators - @CaulfieldTim , @Cath77777 , Prof. Xingshun Qi - and a patient-partner discuss, how, some WHO-related strategies, policies and endoresements are not science-related, but mostly politically and culturally motivated.
Please read here: https://t.co/kWPdRNSUbp
4 major points about the risks of rushing alternative medicine:
Lowered scientific tandards: The WHO is pushing to include traditional and alternative medicines into standard healthcare systems. However, they are dangerously lowering the scientific standards needed to prove these treatments actually work, allowing them to be endorsed before standard safety data exists.
Real risks to patients: Rushing to use unproven traditional remedies can lead to serious patient harm, including dangerous interactions with standard medications. Globally, herbal remedies are actually a more common cause of severe liver failure than prescription drugs.
Driven by politics, not science: The growing acceptance of alternative medicine is often driven by politics, nationalism, and economic interests rather than reliable science. Promoting these unproven practices risks spreading health misinformation and commercially exploiting vulnerable patients.
Safety must come first: While traditional practices are heavily relied upon globally, all patients deserve treatments that are fundamentally safe and effective. We must ensure alternative medicines pass the exact same rigorous scientific tests as conventional healthcare before endorsing them.
Today is National Doctors Day in India. Whether is is WHO or any such "legit" monolithic organization directly promoting misinformation and indirectly driving disinformation that can cause public health harm, as doctors, we do not look at the size of different Goliaths we meet. We fight like David, to protect - because that is what doctors who are really teachers swore - took an oath - that Primum non nocere...
..."first, do no harm."
We hope the WHO is listening. And so are the public.
Editorial: WHO’s misguided push for complementary and alternative medicine
https://t.co/kWPdRNSUbp
Something important.
Dear friends, my recently concluded talk is now available to watch on YouTube.
Before I started my session, I put out a disclaimer that alternative medicine practitioners seated in the audience might find my talk extremely triggering. This is one session I thought would be taken down by alternative medicine (Ayush) regulators in India...
...because I do not mince my words at all, about the massive public-fund wastage called Ayush.
For students who are planning to join Ayurveda or Homeopathy or such Ayush-related colleges for professional training... or those parents who are planning to send their children to Ayush - especially Ayurveda-related professional colleges to make a career out of it, this video will mess up your mind - and rightly so.
This is one video, which I would like everyone to watch, share and promote.... especially among those trying to get into alternative medicine colleges in India as a career option because they will be given the title of 'Dr".
Let us stop wasting our childrens future in India by sending them to a career of deceit and fraud - in alternative medicine - just for the legal (but never practical or logical) 'Dr' title.
Sacred Poisons | The Liver Doc | RenaiESSENSE'26
https://t.co/d0GkKVIpnr via @esSENSEGlobal
I'm a cardiologist. After 40, stop guessing about your health. These numbers tell you whether you're building a long, vibrant life — or quietly declining without knowing it.
I run these on myself. I run them on every patient I care about. Most are cheap bloodwork. All are available now. And together, they paint a picture no standard annual physical will ever give you. Print this. Bring it to your next appointment. Your 60-year-old self will thank you.
ꟷꟷꟷ
𝗙𝗮𝘀𝘁𝗶𝗻𝗴 𝗜𝗻𝘀𝘂𝗹𝗶𝗻
Target: below 5 μIU/mL. Ideal: 3-4.
This is the 10-year warning bell your standard panel completely misses. Your glucose and A1c can look "normal" for a decade while your pancreas is working overtime to keep them there. Fasting insulin catches insulin resistance 5-10 years before your A1c moves. By the time A1c rises, the damage is already extensive.
𝗛𝗢𝗠𝗔-𝗜𝗥
Target: below 1.0.
Calculated from fasting insulin and fasting glucose. The single best measure of insulin sensitivity. Above 1.0 and your metabolism is already under strain. Above 2.5 and you're insulin resistant — even if every other number looks fine.
𝗛𝗯𝗔𝟭𝗰
Target: below 5.4%.
Not below 5.7% — that's the threshold where medicine calls you "prediabetic." By then you've been metabolically compromised for years. Optimal is below 5.4%. Blood sugar mastery is longevity mastery.
𝗧𝗿𝗶𝗴𝗹𝘆𝗰𝗲𝗿𝗶𝗱𝗲 : 𝗛𝗗𝗟 𝗥𝗮𝘁𝗶𝗼
Target: below 2. Ideal: below 1.
Your metabolic health crystal ball. This ratio predicts insulin resistance, cardiovascular risk, and metabolic syndrome better than any single lipid number alone. A ratio above 3.5 is a red flag regardless of what your total cholesterol says.
𝗔𝗽𝗼𝗕
Target: below 80 mg/dL for moderate risk. Below 60 for high risk.
I've written about this extensively. ApoB counts every atherogenic particle hitting your artery walls. A 2024 analysis found 54% of patients had dangerous levels that standard LDL testing completely missed. If you only know your LDL, you're driving with one eye closed.
𝗟𝗽(𝗮)
Test once in your lifetime.
100% genetic. 1 in 5 Americans are elevated. Triples heart attack risk independently of everything else on this list. Diet and exercise cannot lower it. The 2026 ACC/AHA guidelines now recommend everyone be tested. Most never have been.
𝗵𝘀-𝗖𝗥𝗣
Target: below 1.0 mg/L.
You can have perfect cholesterol and inflamed arteries silently preparing to rupture. hs-CRP measures the fire behind the plaque. The JUPITER trial proved that finding and treating inflammation saves lives — even when lipids look fine. If this number is elevated, your mouth, your gut, your metabolic health, and your visceral fat are the first places to investigate.
𝗩𝗶𝘁𝗮𝗺𝗶𝗻 𝗗
Target: 50-80 ng/mL.
Not the bare minimum of 30 your doctor accepts. Suboptimal vitamin D is linked to higher inflammation, weaker immunity, increased cardiovascular events, worse mood, and poorer outcomes across nearly every disease I treat. Supplement D3 with K2 — without K2, calcium deposits in your arteries instead of your bones.
𝗧𝗲𝘀𝘁𝗼𝘀𝘁𝗲𝗿𝗼𝗻𝗲 (𝗧𝗼𝘁𝗮𝗹 + 𝗙𝗿𝗲𝗲)
Men: optimal range 600-1000+ ng/dL total.
Declining testosterone is an independent predictor of cardiovascular death in men. It's tied to insulin resistance, arterial stiffness, visceral fat accumulation, and systemic inflammation. DHEA-S drops 10-20% every decade after 30. Tracking these isn't about vanity — it's evaluating your body's systemic resilience.
𝗕𝗹𝗼𝗼𝗱 𝗣𝗿𝗲𝘀𝘀𝘂𝗿𝗲
Target: below 120/80. Aim closer to 110/70.
Every point above optimal is cumulative arterial damage. Buy a home cuff. Measure morning and evening, seated quietly for five minutes, arm at heart level. White-coat readings in the office miss what's really happening. The smartest $40 investment in cardiac self-care.
𝗩𝗢𝟮 𝗠𝗮𝘅
Men over 40: above 40 mL/kg/min. Women over 40: above 35.
Cardiorespiratory fitness is the single strongest predictor of all-cause mortality — stronger than smoking, diabetes, or heart disease as individual risk factors. A landmark study in JAMA found that extreme fitness was associated with the lowest mortality with no upper limit of benefit. You can estimate VO2 max with a timed mile, a rower test, or a wearable. Get faster every year.
𝗡𝘂𝗺𝗯𝗲𝗿 𝗼𝗳 𝗠𝗲𝗱𝗶𝗰𝗮𝘁𝗶𝗼𝗻𝘀
Target: as few as possible.
Every medication you're on should be earning its place. I just wrote about five commonly prescribed drugs that do more harm than good with long-term use. Bring your full medication list to every appointment. Ask: "Do I still need this?" Deprescribing is one of the most powerful and underused tools in medicine.
ꟷꟷꟷ
Thirteen numbers. Most available through cheap bloodwork and simple tests. Get them once or twice a year. Here's what I want you to understand: these numbers don't just tell you where you are. They tell you where you're heading. A fasting insulin of 8 today becomes diabetes in five years. An ApoB of 120 today becomes a heart attack in ten. An hs-CRP of 3 today means your arteries are inflamed right now — regardless of how healthy you feel. The standard annual physical checks a fraction of these. It was designed to find disease that's already there. This panel finds the disease that's coming — years before it arrives.
What gets measured gets improved. Optimize with the foundation I write about every week on this platform:
Zone 2 cardio plus resistance training 3-4 times per week. High-protein whole-food nutrition. Sleep 7-9 hours — non-negotiable. Morning sunlight. Stress management. And the targeted supplements I've covered in detail — creatine, magnesium, CoQ10, D3+K2, glycine, omega-3, psyllium husk.
The breakthroughs coming in the next decade — gene editing for cholesterol, cellular reprogramming, senolytics that clear senescent "zombie" cells driving inflammation and aging, GLP-1 drugs rewriting metabolic medicine — will be most powerful for people who've already built the metabolic foundation to receive them.
The future of medicine is personalized. But it starts with knowing your numbers today. Print this list. Book the bloodwork. Own the data. Prevention isn't passive. It's the most aggressive thing you can do for the decades ahead.
For the kind attention of the public please!
All through the night, I performed a post publication peer review of this IIT Roorke paper that claimed that it identified chemical components in cow urine that could highly efectively kill Chikungunya virus in lab conditions.
https://t.co/dFJ6x2eIqQ
There are serious concerns in the paper that mandate post publication Editorial Review from the Journal and Publication Integrity Office, and need for validation of findings... that could mandate a retraction as per COPE Guidelines. A document with all concerns explained has been emailed to:
🟡Professor (Dr) Thomas F. Hofmann
Editor-in-Chief
ACS Agricultural Science & Technology
🟡Copy to: Publication Integrity Office
ACS Publications, American Chemical Society
🟡Copy to: Professor (Dr) Laura McConnell
Deputy Editor, ACS Agricultural Science & Technology
🟡Copy to:William King, The Managing Editor American Chemical Society
A lay summary of major concerns are provided below:
🔴Possible areas of data fabrication, manipulation, and internal contradictions in the study claiming antiviral activity of cow urine distillate (CUD).
🔴Identical efficacy values reported for different experimental conditions, suggesting possible data duplication or carryover.
🔴Methodological flaws, including testing at cytotoxic concentrations, invalidating antiviral claims.
🔴Manipulation of synergy thresholds, using non-standard cut-offs to falsely claim synergism.
🔴Inconsistent and contradictory GC–MS datasets, with discrepancies in metabolite identification and absent compounds.
🔴Identification of synthetic pharmaceuticals, such as medroxyprogesterone, as natural metabolites, indicating contamination or misreporting.
🔴Implausible detection of prostaglandin A1, which is unstable and unlikely to survive high-temperature distillation.
🔴Lack of direct evidence linking identified metabolites to antiviral effects, with concentrations in CUD unverified.
🔴Cytotoxicity confounding viral inhibition results, with host cell death possibly causing false positives.
🔴Weak in silico and biochemical data, with docking scores and enzyme inhibition results unreliable.
🔴Structural inaccuracies in molecular docking, such as improbable hydrogen bonds.
🔴Statistical and analytical misrepresentations, including inappropriate synergy thresholds and wide variability without proper significance testing.
🔴Undeclared conflicts of interest, as funding sources and author affiliations favor traditional and cow-derived products.
🔴Numerous inconsistencies across figures and tables, including contradictory retention times and unlabelled peaks, undermining data credibility.
Requesting for action from the Journal
@ACSPublications@AmerChemSociety@ACSReactions
➡️Initiate an editorial review under ACS and COPE guidelines.
➡️Obtain raw data: plaque counts, cell viability, GC–MS spectra, and metabolite quantification.Verify compound identifications and concentrations with independent analysis.
➡️Reassess the validity of the claimed antiviral mechanism based on verified data.
➡️Reevaluate synergy analyses using standard criteria.
➡️Consider issuing an Expression of Concern pending investigation.
➡️If unresolved, proceed with retraction to protect scientific integrity and public health.