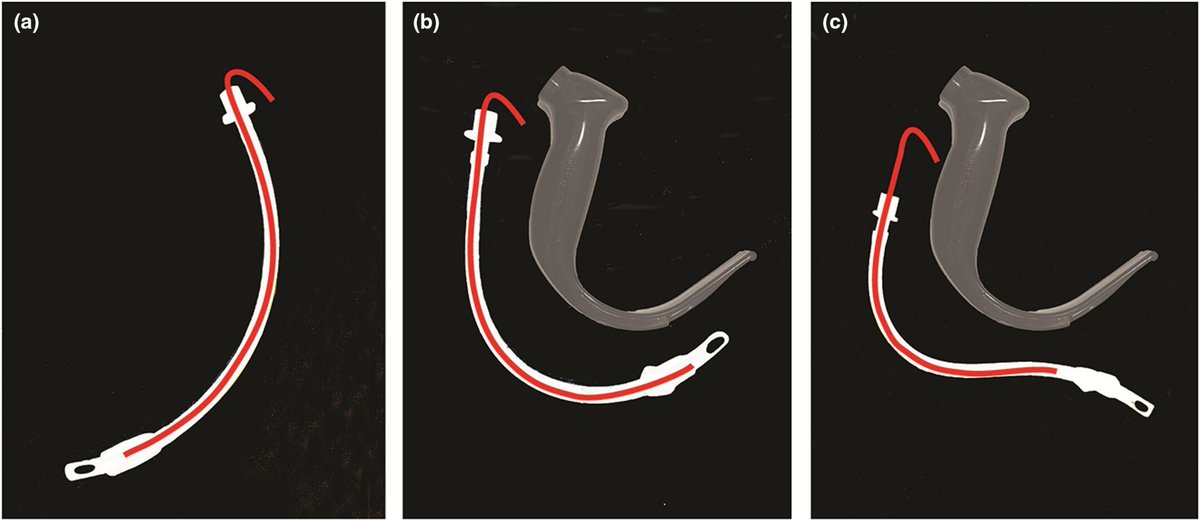
When using a hyperangulated videolaryngoscope have you tried "reverse loading" a tracheal tube on to a preformed stylet?
The stylet & tracheal tube are shaped forcibly in the opposite direction to the normal curvature and to match the shape of the blade.
#anaesthesia #MedTwitter #airway
https://t.co/wOF4wgCXf7
Risk adjusted #DAOH days alive and out of hospital after #colorectal cancer resection was greater in patients without #postoperative complications
https://t.co/2ZtFs3AfAP
Personally I think glottic impersonation is very rare indeed in adults. The fact that the image used is cropped from a wider image that shows both orifices maybe makes that point.
I don’t think it is the ‘explanation’ for oesophageal intubation that some seem to think it is. That’s just getting a poor view and poor delivery of the tube (most commonly during DL) and we’ve ALL done it.
However use of laryngeal grading that does not aid communication or even obfuscates is super common…..
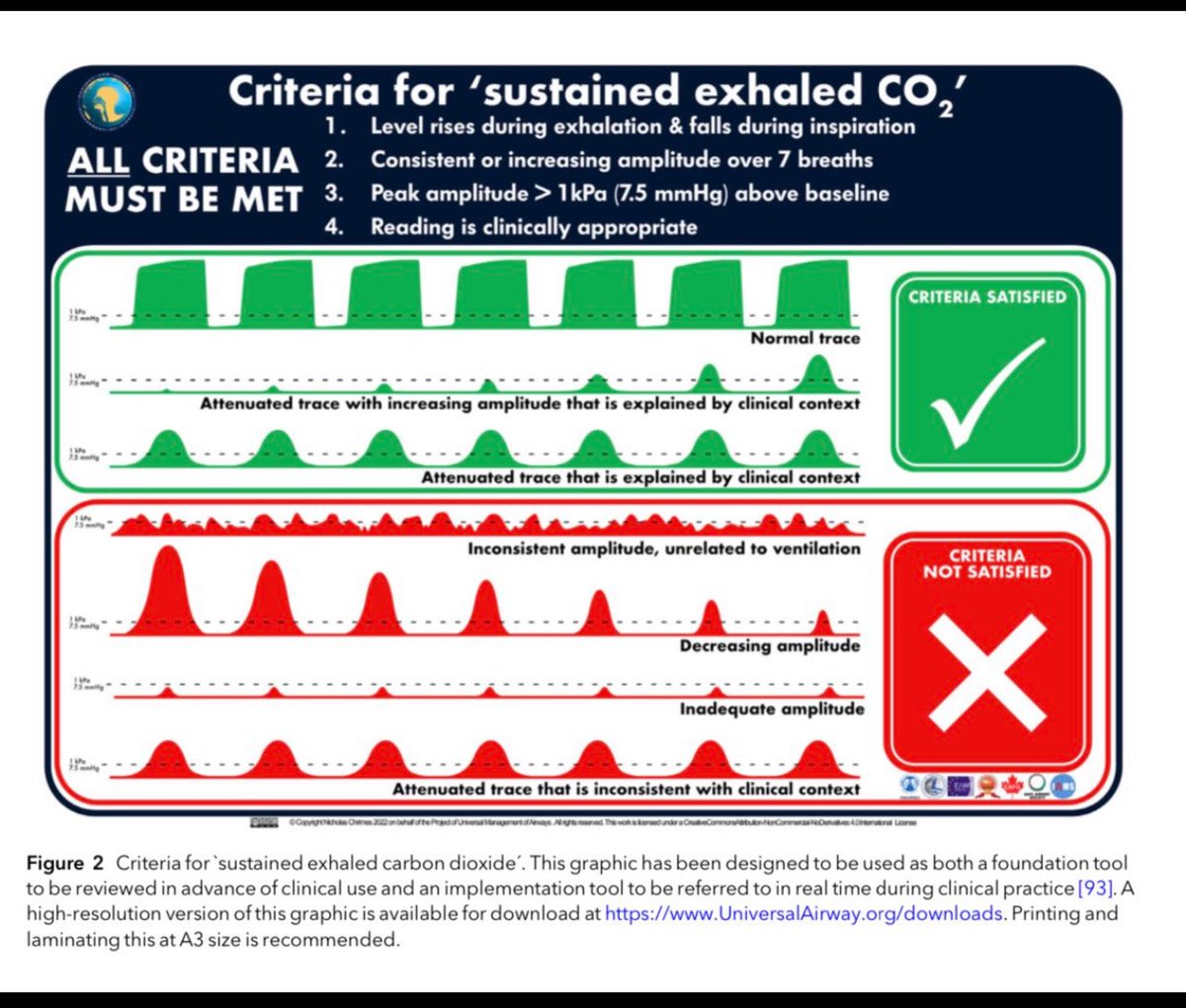
Completely agree with your point about the need to confirm intubation with waveform capnography… but that needs a system and the system is “sustained exhaled CO2” (noting that no trace wrong place has been officially retired)
In my (not so humble) opinion Cormack and Lehane is “practically” useless.
There are 4 problems with it
1 it is poorly described - the worded in the paper don’t match the images
- grade 1 = > 50% of cords (not 100%)
-grade 2 = <50% or just posterior laryngeal structures
2 the change in grade has no correlation with the point at which a change in technique (for Mac Laryngoscopy) is needed
- can see cords: stick tube in
- can’t see cords but can lift epiglottis use bougie (75% success rate)
-can’t lift epiglottis or can’t see it: something clever
3 their paper had no data I. It. It had estimates of frequency of grades and rhey were wildly optimistic and since proven to be miles off actual rates
4 it is very poorly remembered/quoted so even fails as a communication tool
Fortunately I sorted thick all out 26 yrs ago.😌
Feel free to join those using th more logical Easy/Retricted/Difficult classification
https://t.co/WgsekFJvPW
Again the line “ gastric ultrasound may guide clinical decision making”….. but I still think we really don’t know “how”
It’s tricky….
We know the incidence of a non-empty stomach in all elective patients is around 5-6% (much higher in some series)
But the incidence of aspiration is around 1 in 10,000
That’s 600-fold lower
If we start doing RSIs or even intubating all these patients then there is a significant risk we’ll cause more harm.
So I think identifying who has a full stomach is the easy bit. Working out who is actually at high risk or deciding what to do about it is the complex one!
Why not use RSI for all patients on a GLP1 agonist?
First - because (as per my previous tweet) the risk of aspiration is >600-fold lower than the risk of having a full stomach
Second because RSI is not a benign technique
- increases risk of failed intubation 8-fold
- increases risk of anaesthetic overdose (CVS instability etc)
-increases risk of anaesthetic under dose (awareness)
Etc etc etc
If using muscle relaxants and TT when otherwise would be using an SGA
-increases risk of airway complications at insertion and removal from use of TT
-increases risk of anaphylaxis from NMBA
-and awareness (from NMBA)
So I think quite a few reasons to pause before deciding swathes of folk need RSI
Yes but what do we then do for airway management….?
We know the incidence of a non-empty stomach in all elective patients is around 5-6% (much higher in some series)
But the incidence of aspiration is around 1 in 10,000
That’s 600-fold lower
If we start doing RSIs or even intubating all these patients then there is a significant risk we’ll cause more harm.
So I think identifying who has a full stomach is the easy bit. Working out who is actually at high risk or deciding what to do about it is the complex one!
@kariem
@anzics and the @Int_SRRS are exploring the feasibility of holding a combined RRS / safety and quality meeting in Christchurch in 2017
Let us know if you be willing to attend using the QR code below
Another death involving unrecognised oesophageal intubation. Misinterpretation of chest impedence trace as ETCO2 trace.
PUMA guidelines address the need for monitoring displays to be standardised and ETCO2 trace to be distinctive. Free full text in @Anaes_Journal
https://t.co/7tCqUbdCPd
https://t.co/abmtwcGSa8
@andonia911 @AirwayMxAcademy@Anaes_Journal There should be processes in place to deploy airway equipment urgently to anywhere in the hospital but in areas where airway management is regularly performed or the need for it is easily foreseeable (such as PACU), the equipment should be immediately available.
Time to adopt
SUSTAINED EXHALED CO2
This is because ‘no trace wrong place’ is
-insufficient (oesophageal intubation can occur with a trace:an abnormal one)
-misconstrued (eg wrong place always equals no trace, or ‘good trace equals right place’)
-used outside it’s original remit (cardiac arrest)
SECO2
If far better suited to detecting the possibility of oesophageal intubation
- which continues to cause avoidable deaths
https://t.co/m0v20Kaxa0
In Australia & NZ you should only be using rocuronium if there’s a benefit to the patient from its rapid onset.
That doesn’t necessarily require it to be RSI, could just be challenging FMV, short safe apnoea time, etc.
If you just want to reverse w sugammadex, use vecuronium.
• There is a significant difference between the rates of peri-operative hypersensitivity reactions with rocuronium and suxamethonium vs. atracurium.
• Females may be higher risk than males of reacting to neuromuscular blocking drugs.
#anaesthesia#allergy#MedTwitter
https://t.co/YVDmrFZ3PO
@dasairway guidelines out
USE A VIDEOLARYNGOSCOPE
DEFAULT Videolaryngoscopy is now the recommended norm
Some folk will need to make changes.
We recently published a narrative review which discusses the challenges and myths around VL and gives guidance on default VL implementation from those who have done it
https://t.co/WjyLh1AuSV
@BJAJournals@Anaes_Journal@Fionafionakel
1/2