Recommed me Local guide from amsterdam to keukenhof for tulip festival 2027 please. I would love to bring my 80 years old mother for the festive. Trying my luck on X.
CKD staging isn’t just about GFR anymore. Albuminuria changes everything. 🫘
CKD is classified by 3 things:
📌 Cause (C)
📌 GFR (G)
📌 Albuminuria (A)
Here’s why it matters clinically:
Same GFR, very different risk:
A patient with GFR 60 (G2) and normal albumin → 🟢 Screen only
That same patient with GFR 60 + albumin ≥300 mg/g → 🔴 Treat AND refer
The referral thresholds:
🟢 G1–G2 + A1 → Screen (monitor, no CKD if no other markers)
🟡 G1–G3a + A2 / G3a + A1 → Treat (1–2x/year follow-up)
🟠 G3b+ or A3 → Treat and refer (3x/year)
🔴 G4–G5 (any albuminuria) → Treat and refer (4+ visits/year)
Bottom line:
Don’t just check the creatinine.
Check the urine albumin.
A patient with preserved GFR and heavy proteinuria is already high risk.
The number in each cell = recommended monitoring visits per year. Act accordingly.
#CKD #Nephrology #KidneyDisease #Albuminuria #GFR #InternalMedicine #MedEd
🇺🇸🇻🇦 The day after Trump called him "WEAK on Crime" and "terrible for Foreign Policy," Pope Leo XIV walked into the Grand Mosque in Algiers.
The first American pope, attacked by an American president, responded by visiting a Muslim house of worship in Africa.
The message wasn't subtle and it probably wasn't meant to be.
Nicole Kidman vs. Lauren Sanchez is the perfect metaphor for 𝕏
You do your best to genuinely get some attention and then the big account enters the room 🤣
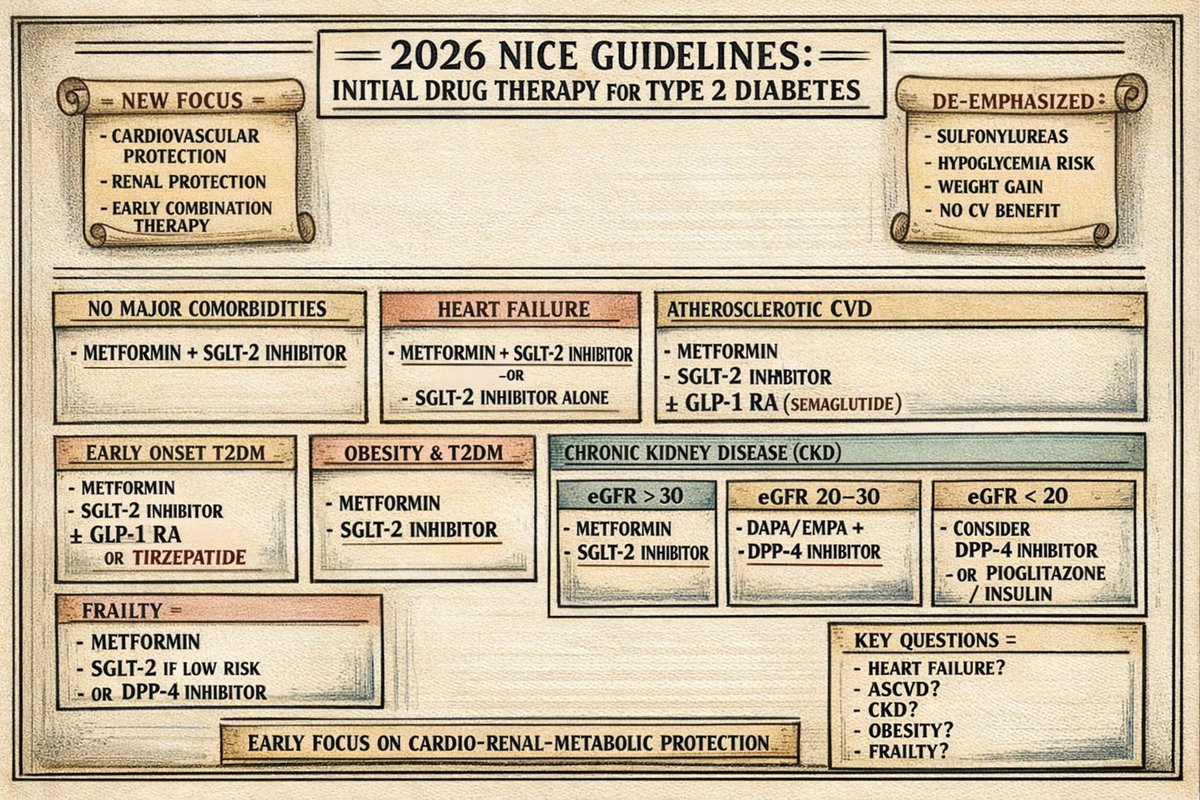
🧵 New 2026 NICE Update on Initial Drug Therapy in Type 2 Diabetes Detailed Thread
1️⃣ Big Shift in Philosophy
This is no longer just about lowering HbA1c.
The new guidance prioritises:
• Cardiovascular protection
• Renal protection
• Individualised treatment
• Early combination therapy
Glucose control is important but outcomes matter more.
2️⃣ First-Line Therapy (No Major Comorbidities)
For most adults:
✅ Modified-release metformin
PLUS
✅ An SGLT-2 inhibitor
If metformin cannot be used → start SGLT-2 inhibitor alone.
➡️ This is a major shift from traditional “metformin first, add later.”
3️⃣ Why SGLT-2 So Early?
Because evidence now strongly supports:
• Reduction in heart failure hospitalization
• Slowing CKD progression
• Cardiovascular mortality benefit
• Weight reduction
• Low hypoglycaemia risk
This class is now foundational therapy.
4️⃣ If the Patient Has Heart Failure
Start immediately:
✅ Metformin
✅ SGLT-2 inhibitor
If metformin contraindicated → SGLT-2 alone.
HF benefit drives this decision independent of HbA1c.
5️⃣ If Atherosclerotic CVD Is Present
Initial therapy can include:
✅ Metformin
✅ SGLT-2 inhibitor
✅ Subcutaneous semaglutide (GLP-1 RA)
If Yes 👉🏻 GLP-1 RA can now be started upfront in ASCVD.
This reflects strong CV outcome trial data.
6️⃣ Early-Onset Type 2 Diabetes
(Younger patients, aggressive phenotype)
Start:
✅ Metformin
✅ SGLT-2 inhibitor
Consider adding:
• GLP-1 receptor agonist
• Tirzepatide
This group often needs earlier intensification.
7️⃣ Obesity + Type 2 Diabetes
Initial therapy:
✅ Metformin
✅ SGLT-2 inhibitor
Weight-neutral or weight-reducing strategies are preferred.
Avoid agents that promote weight gain unless necessary.
8️⃣ Chronic Kidney Disease (CKD)
Treatment depends on eGFR:
🔹 eGFR >30 → Metformin + SGLT-2
🔹 eGFR 20–30 → Dapagliflozin or Empagliflozin + DPP-4 inhibitor
🔹 eGFR <20 → Consider DPP-4 inhibitor
If DPP-4 not suitable → consider pioglitazone or insulin.
Renal protection is central in this update.
9️⃣ Frailty
Be cautious.
Offer:
✅ Metformin
Consider SGLT-2 only if risk of:
• Hypotension
• Dehydration
• Falls
If risk is high → DPP-4 inhibitor may be safer.
Individualisation is critical here.
🔟 What’s Clearly De-emphasised?
Sulfonylureas are no longer early go-to drugs.
Reasons:
• Hypoglycaemia risk
• Weight gain
• No cardiovascular benefit
They are now secondary options.
1️⃣1️⃣ Key Takeaway
The 2026 update moves us from:
“Glucose-centric diabetes care”
➡️ to
“Cardio-renal-metabolic protection from day one.”
Early combination therapy is now the norm, not the exception.
1️⃣2️⃣ Practical Clinical Message
When starting treatment in Type 2 Diabetes, now ask:
• Does this patient have HF?
• ASCVD?
• CKD?
• Obesity?
• Frailty?
The comorbidity determines the drug choice not just HbA1c.
https://t.co/mlP4dTeHVp
#MedTwitter #MedX
Checotah, Oklahoma’s own Carrie Underwood demonstrated grace under pressure today and her incredible talent. Thank you for honoring our beautiful nation.
Retinoids are the ONLY 'miracle' skincare ingredient.
They treat acne, pigmentation, scarring, fine lines/ wrinkles, and even have anti-cancer effect. But most people use them wrong, end up with irritated skin, and stop. Here's the RIGHT way to use them in your routine... 👇 1/
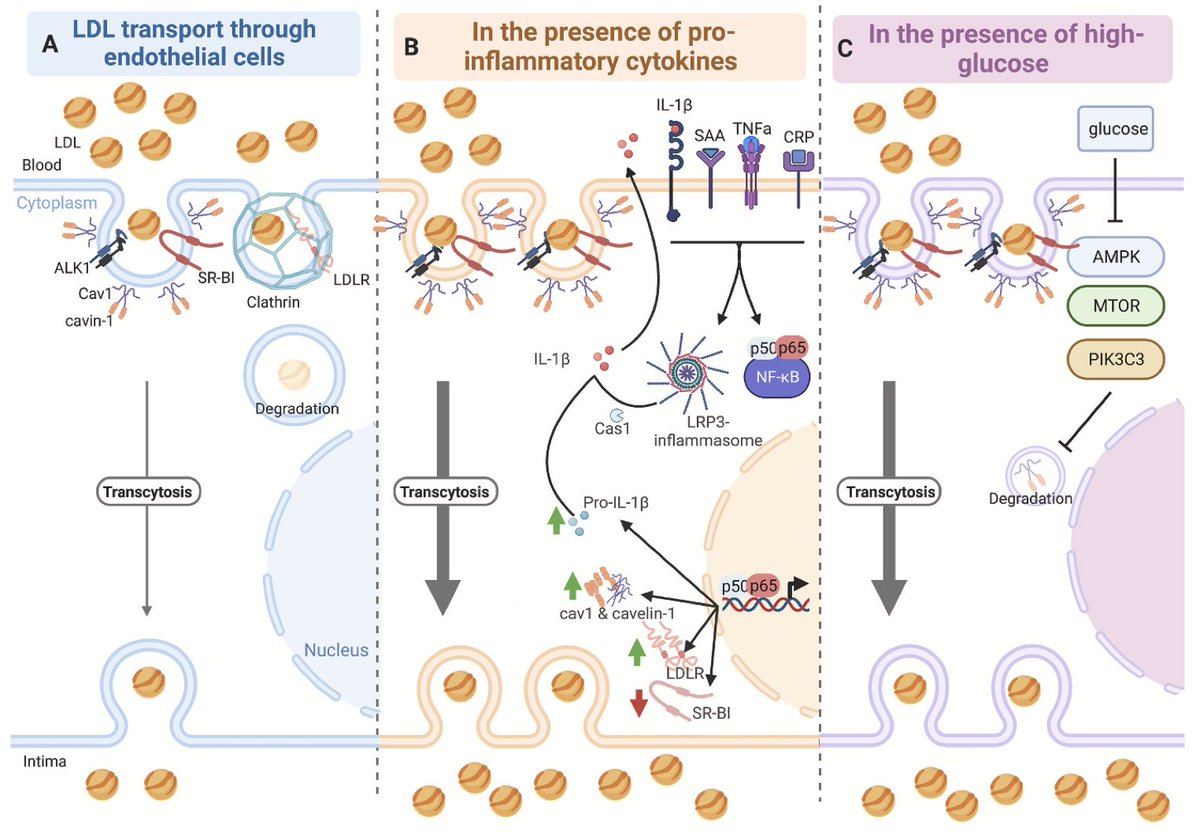
New Study Demonstrates How Inflammation🔥pulls LDL into the Artery Wall - 🧵 for the lay-reader (upon request)
LDL particles play a role in the pathway of atherosclerosis. To do this, they must enter the artery wall by passing through the endothelium, a thin membrane that lines the walls of blood vessels
But how? Do LDL particles just passively flow through the endothelium like grains of rice thrown at a chicken-wire fence?
Well, the diameter of an LDL is on the order of 20-30 nm, whereas the gaps between endothelial cells is ~3-6nm... so, instead, LDL must be transported, actively, into the artery wall. Inflammation plays a role here.
This new study shows that inflammatory transcriptional regulators and cytokines (signaling molecules) increase the expression of proteins involved in the formation of pockets of membrane,"caveole," that 'suck up' LDL particles.
Specifically, the inflammatory cytokines include TNFalpha and IL-1Beta, which activate NLRP3 inflammasome, which causes increased expression of proteins that compose caveole and contribute to LDL transcytosis (active transport through the endothelium)
Earlier studies also showed the elevated glucose promotes this transcytosis process
In summary, inflammation and elevated glucose are 2 factors that cause LDL to be taken into artery walls and promote atherosclerosis.
Questions that remain (for me) are:
- what is the relative impact of high LDL alone is the ABSENCE of chronic pathological inflammation and/or elevated glucose?
- what therapeutic approaches could prevent cardiovascular disease by targeting these pathways (by extension, what cardioprotective role might ketosis play via beta hydroxybutyrate, which inhibits NLRP3)?
- what are other pathways involved in transcytosis (including the undiscovered and understudied), and might there be a more bidirectional and dynamic process, in the context of a healthy metabolism, than we previously thought?
https://t.co/hxUxLfM8gi
https://t.co/LMB4qG4h4b
@DoctorTro Would support low-carb diet as a cardiologist who treat a lot of patients with metabolic syndrome. Unfortunately, almost all refuse to comply.
I started smoking cigarettes at age 12 and became a daily drinker at age 17
At age 58 I'm 20 years sober, an Ultramarathon runner and Ironman Triathlete
You can reinvent yourself at anytime