In patients with #AFib undergoing ablation, a PVI-only approach shows noninferior rhythm control efficacy and comparable procedural safety in patients with #HFrEF compared with those without HFrEF. https://t.co/Dc2am0hMho #JACCCEP
2️⃣0️⃣ years after PVI during catheter ablation, stable sinus rhythm was maintained in a quarter of pts w/ symptomatic drug-refractory paroxysmal #AFib, including those taking antiarrhythmic drugs & those who had multiple ablation procedures. 🔗 https://t.co/YC3O9yNYbZ #JACCCEP
Pulsed-Field vs Thermal Ablation of Atrial Fibrillation in Patients From the Marshall Islands: A Study of Generalized Coronary Spasm | JACC: Clinical Electrophysiology https://t.co/SZMqG4GIxW
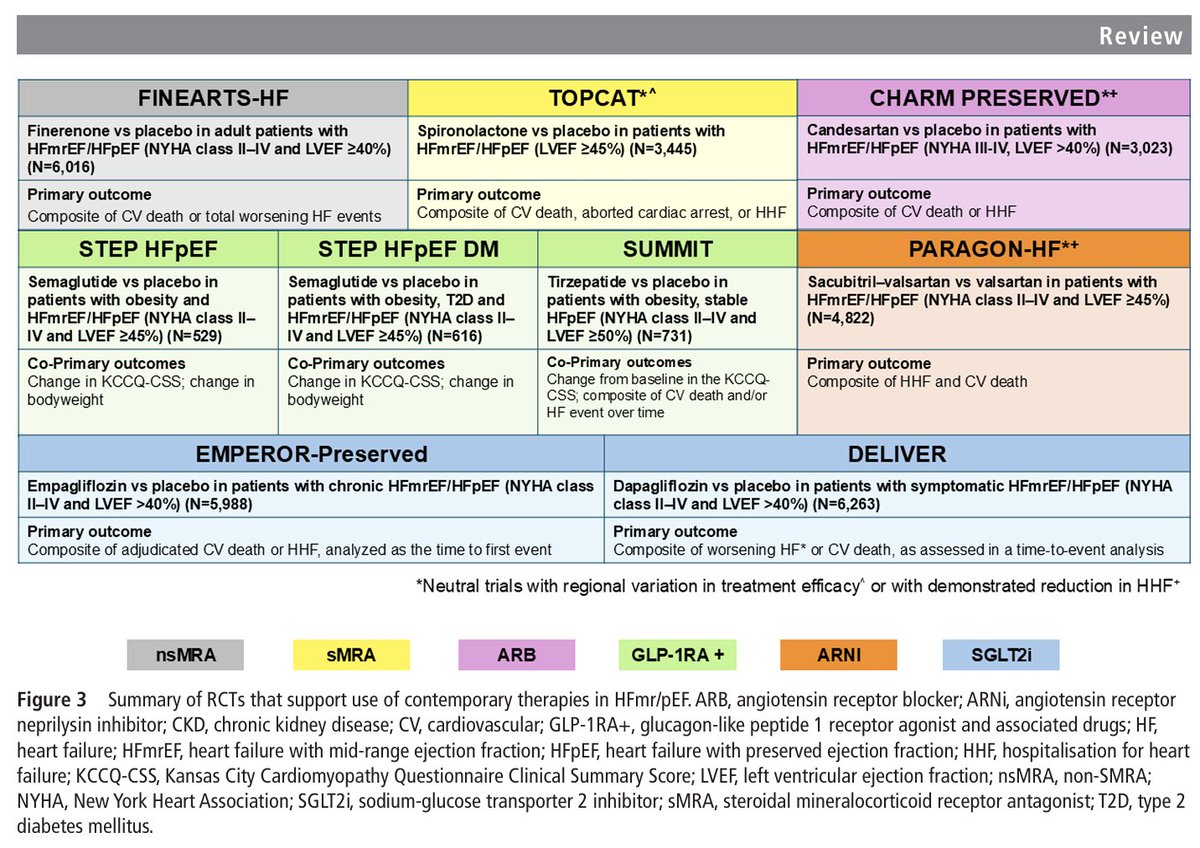
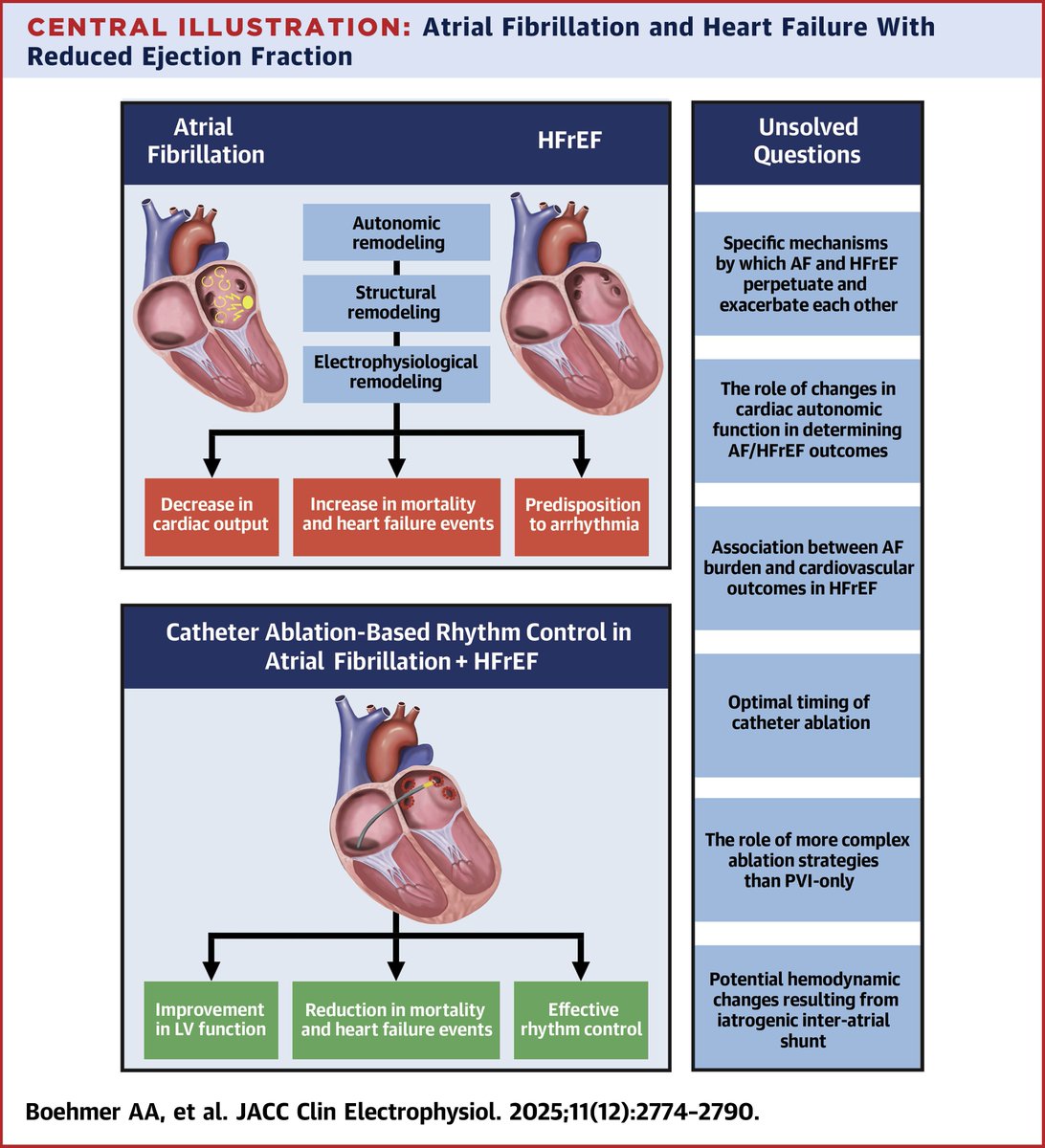
#AFib+HFrEF: State-of-the-Art Review📚
Recent data show SR restoration ⬆️ LV function & ⬇️death/HF hosp vs medical therapy.
🤔Should ablation be first-line or are we over-selecting responders?
🖇️https://t.co/6eq9GCyWfW
@JACCJournals@LuigiDiBiaseMD@nmarrouche@DhirajGuptaBHRS
Congreso #Ritmo26
11-13 Marzo, Córdoba, España 🇪🇸
Los socios LAHRS con cuota al día cuentan con becas en la inscripción PRESENCIAL a dicho evento
Este beneficio tiene validez hasta el día 23 de Febrero
Solicite su beca a [email protected]
https://t.co/jmaQ05s5sl
Congrats to @Peteweissmd and collaborators on this first-ever Early Feasibility Study to evaluate Ultra-Low Cryoablation for Scar-Related VT Ablation. We greatly appreciate @US_FDA initiatives to prioritize early technology evaluations in the US. #FirstinPHX#ablateVT
https://t.co/qdAmeGA1Lv
Congreso #HRS2026
Beneficio Socios LAHRS
Bonificación del 75% en la inscripción PRESENCIAL al congreso HRS en la ciudad de Chicago 🇺🇸
Solicite su código de beca a [email protected]
https://t.co/70d94Xa5d1
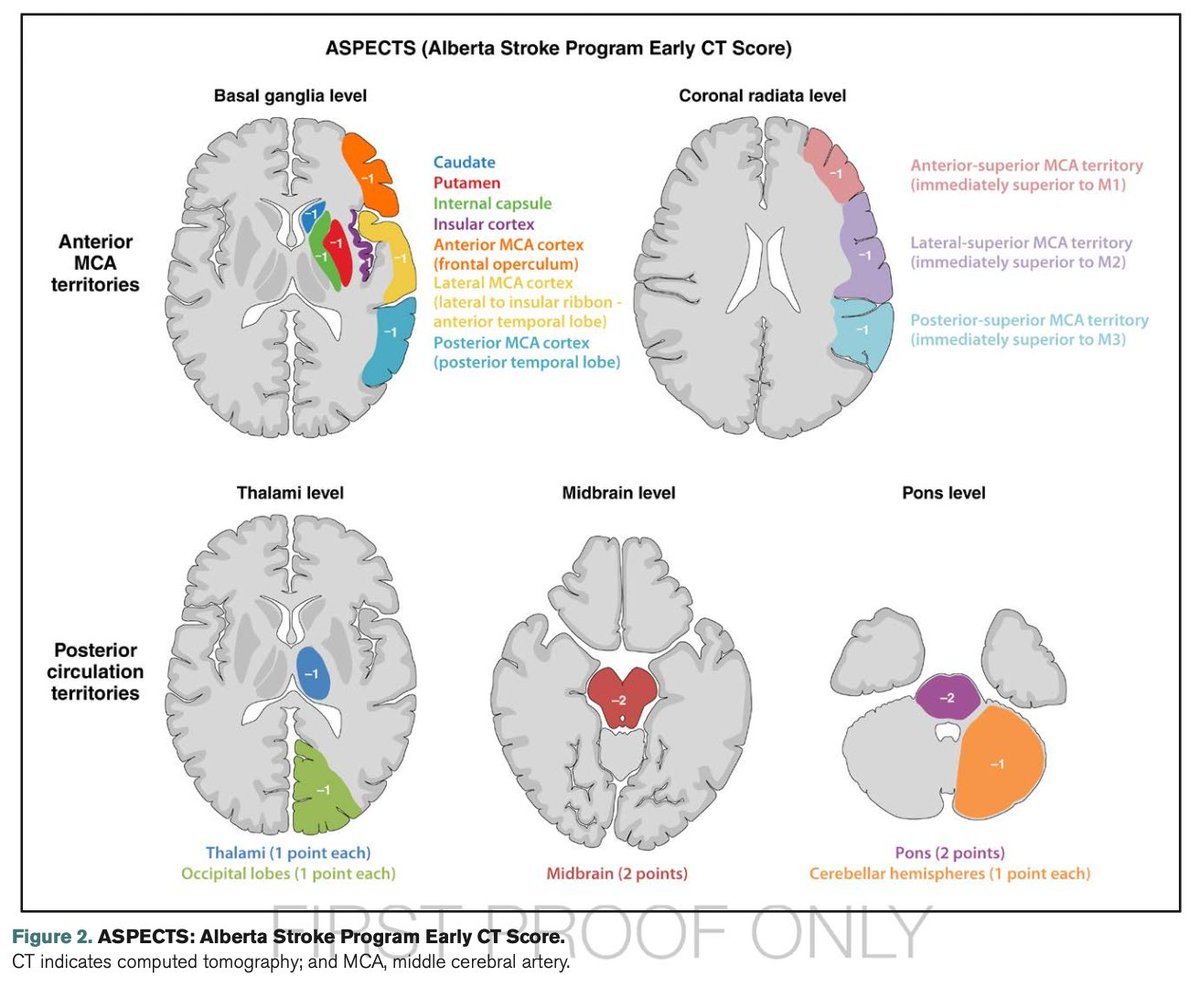
Recién salidas del horno: Guía AHA, 2026, de Evento Vascular Cerebral (EVC) Isquémico. Cambios o puntos relevantes:
🔴 Tenecteplase vs. Alteplase (Cambio Mayor) Se recomienda el uso de Tenecteplase (0.25 mg/kg, bolo único, máx. 25 mg) como una alternativa de primera línea, no inferior a la Alteplase, para pacientes elegibles en la ventana de 4.5 horas. Nota: La dosis de 0.4 mg/kg de Tenecteplase no se recomienda por falta de beneficio adicional y mayor riesgo de seguridad.
🔴 Ictus Leve No Incapacitante: En pacientes con déficits leves que no son incapacitantes (ej. síndrome sensitivo aislado, NIHSS bajo sin impacto funcional) dentro de las 4.5 horas, no se recomienda la trombolisis IV. Se prefiere la doble antiagregación plaquetaria (DAPT).
🔴 Trombectomía (EVT) en "Large Core": Se amplía la indicación de trombectomía mecánica para incluir pacientes con infartos de núcleo isquémico grande establecidos (ASPECTS 3-5), (antes eran excluidos).
🔴 Se desaconseja la reducción intensiva de la PAS (<140 mmHg) tras una reperfusión exitosa. Objetivo: TA <180/105 mmHg en las primeras 24 horas.
🔴 Oclusión de Arteria Basilar: realizar trombectomía en pacientes con oclusión de la arteria basilar a las <24 horas si NIHSS ≥10.
🔴 Control Glucémico: mantener entre 140-180 mg/dL.
🔴 Ventanas Extendidas de Trombolisis: Se recomienda el uso de trombolisis IV en ventana extendida (4.5 a 9 horas o ictus del despertar) en pacientes seleccionados mediante imagen avanzada que demuestre mismatch (DWI-FLAIR o Perfusión).
🔴 Nuevas Guías Pediátricas: Por primera vez se incluyen recomendaciones específicas para pediatría
Vamos a revisarlas a fondo para actualizar las apps.
Among 409 patients undergoing #transcatheter aortic valve replacement, intraprocedural block occurred in the atrioventricular node or His bundle, with site-specific predictors for intraprocedural and delayed heart block.
https://t.co/KOQePnxJB0
The anatomy of atrial conduction: a review of anatomical landmarks integrated with computed tomographic virtual dissection to provide a road map for right atrial pacing #OpenAccess@JustinTretterMD
https://t.co/v1axQpuSJ7