“PaO₂/FiO₂ and SpO₂/FiO₂ ratios revisited: Useful, misleading, or both?” in the Journal of Intensive Medicine. A review exploring the strengths, pitfalls, and future of oxygenation metrics in ARDS and respiratory failure.
https://t.co/etYyBGzhys
🫀⚠️ Post-resuscitation vasoplegic shock: are we targeting the right physiology?
After ROSC, we often focus on blood pressure.
But the problem is much more complex.
🧠 What is really happening?
Post-resuscitation shock is not a single entity:
👉 Myocardial dysfunction
👉 Vasoplegia
👉 Relative hypovolemia
➡️ And their contribution changes over time in the same patient
📌 Current standard
✔️ MAP target: ≥ 60-65 mmHg
❌ No strong evidence supporting higher targets (>70 mmHg)
👉 Higher MAP may improve myocardial injury and cerebral oxygenation
👉 But no clear outcome benefit
💉 Vasopressor reality
• Norepinephrine = first-line
• Epinephrine → ↑ mortality, arrhythmias (observational data)
• Dopamine → ↑ arrhythmias
➡️ Catecholamines are necessary… but not harmless
🔥 The hidden problem: vasoplegia
Driven by:
• Ischemia-reperfusion injury
• Cytokine surge
• Nitric oxide overproduction
• Vasopressin deficiency
➡️ Leading to loss of vascular tone and responsiveness
⚖️ Are we overusing catecholamines?
High adrenergic load may cause:
• Myocardial injury
• Arrhythmias
• Immune dysregulation
• Receptor desensitization
➡️ This is why catecholamine-sparing strategies are emerging
🧩 What about vasopressin?
✔️ Physiological rationale exists
✔️ May reduce catecholamine exposure
❌ No strong evidence for routine use post-ROSC
❌ Possible ischemic risks
📊 Key concept: hemodynamic phenotype
Not all patients are the same:
• Early phase → low CO + high SVR
• Later phase → high CO + low SVR
➡️ Same MAP ≠ same perfusion
👉 This is where multimodal monitoring becomes essential
🚨 Critical insight
Optimizing MAP alone:
❌ Does NOT guarantee microcirculatory perfusion
❌ Does NOT ensure organ protection
🔥 Take-home message
Post-resuscitation shock is:
👉 Dynamic
👉 Heterogeneous
👉 Frequently oversimplified
And:
➡️ Vasopressor therapy should be individualized, not protocolized
📚 Jendoubi A. et al. (2026)
Critical Care
https://t.co/AdBRWWeHHP
Primer consenso de expertos sobre conocimientos formativos básicos y avanzados en EEG durante la anestesia @JG_Anestesia@mjcolomina@Lorena_Varela_R@MarinaVarelaDu1@dramarusa
Disponible en file:///Users/alfredo/Downloads/consensus_document_on_electroencephalography.398.pdf
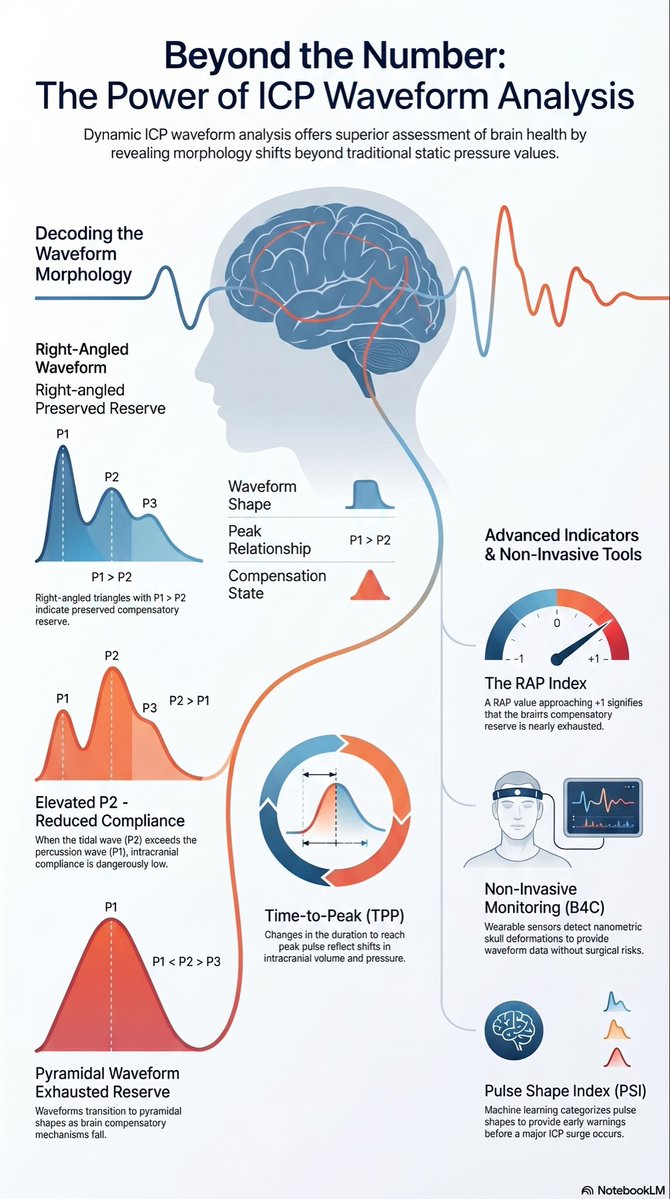
🧠 A major paradigm shift is underway in neurocritical care, moving beyond static intracranial pressure (ICP) thresholds to dynamic ICP waveform analysis for patients with acute brain injuries!
📦 The classic Monro-Kellie doctrine of intracranial dynamics is evolving to account for these complex intracranial pressure-volume relationships 🌊. When these vital buffering mechanisms fail, patients face a dangerously reduced tolerance to volume changes known as "intracranial compartment syndrome."
📊 A standard ICP waveform features three key peaks: P1 (percussion), P2 (tidal), and P3 (dicrotic). 📉 As intracranial compliance worsens, the P2 peak grows larger than P1 (resulting in a P2/P1 ratio > 1), and the overall wave morphology shifts from a triangular to a pyramidal shape. (if one compares these with an arterial line P2 coincides with aortic valve closure. ICP waveforms therefore are a reflection of the brain’s cerebrovascular tree “shaking” the intracranial CSF compartment.
🧮 Advanced analytical metrics, such as the amplitude-pressure index (RAP), can successfully quantify this dynamic loss of brain buffering capacity.
🚀 Excitingly, non-invasive innovations like the Brain4Care (B4C) system use wearable scalp sensors to detect nanometric skull expansions, providing reliable P2/P1 ratios without the need for invasive surgery! (TCD is also another non-invasive way to show this pressure-volume relationship and changes in waveforms.)
🎯 Automating and monitoring these dynamic waveform changes allows clinicians to spot patient deterioration early and deliver proactive, individualized treatments.
🔗 Read the full review by Sérgio Brasil and Fabio Silvio Taccone here: https://t.co/qK1uH5Hkf9
@mayoclinicnccfl #NCC #MayoNCC
Comments: “ICP, it’s more than a number.”
https://t.co/LZG2G0WYWO
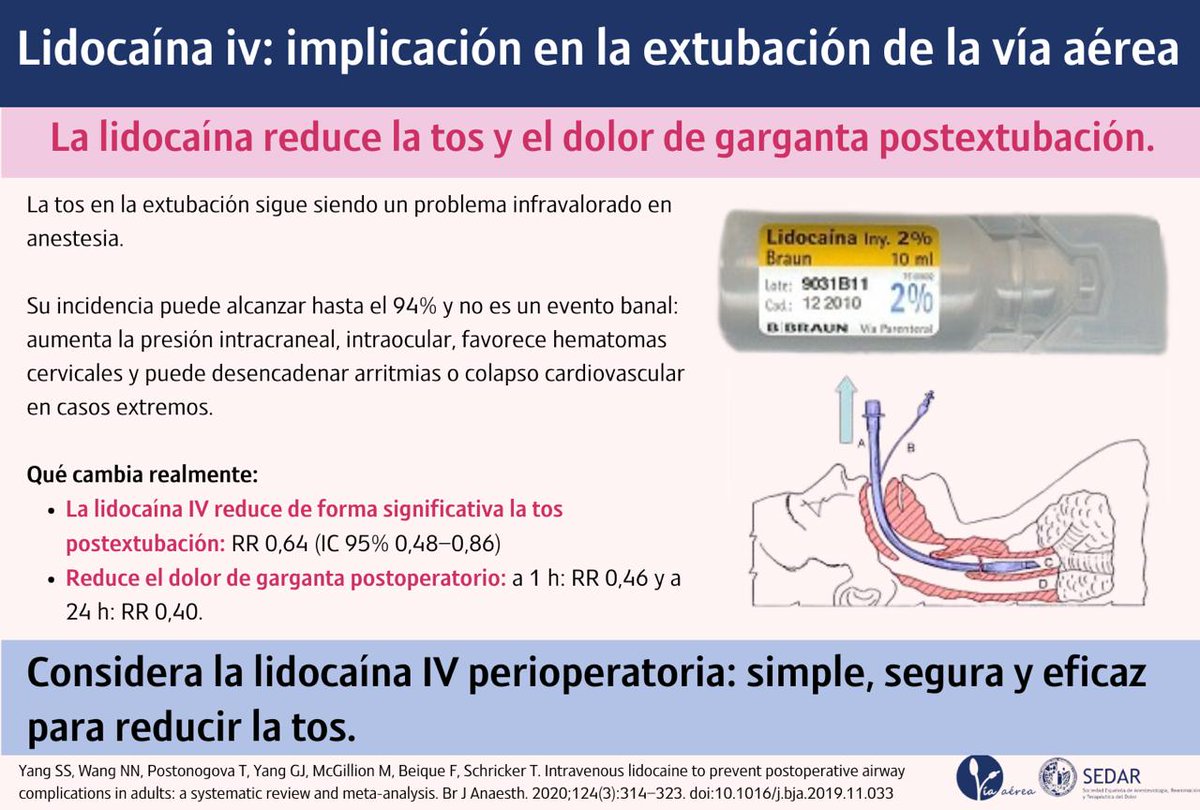
#VíaAéreaSEDAR 💉🫁
¿Hay algo que podamos hacer para evitar complicaciones en la extubación?
👉 Esta revisión indica que la lidocaína IV reduce significativamente la tos (RR 0,64) y el dolor de garganta postoperatorio.
💡 Simple, segura y eficaz.
📖 https://t.co/SN17ntr7Ws
💉The 2026 Anaphylaxis Guidelines highlight something uncomfortable for all of us in acute care:
we do not fail because we lack knowledge, but because we fail to act on what we already know.
Across 12 international guidelines, there is almost perfect agreement on one point:
intramuscular epinephrine is the first and most important intervention⚠️. Yet in real practice, it remains significantly underused, often replaced or delayed by antihistamines or corticosteroids, therapies with no evidence for acute life saving benefit
This gap between evidence and behavior is the central clinical problem.
From a bedside perspective, three insights are particularly relevant:
First, diagnosis remains the main bottleneck, not treatment.
The guidelines clearly show that variability in diagnostic criteria, especially in patients without skin manifestations or in infants, leads to hesitation. Clinically, this reinforces a key principle:
-> anaphylaxis is a clinical diagnosis driven by physiology, not by complete textbook criteria. Waiting for skin signs or full multisystem involvement delays epinephrine and worsens outcomes.
Second, the document reframes management from a pharmacologic problem to a systems and education problem.
Underrecognition by clinicians, lack of training in schools and community settings, and poor patient education all contribute to undertreatment. In reality, the success of anaphylaxis management depends less on ICU level interventions and more on early recognition and immediate action in prehospital environments.
Third, there is a clear shift toward proactive risk management rather than reactive treatment.
Modern guidelines emphasize emergency action plans, patient carried epinephrine, and structured education programs. This aligns with a broader trend in critical care: outcomes improve when interventions occur before physiological collapse, not after.
An important nuance for critical care physicians is the role of adjunctive therapies.
Antihistamines and corticosteroids are consistently positioned as SECONDARY, non life saving treatments. Their continued overuse reflects a cognitive bias toward treating visible symptoms rather than addressing the underlying hemodynamic and airway threat. Clinically, this is equivalent to treating hypotension in septic shock with paracetamol.
🤓Bottom line:
Anaphylaxis is one of the clearest examples in medicine where the evidence is simple, but implementation fails.
The priority is not new drugs or devices, but closing the gap between recognition and immediate epinephrine administration.
📃Reference
Wallace DV, Immunol Allergy Clin N Am ▪ (2026) https://t.co/VoarNwD7v7
Update to my PENG block Video out now on my YouTube channel!
Great for Hip Arthroplasty, Arthroscopy & Fracture!
Link Here👇🏽👇🏽👇🏽
https://t.co/QhrJ6TIn9m
#RegionalAnaesthesia#RegionalAnesthesia
#DocenciaSEDAR | Nuevas herramientas de simulación farmacocinética aplicadas a la TCI.
Puedes ampliarlo en este magnífico blog 👇
https://t.co/DaQz3CXADb
#DocenciaSEDAR
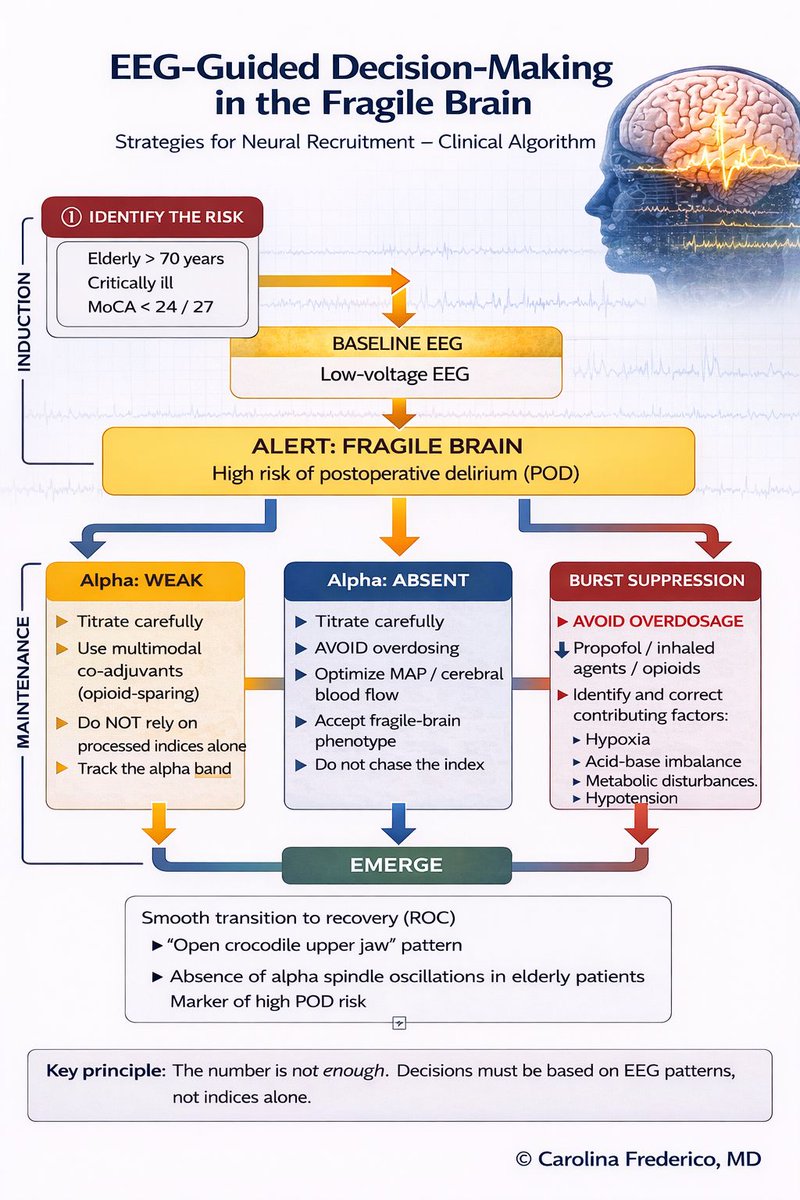
👉 EEG-guided anesthesia in the elderly: Where is the real challenge?
⚠️ El cerebro frágil no se comporta igual.
Una correcta interpretación del EEG marca la diferencia en el paciente mayor.
Aquí una infografía para ayudarte.