A striking #ImagesInRadiology case reveals the tunnel sign in pulmonary paragonimiasis 🫁
CT reconstructions exposed interconnected tunnel-like cavities, steering diagnosis away from TB & toward Paragonimus westermani, confirmed by history & serology.
https://t.co/GZfeJYWZhO
Hypercalcemia in patients with Hodgkin's lymphoma typically presents with a suppressed parathyroid hormone (PTH) level.
In these cases, the hypercalcemia is usually driven by the extralymphatic/unregulated overproduction of 1,25-dihydroxyvitamin D (calcitriol) by the lymphoma cells or associated macrophages, rather than by the parathyroid glands.
●Why Does This Happen?
*Unregulated 1-α-hydroxylase Activity:
The cells in Hodgkin's lymphoma (including macrophages and the tumor cells themselves) overexpress the enzyme 1-α-hydroxylase.
This causes unregulated conversion of inactive Vitamin D into its active form, 1,25
-(OH)_2D calcitriol.
*The Mechanism:
Excess calcitriol dramatically increases the absorption of calcium from the gut.
*Suppressed PTH:
The high calcium load in the bloodstream acts on the parathyroid glands via negative feedback, shutting down or "suppressing" natural PTH production
https://t.co/0N7wUCCuiZ
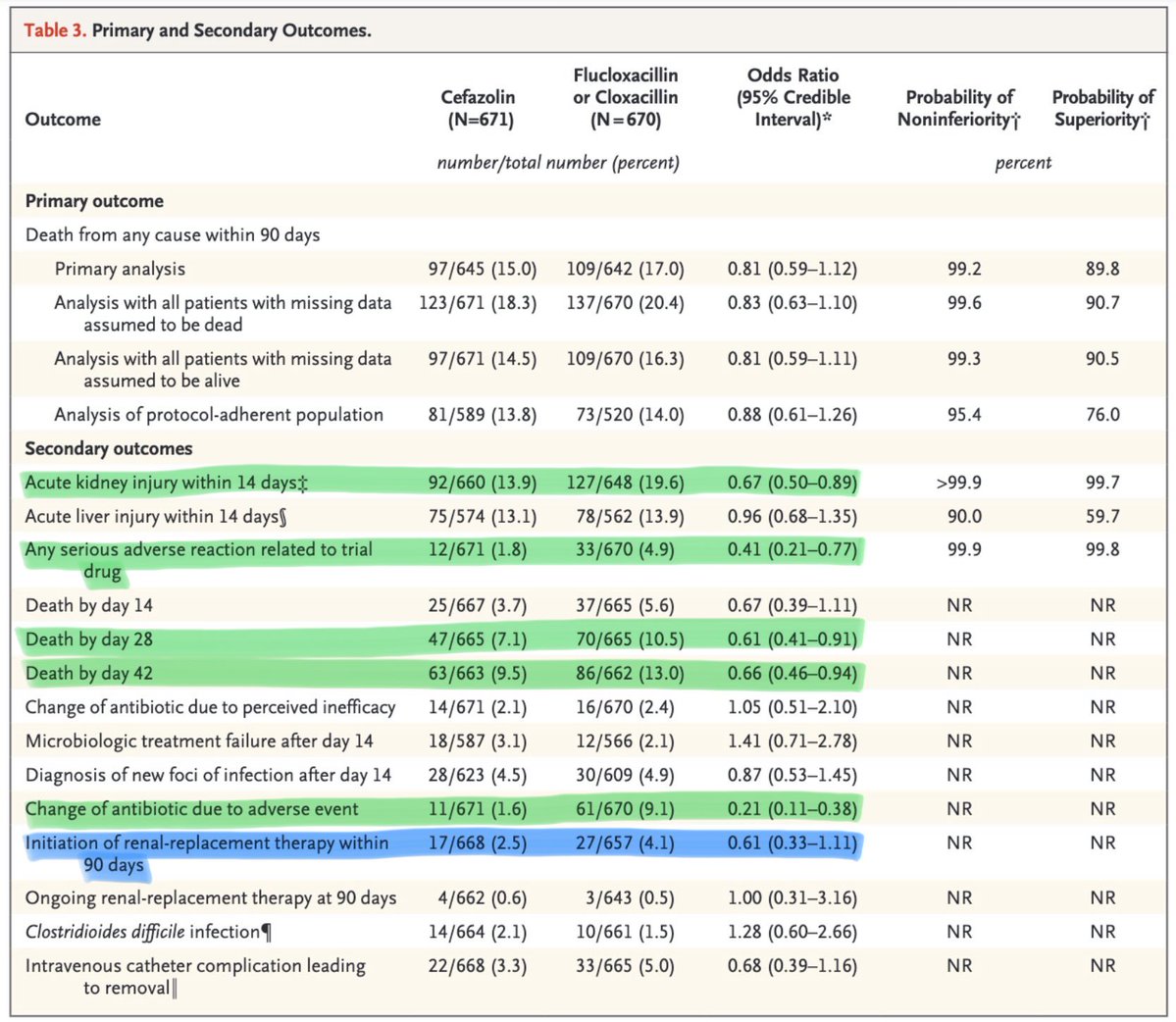
For MSSA bacteremia, the SNAP trial found cefazolin was as effective as antistaphylococcal penicillins but caused fewer serious adverse events, largely due to less AKI.
Same bug. Same outcomes. Less kidney injury.
Cefazolin ftw
https://t.co/cIxGaQOD5b
An algorithmic approach to the diagnosis of organizing pneumonia (OP).
The algorithm is based on the integration of clinical context, chest imaging patterns (specifically HRCT), and tissue diagnosis where necessary.
https://t.co/XQ7B4cSAtE
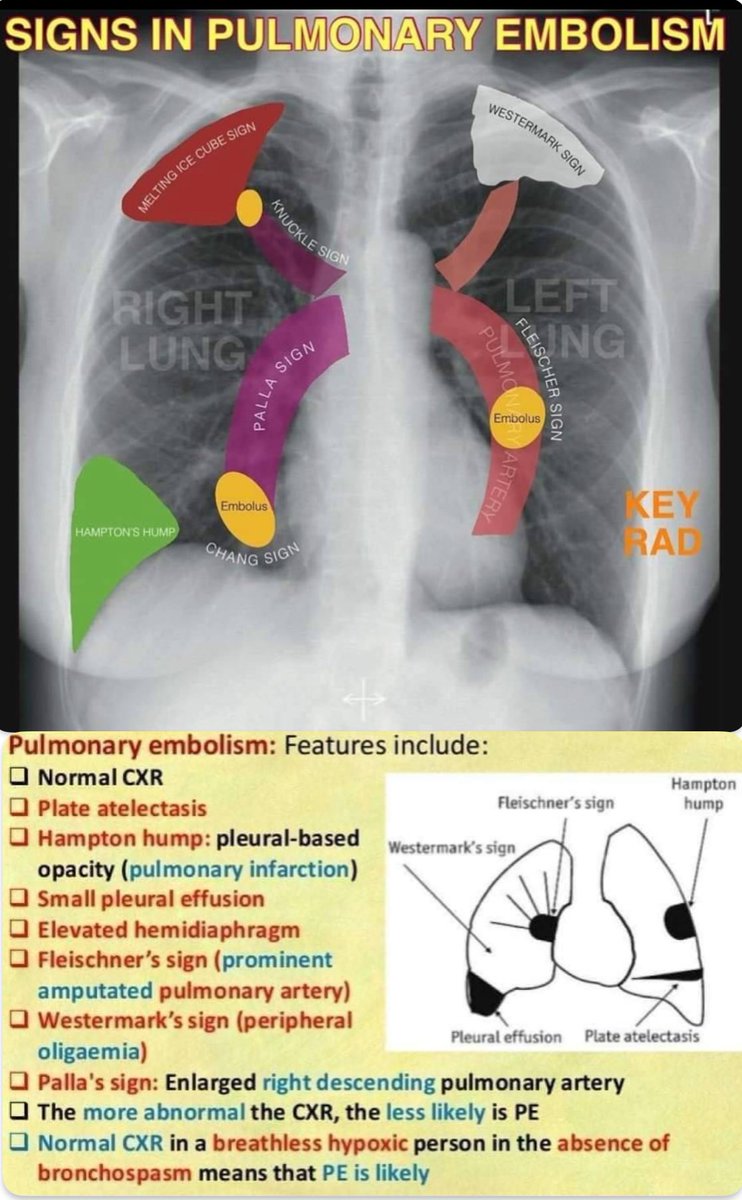
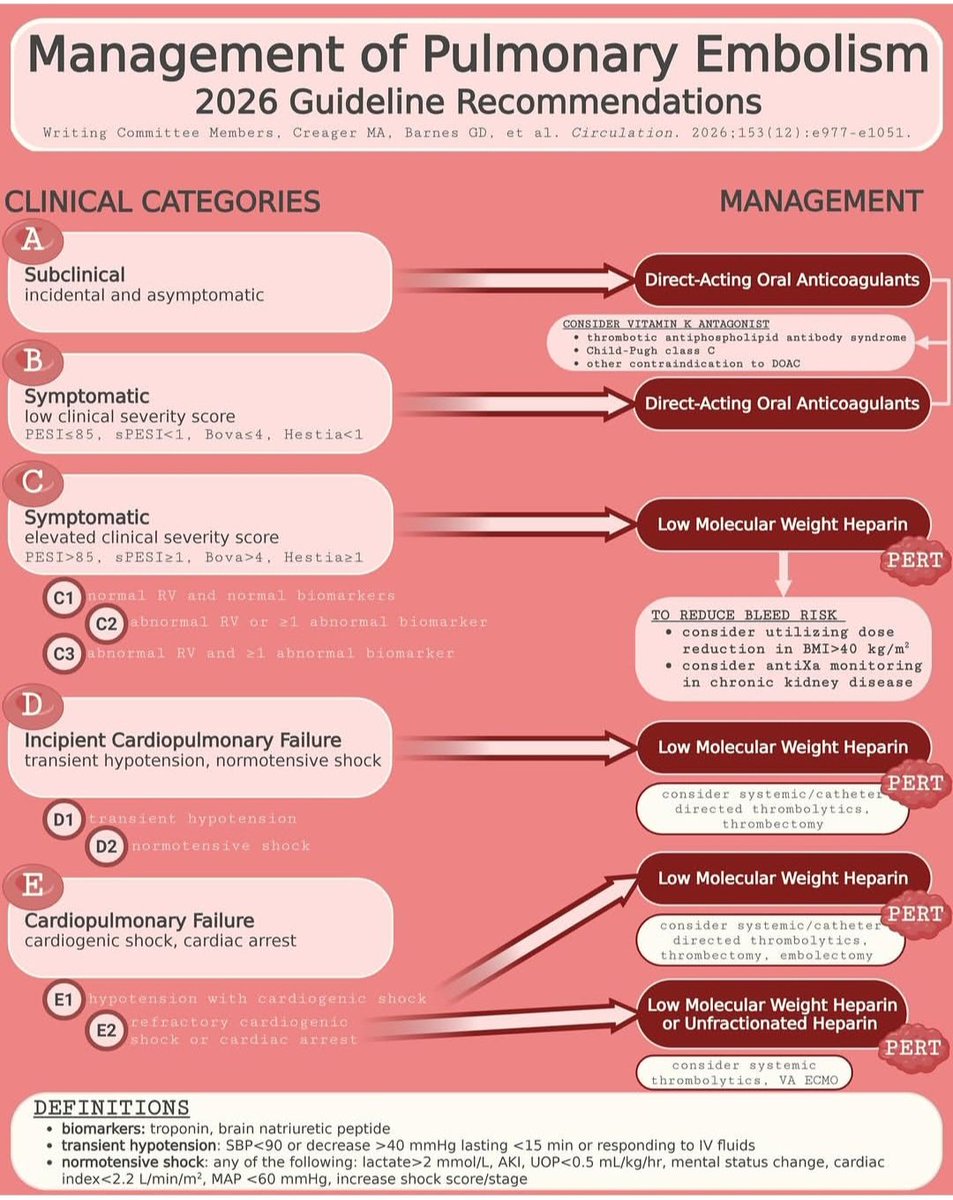
The 2026 AHA/ACC Guideline for the management of acute pulmonary embolism (PE).
This guideline replaces traditional "massive" and "submassive" labels with five clinical categories (A–E) to more precisely guide therapeutic decisions based on clinical severity, biomarkers, and hemodynamic stability.
https://t.co/fDjaz0bvZQ
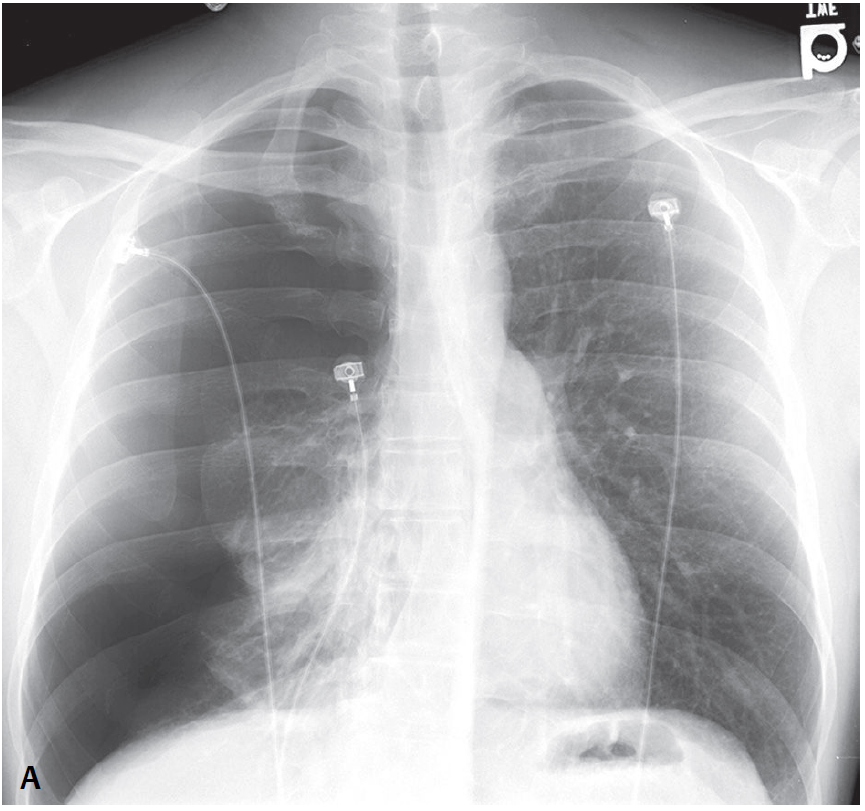
X-RAY QUIZ: Patient has lung cancer. Image 1 shows a right hilar mass. 4 months later (image 2) what complication has occurred?
A: Lung metastases
B: Phrenic nerve palsy
C: Right lower zone pneumonia
D: Right pleural effusion
E: Pneumothorax
Start Quiz https://t.co/RCicOlIpLB
Chest Xray ; There is complete opacification of the right hemithorax with mediastinal pull to the right. There is compensatory hyperinflation of the left lung with herniation across the midline to the right noted. No focal left lung lesion is seen.
Difficult to assess true cardiac size. The bony rib cage is normal.
Diagnosis; Right lung collapse/Atelectasis? Due to endobronchial tumor or foreign body .
In cases showing diffuse bronchiectasis related to infection (not traction bronchiectasis, which is a feature of fibrotic lung disease), it is important to remember that bronchiectasis itself is not a diagnosis. It reflects an underlying cause, and the radiologist should try to suggest that cause based on the pattern and distribution.
A practical first step is to assess whether the diffuse bronchiectasis is central or peripheral.
•Central bronchiectasis has a limited differential.
•With upper lobe predominance, consider cystic fibrosis and allergic bronchopulmonary aspergillosis.
•With lower lobe predominance, consider primary ciliary dyskinesia and immunodeficiency.
•Peripheral bronchiectasis also provides clues.
•Predominance in the right middle lobe and lingula suggests Mycobacterium avium complex infection.
•Lower lobe–predominant peripheral bronchiectasis may point toward rheumatoid arthritis–related airway disease.
Across these entities, diffuse bronchiectasis is often accompanied by tree-in-bud nodules and mucus plugging, reflecting active or recurrent infection.
👉 Based on these basic imaging principles and the provided videos, what is your diagnosis or differential diagnosis in this case?