Interventional Cardiology consultant letting their IC fellow do their first PCI.🤦🏾♂️ #MedTwitter#CardioTwitter#IC#ACCFIT
Source: https://t.co/EeJMF7QCGw
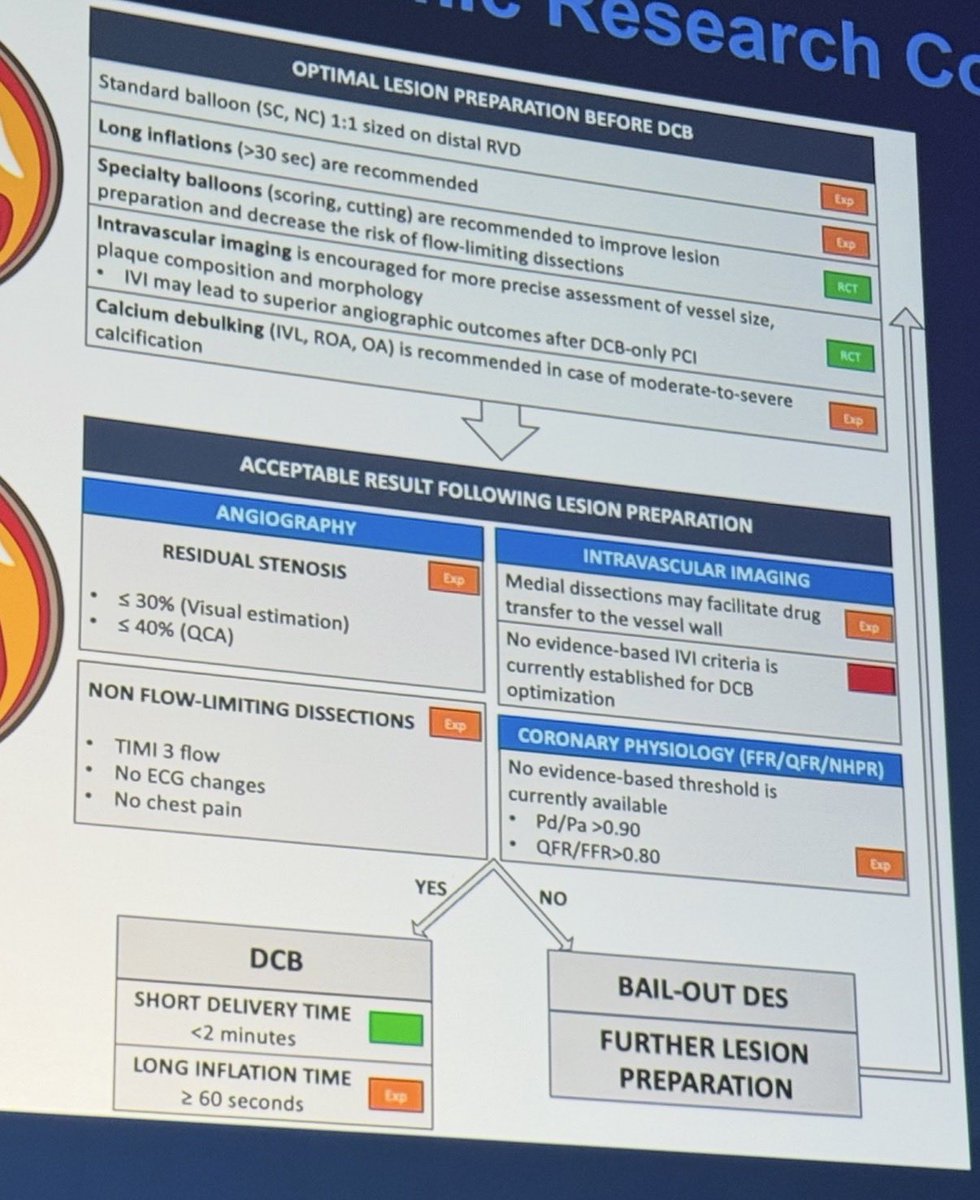
New insights for DCB:
• Prolong pre-dilation inflation.
• Start the timer once the DCB is loaded on the monorail and ready to be delivered.
• If not delivered within >2 mins, replace the DCB.
@crfheart#Fellows2026
Welcome to a a novel simple and easy-to-use 3D wiring technique for coronary CTOs named ZOLUTION: Zero OverLap View Universal Three dimensIONal wiring https://t.co/9FDWY29IUk @ccijournal
Welcome to the “skipping rope technique” for managing burr entrapment during rotational atherectomy, based on sequential counterclockwise rotational force is applied to the drive shaft, generating alternative torque dynamics https://t.co/sz8tj6y5my @ccijournal
#TCTAP2026@summitmd_cvrf
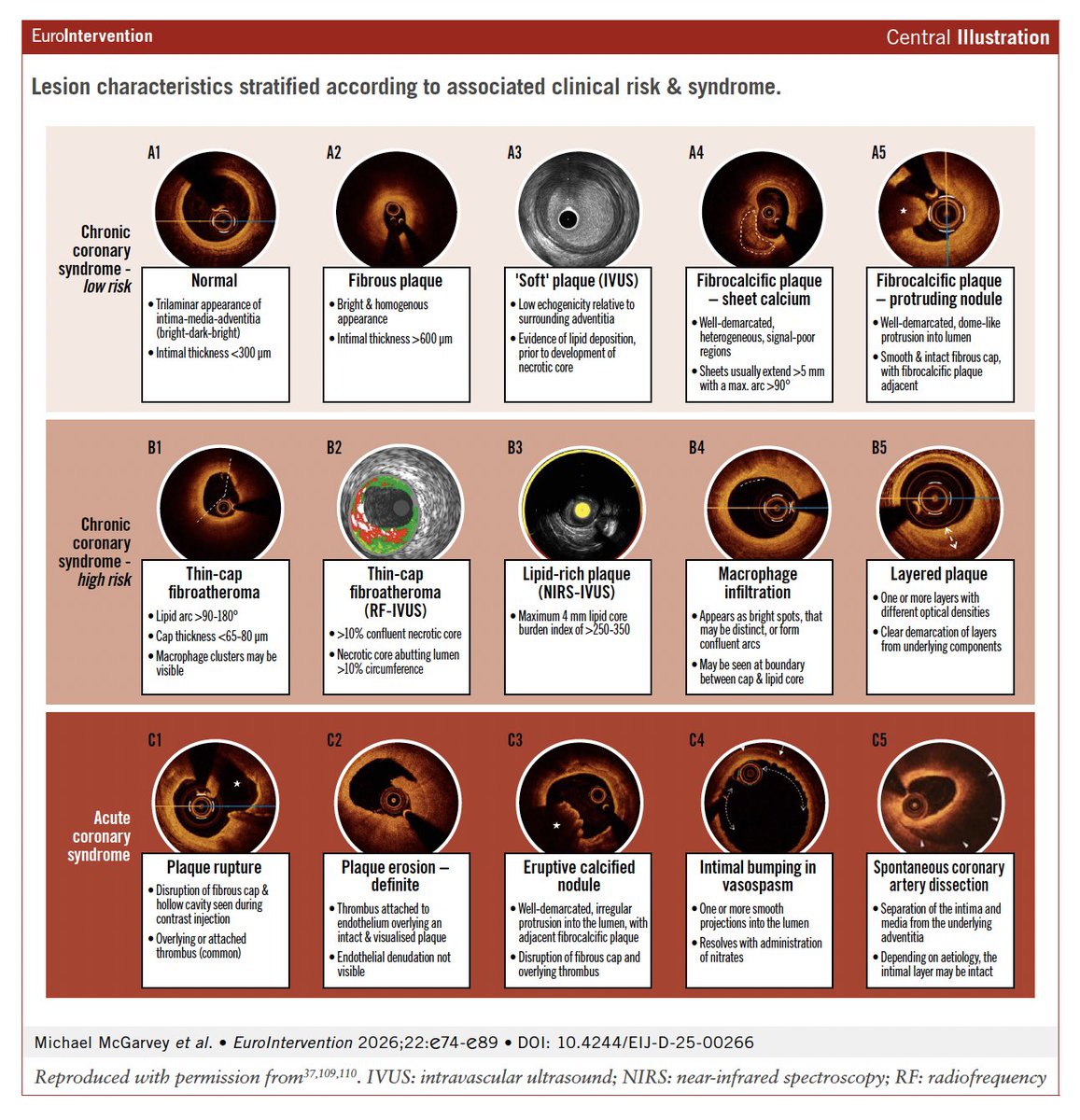
❤️🔥In-Stent Restenosis and Neointimal Calcification: From Risk Factors to Treatment
💥Different patterns of Neoatherosclerosis as seen on IVI/OCT 👇
How to correct incomplete crush and how to prevent lack of carina coverage
Episode 2⃣ of this series on "How to perform DK-Crush for left main bifurcation stenting" is now online!
📺https://t.co/5sg3uk19Tu
In this episode, learn about:
🟣Differentiating between complete and incomplete crush
🟣The importance of sequential crush and bigger balloons, adequately sized according to proximal vessel diameter
Includes an additional analysis by @GoranEBC & William Wijns.
@twj1974@NievesGonzalo1@BURZOTTA_F@M_Lesiak@gabor_gt@RhianEDavies1@esbrilakis@VisibleHeartLab
#interventionalcardiology #CardioEd #EuroPCR
With great pleasure we report metaanalysis of 5 trials including LEMANS at 10 year follow-up in @JACCJournals. There is no difference in mortality between PCI and CABG for left main disease. In fact its identical : 23.4% vs 23.3%, HR 1.02 (0.89–1.17), RMST difference of exactly 0.0 years. Those are outcomes still with BMS and rare IVUS. Not bad! Great news for the patients. @GreggWStone@Hragy@SerruysPatrick@ZSiudak@EAPCIPresident@AHP_PAKS@uniwersytet_afm Thank you David Koeckerling and Ahmad Yosif.
https://t.co/Kk9cy8v11o
Koeckerling et al. just dropped in @JACCJournals: a reconstructed-IPD meta-analysis of all 5 RCTs comparing PCI vs CABG for left main disease (LE MANS, SYNTAX, PRECOMBAT, EXCEL, NOBLE). 4,499 patients pooled. The headline: 10-year all-cause mortality is virtually identical — 23.4% vs 23.3%, HR 1.02 (0.89–1.17), RMST difference of exactly 0.0 years.
This is genuinely good news. For patients with left main disease and low-to-intermediate anatomic complexity who are eligible for both strategies, we can now tell them with reasonable confidence: your chances of being alive at 10 years are the same regardless of which path you choose.
The methodology deserves praise. The team used reconstructed time-to-event IPD (via the IPDfromKM algorithm) with 98.7% fidelity, pooled in a 1-stage Cox model with γ-frailty for trial, verified proportional hazards (Schoenfeld P=0.59), ran RMST as a complementary analysis, and confirmed everything with conventional fixed/random effects meta-analysis. Every approach converges to the same number. That's reassuring.
But as with any meta-analysis, the fine print matters. A few observations:
𝗧𝗵𝗲 𝗘𝗫𝗖𝗘𝗟 𝗾𝘂𝗲𝘀𝘁𝗶𝗼𝗻
EXCEL is the largest trial (n=1905, 23% of the weight) and the only one with contemporary 2nd-gen DES (everolimus). It's also the only trial censored at 5 years — no 10-year follow-up, none planned. And it was the only trial showing a statistically significant excess in all-cause mortality with PCI at 5 years (13.0% vs 9.9%, difference 3.1 pp).
@GreggWStone et al. themselves wrote in NEJM 2019: "at this time point the hazard curves were continuing to diverge. Ten-year follow-up is needed."
Administrative censoring at 5 years is statistically valid — it doesn't bias the HR within the observed window. But it removes the possibility of detecting whether the divergence continued or reversed. The other 4 trials that DO have 10-year data all used 1st-gen DES or BMS. So the question "what happens to everolimus-eluting stents in left main at 10 years?" remains genuinely unanswered.
𝗥𝗲𝗰𝗼𝗻𝘀𝘁𝗿𝘂𝗰𝘁𝗲𝗱 𝗜𝗣𝗗 ≠ 𝘁𝗿𝘂𝗲 𝗜𝗣𝗗
The reconstruction method is validated and reliable for time-to-event data. But it cannot recover individual covariates. This means the meta-analysis cannot test treatment-by-subgroup interactions for diabetes, acute coronary syndromes, or SYNTAX score at 10 years. The Sabatine et al. IPD meta-analysis (Lancet 2021) found no interaction at 5 years — but extrapolating that to 10 years is an assumption, not a finding.
This matters because the NOBLE 10-year paper (Holck et al., Lancet 2026) found a significant interaction between ACS presentation and mortality (HR 0.57 favoring PCI in ACS, p_interaction=0.049). If confirmed, this would have major practical implications. But it couldn't be tested in the pooled analysis.
𝗠𝗼𝗿𝘁𝗮𝗹𝗶𝘁𝘆 𝗲𝗾𝘂𝗮𝗹 ≠ 𝗼𝘂𝘁𝗰𝗼𝗺𝗲𝘀 𝗲𝗾𝘂𝗮𝗹
The meta-analysis only reports mortality. No MI, no stroke, no repeat revascularization. This is a deliberate and defensible choice (mortality is the hardest endpoint, immune to ascertainment bias). But it leaves the conversation incomplete.
As an exercise, I pooled the 3 trials that report non-mortality endpoints at their longest available follow-up (LE MANS 10yr, PRECOMBAT 10yr, EXCEL 5yr — ~2,610 patients). Exploratory, not definitive, but informative:
→ Repeat revascularization: RR 1.66 (1.36–2.03). Significantly and consistently higher with PCI. No surprise — but the magnitude matters for shared decision-making.
→ Total MI: RR 1.12 (0.87–1.46). Apparently neutral. But EXCEL shows why this is misleading: periprocedural MI favored PCI (RR ~0.66) while spontaneous MI favored CABG (RR ~1.92). They cancel out in the composite. Classic Simpson's-adjacent phenomenon — the total hides a divergence that matters clinically.
→ Spontaneous MI (EXCEL-driven): RR 1.64 (1.14–2.38), P=0.008. This is the trade-off the patient needs to hear. CABG appears to protect better against late spontaneous infarction — plausibly because grafts bypass vulnerable proximal plaques that stents don't address.
Caveat: SYNTAX and NOBLE didn't collect these endpoints between 5–10 years, so this analysis is incomplete. It's a conversation starter, not a conclusion.
𝗛𝗼𝘄 𝗱𝗼𝗲𝘀 𝗢𝗣𝗧𝗜𝗠𝗔𝗟 𝗳𝗶𝘁 𝗶𝗻?
The OPTIMAL trial (Testa et al., NEJM 2026) just showed that IVUS-guided PCI adds no benefit over angiography-guided PCI in left main (HR 1.11, 0.87–1.42). This seems to contradict the NOBLE IVUS substudy (20% vs 31% mortality with/without final IVUS).
But there's no contradiction. The NOBLE observation was confounded by indication. OPTIMAL randomized the comparison and found that in expert hands — operators who already internalize IVUS-derived optimization criteria — the imaging itself doesn't add incremental value. The control arm had 96% post-dilation rates and 85% POT. That's not "angiography-naïve" PCI — it's PCI done by people who think with IVUS even when they don't use it.
This actually reinforces the Koeckerling findings: PCI in the included trials, even without mandated imaging, achieved equivalent mortality to CABG. If even IVUS doesn't move the needle in expert centers, then the mortality equivalence reported in the meta-analysis is likely robust and not contingent on a hypothetical "better PCI."
𝗧𝗮𝗸𝗲-𝗮𝘄𝗮𝘆
My thoughts:
1. PCI and CABG offer the same probability of being alive at 10 years in patients with left main disease and SYNTAX ≤32. This is established.
2. But equal survival is not the same as equal outcomes. PCI means ~66% more repeat revascularization and likely more spontaneous MI. CABG means more periprocedural stroke and a harder early recovery.
3. The choice isn't about which is "better." It's about which set of trade-offs aligns with the patient sitting in front of you — their anatomy, their comorbidities, their values, their fear of surgery vs. their tolerance for reintervention.
Equal mortality is the foundation. The rest is shared decision-making. Again, kudos to the authors. This is beautiful work!
#CardiologyX #InterventionalCardiology #LeftMain
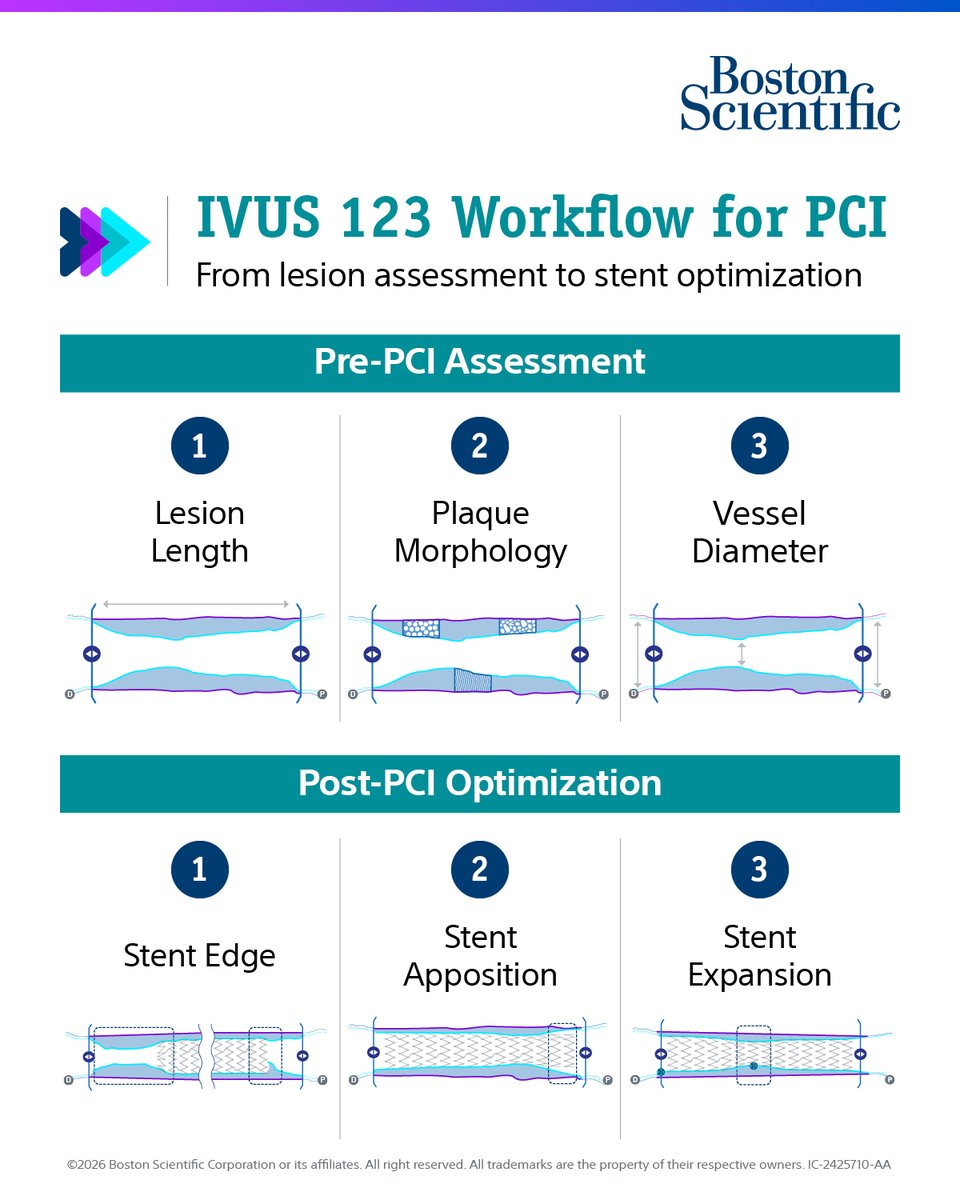
Improved IVUS-guided PCI outcomes support critical clinical decisions.
In a recent publication, Dr. Simon Walsh outlines the IVUS 123 Workflow, a simplified, standardized approach designed to support intuitive decision-making, reproducibility, and long-term PCI durability.
📄Read more: https://t.co/A3H9tfj7Fw
Want a FREE registration for #EuroPCR? 👀
Submit your case to the PCR Fellows Course – the best 3 cases will present in the fellow course and get free registration to EuroPCR.
Showcase your work on a global stage.
@PCRonline@kiadeb87@ANazmiCalik
🔗 https://t.co/A79x8ifetz
In this new State-of-the-art paper, the authors review the evidence and guideline support for intracoronary imaging in contemporary clinical practice, and outline a modern, imaging-driven approach to PCI planning.
https://t.co/YUCGlkT9Et
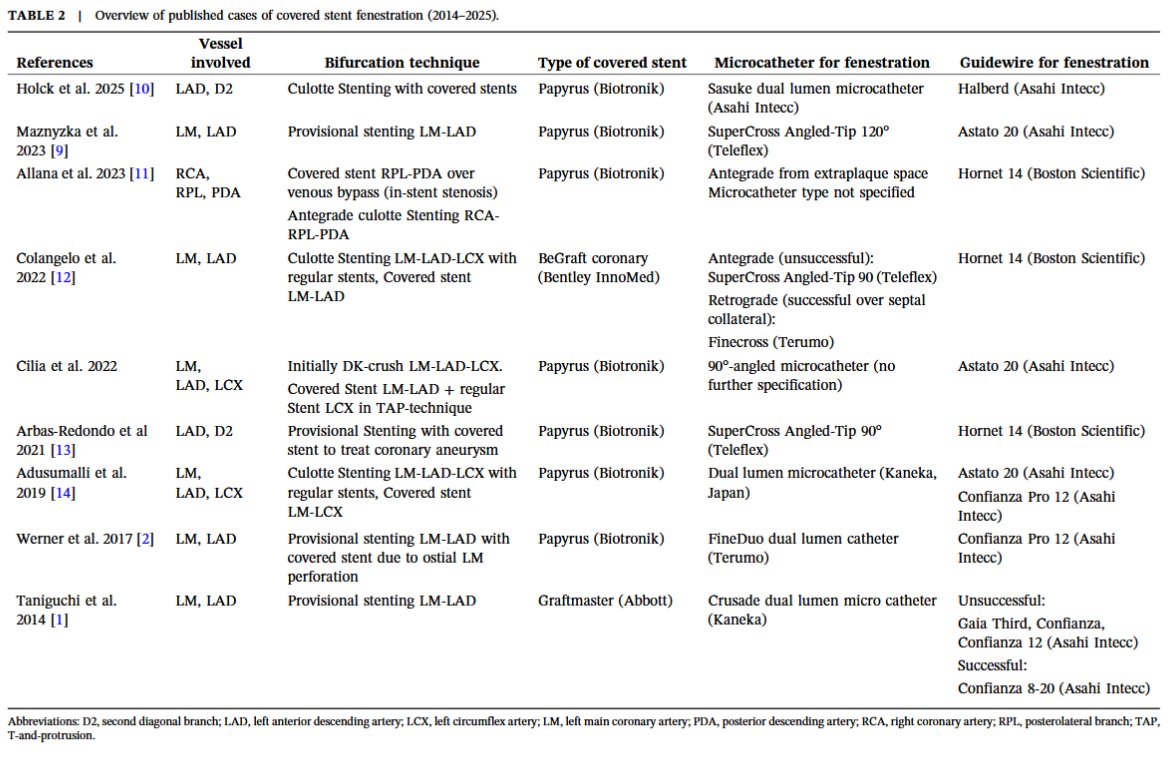
Must-read tutorial on treatment of coronary perforations in bifurcation lesions with a two-stent strategies using fenestrated covered stents, just published in Catheterization & Cardiovascular Interventions https://t.co/qdyRv52LcY @ccijournal
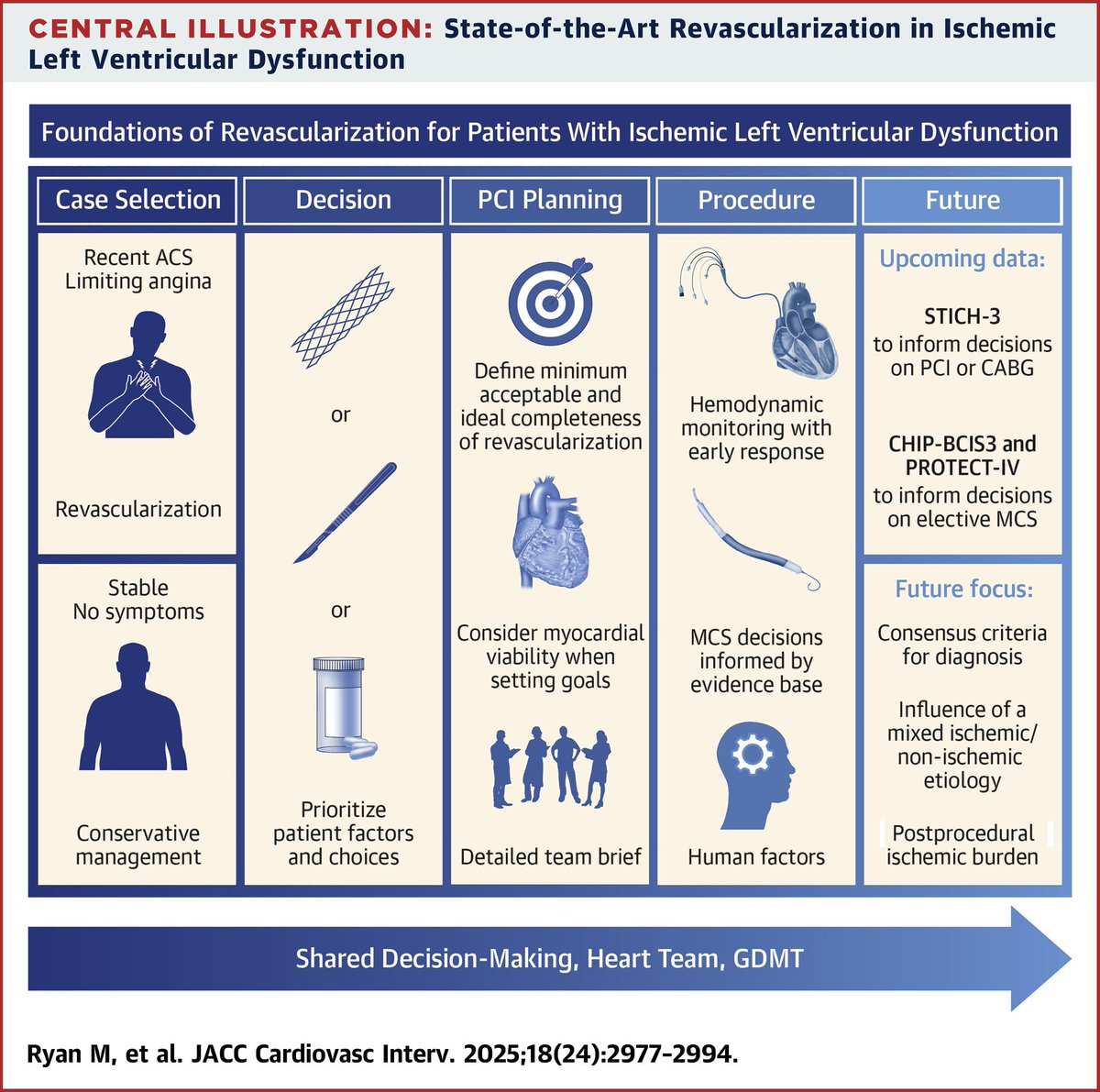
Revascularization in severe LV dysfunction: State of Art paper just out in @JACCJournals@ACCinTouch https://t.co/8eGgL88mbj
CABG or PCI or OMT?
When to use MCS?
Does RHC help?
Pre-procedure planning
Ideal teams/skill sets
Major upcoming trials
https://t.co/HIUmujjxWX
Decisions in complex left main PCI – Left main trifurcation
📺https://t.co/r4lhai4lth
Watch this session replay for an in-depth analysis of complex LM trifurcation PCI, from evaluation through imaging and physiology, lesion preparation strategies, and treatment options including stepwise provisional approaches, upfront two-stent techniques, and DCB!
A. Al Nooryani, F. Malik, O. Al Shammeri, @MPAOSS@BURZOTTA_F, U. Kaul
#EuroPCR #interventionalcardiology
This paper from the European CTO Club provides a comprehensive overview of contemporary interventional management of heavily calcified CTOs, suggesting an integrated diagnostic and therapeutic approach to guide the choice between the available options. https://t.co/QQqye7GPrZ
The Ultimate CPET Thread
How to Decode Dyspnea Using Physiology (Braunwald + Clinical Insights)
CPET is not just a stress test, It is a complete physiologic study of the heart, lungs, and muscles working together under stress
A 🧵
Calcium Challenge – Tackling Rings, Nodules and Plates: How Can We Get More from Intravascular Lithotripsy Technology?
#CalcifiedPCI#IVL@radcliffeCARDIO
🔗 https://t.co/Wzj10Abth6
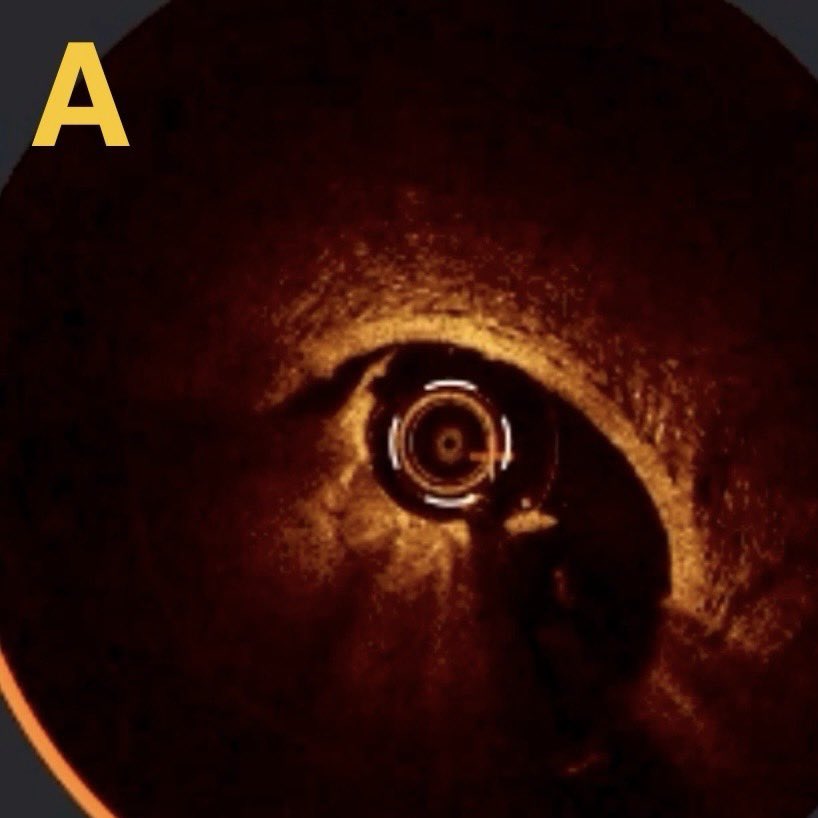
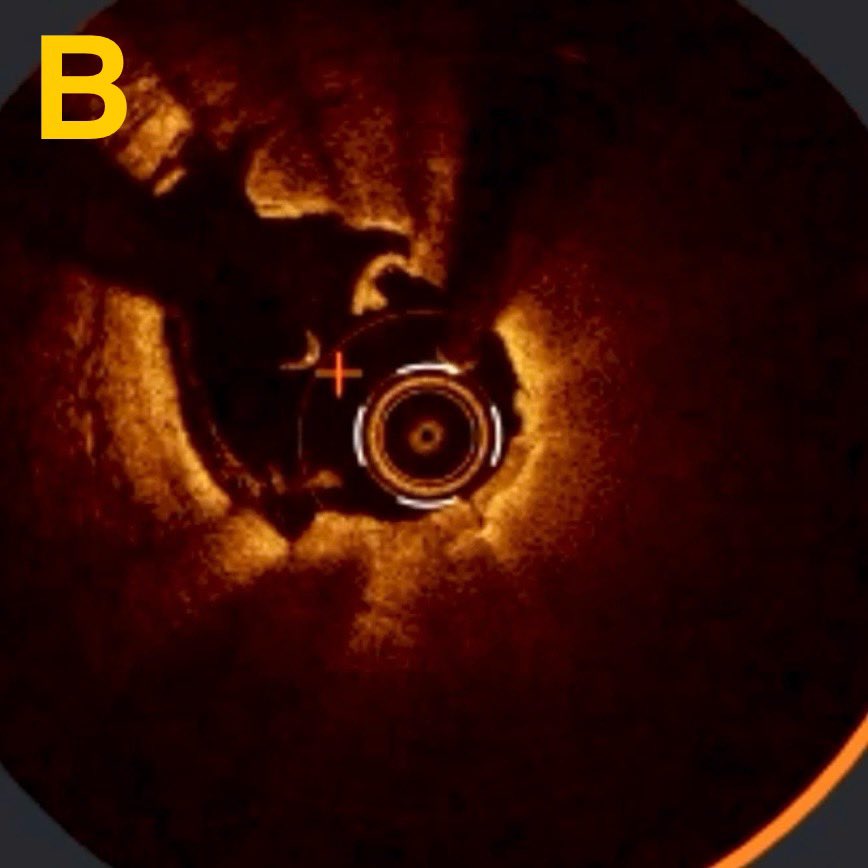
Dissection vs. Dissection
All dissections are not the same. Some can be left alone to heal over time, while others demand more immediate attention.
IVUS and OCT can reveal important features not seen by angio.
How would you treat each of the lesions seen after CBA in a LCX?
My answers in the ‘near future’. Or sooner if this post goes viral! 😂
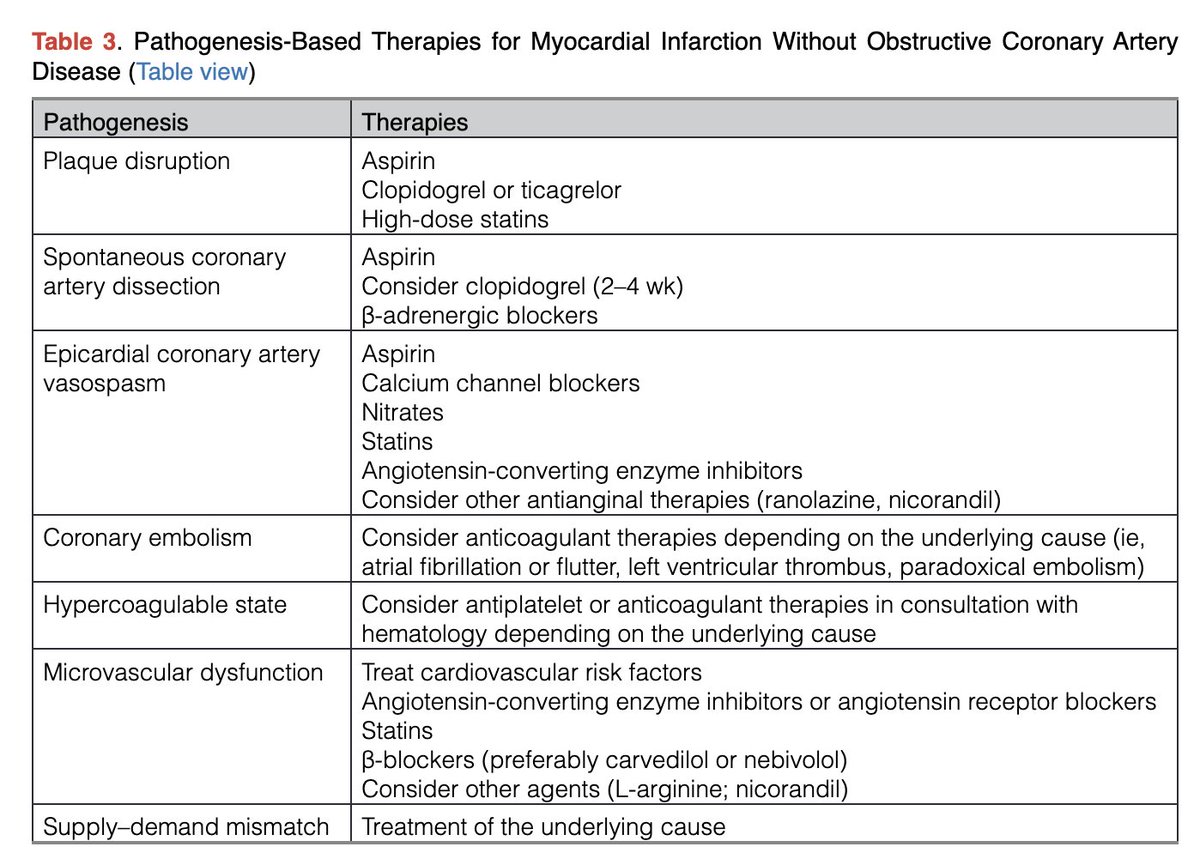
🔴State of the Art: Evaluation & Medical Management of Nonobstructive Coronary Artery Disease in Patients With Chest Pain: A Scientific Statement @CircAHA#Cardiology#CardioEd#FOAMed#AHA2025
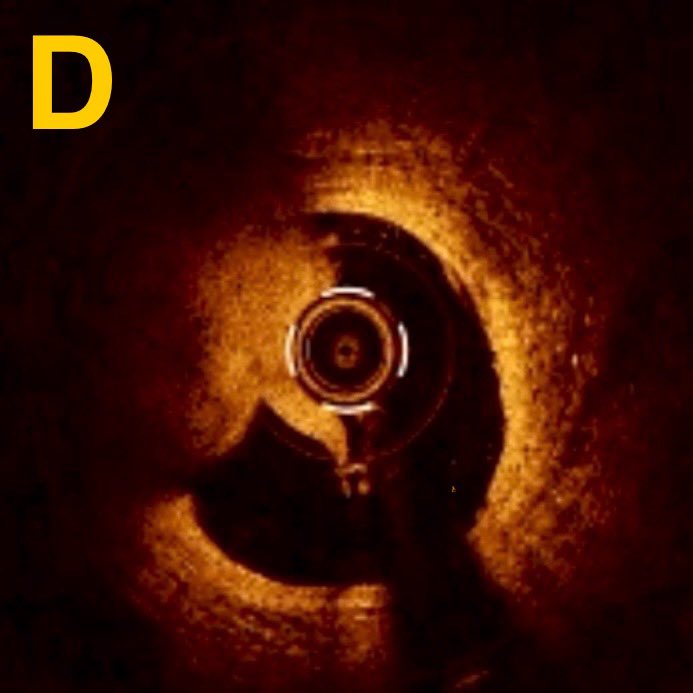
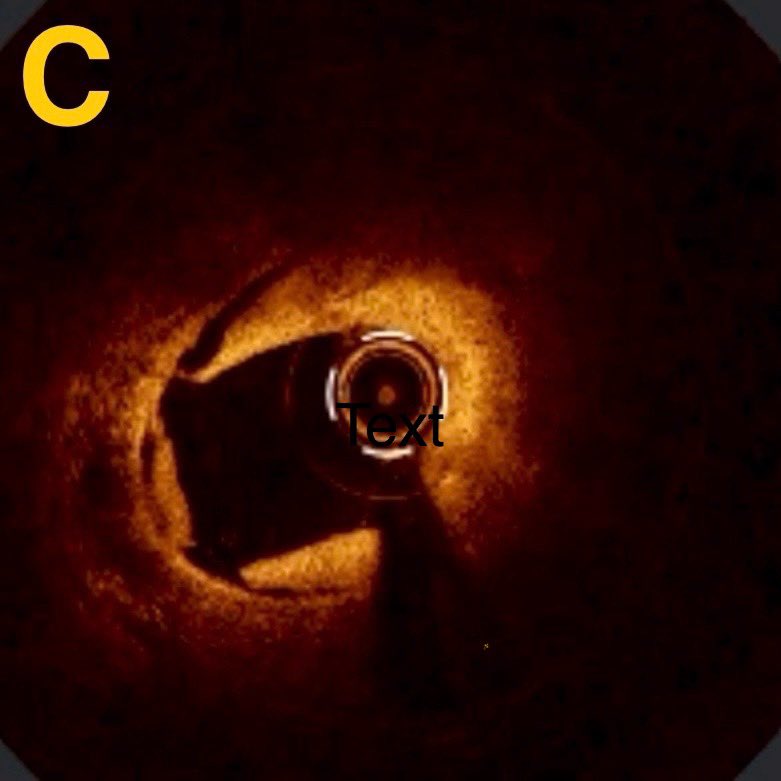
My Best OCT Image! 🧶
This image is ‘one in a million’ - literally, because I looked at 100s of 1000s of imaging frames this week. 😂
This shows the final appearance of an LCX treated with scoring PTCA, NC 🎈, and DCB.
Analysis to follow…