Listen up!
Trying to get into a rhythm on how to approach pulsatile tinnitus?
Does pulsatile tinnitus get your heart racing?
This week’s @theAJNR SCANtastic has all you need to know!
https://t.co/BTI94N5Wsk
Pulsatile tinnitus is caused by turbulent blood around the petrous bone!
It’s like traffic: if you alter the flow of traffic, you will start to hear some noise & horns!
So what causes turbulent traffic?
1. Complex traffic patterns
If the roads are crazy, people get confused and drive crazy. Same w/flow from:
--AVMs
--dAVFs
--Tumors
--Diverticula
2. Diverted traffic
Nothing causes more chaos than making people go a different way than normal. Variant flow anatomy can cause pulsatile tinnitus:
--Large mastoid emissary veins
--Large occipital sinus.
3. Blockage of traffic!
If there is an accident, there is turbulence as people try to get around. For flow, blockages are stenoses:
--Carotid stenosis
--Transverse/sigmoid sinus stenosis
--Jugular stenosis
In this month’s @theAJNR, Zhang et al. found jugular stenoses were equally prevalent in both controls & pts w/pulsatile tinnitus
It raises the question if should we treat jugular stenosis!
Now hopefully your heart won’t skip a beat when you see a case of pulsatile tinnitus!
Follow @theAJNR and check it out for yourself:
https://t.co/BTI94N5Wsk
Feeling unarmed when it comes to evaluating cervical radiculopathy & foraminal narrowing on MR?
Think of the nerve root like a hot dog, sitting between the two buns of the disc/uncovertebral joint & facet.
The more you put in your hot dog, the more the hot dog itself is squished. Same w/the nerve root.
Spurring & degenerative change are like the extra topping that push on the hot dog inside the buns.
A small amount of toppings/degenerative change, leaves the hot dog space. But if you pile on fixings, then the hot dog is taken over.
Ask yourself--how is my hot dog doing?
Mild stenosis is like just a little ketchup & mustard on the bun but hot dog still has space.
Moderate stenosis is when you aren’t just putting on sauce, you are adding things that take up space, like relish.
But there’s only so much relish one can put on, so it doesn’t take up more than half the bun.
Severe stenosis is like a chili cheese dog, where the hot dog is smothered & it has no room in the bun away from the chili or cheese. Here the narrowing is greater than 50%
This is the Kim classification & has strong correlation w/symptoms I like it bc it doesn’t require calipers to estimate a >50% narrowing
So now you know how to both image and assess stenosis in the cervical neural foramen.
Now hopefully rating cervical foraminal narrowing won’t be a pain in the neck!
Most of us were taught to classify large artery stroke by the vessel.
Carotid.
MCA.
Basilar.
Vertebral.
But that approach often doesn't tell us what to do next.
The more useful question is:
What is the mechanism behind the artery?
When I review a CTA after the acute phase, I try to answer only 4 questions:
① Is the artery throwing clots?
Think:
• carotid plaque
• vertebral plaque
• artery-to-artery embolism
The prevention strategy often revolves around antiplatelets, statins and consideration of carotid intervention.
② Is the artery itself diseased?
Think:
• symptomatic intracranial stenosis
• MCA disease
• basilar disease
The focus shifts toward aggressive medical therapy and vascular risk-factor control.
③ Is the brain losing flow?
Think:
• watershed infarcts
• limb-shaking episodes
• BP-dependent symptoms
• dehydration-related worsening
Sometimes the problem is not embolism.
It is perfusion.
④ Is this even atherosclerosis?
Think:
• dissection
• vasculitis
• Moyamoya
• cancer-associated stroke
• other vasculopathies
Treating the stenosis alone won't solve the problem.
The cause matters.
The Large Artery Stroke Passport
CTA tells you WHERE.
The mechanism tells you WHY.
Secondary prevention tells you WHAT TO DO NEXT.
#Stroke
#StrokeNeurology
#NeuroTwitter
#MedTwitter
#Neurology
#VascularNeurology
#StrokeMedicine
#NeuroEducation
Time is brain!
So you don’t have time to struggle w/that stroke alert head CT.
Here’s are the FIVE main the CT findings in acute stroke.
--Hyperdense artery sign
Occurs when you see the thrombus in the artery.
Thrombus appears hyperdense bc clot is denser than normal flowing blood—& CT is just a measure of density.
--Blurred basal ganglia/lentiform nucleus.
Usually this region is a triangle of low density white matter surrounding the high density lentiform nucleus
In an acute infarct, this triangle becomes blurred, bc the lentiform nucleus becomes edematous & similar in density to white matter.
--Hypodense regions of brain
When O2 & ATP run out, Na/K pump stops working
Osmotic gradient causes Na & H20 rush into the cell.
More water in the cell = lower density. For every 1% increase in H20 there is a 2.5 HU decrease in density
Means damage is irreversible
--Insular ribbon
Insula is an internal MCA watershed between the lenticulostriates & M2 sylvian branches
Infarcts relatively early with low blood supply & becomes a low density ribbon
--Sulcal effacement
Normally, brain has sulci that look like ice cracks/crevasses along its surface.
As water accumulates in dead cells, swelling occurs, & the crevasses are effaced by the swollen brain
So now you know the 5 main signs of acute infarct on CT—remember, if you see these five, soon that brain won’t be alive!
🧠⚡ Epilepsy is more than just seizures.
It’s a disorder of abnormal electrical activity in the brain that can affect consciousness, movement, memory, and quality of life.
Recognizing the signs early can save lives. 🚨
🔹 Focal vs generalized seizures
🔹 EEG & MRI diagnosis
🔹 Emergency management of status epilepticus
🔹 High-yield treatment overview
Every doctor and medical student should know these basics. 👨⚕️📚
#Epilepsy #Neurology #MedTwitter #FOAMed #MedicalEducation #Medicine #NeuroTwitter #Seizure #Doctor #MedEd
Key movement patterns seen in basal ganglia lesions
High-yield review: chorea, athetosis, ballismus, tremor & parkinsonism
If you found this helpful, like, share, and follow for more high-yield medical content
Most anticoagulation mistakes in stroke happen because we ask:
Which anticoagulant should I use?
before asking:
Does this stroke even deserve anticoagulation?”
Stroke anticoagulation is not a prescription.
It is AIR TRAFFIC CONTROL.
Every stroke subtype is a different aircraft.
And every aircraft does NOT get runway clearance.
🟢 GREEN RUNWAY
These are thrombin-rich strokes.
✔ AF-related stroke
→ DOAC usually preferred
✔ Mechanical valve
→ Warfarin only runway
✔ Rheumatic MS + AF
→ Warfarin tower
✔ LV thrombus
→ Usually 3–6 months
✔ Cerebral venous thrombosis
→ Heparin first, even if venous hemorrhagic infarct exists
✔ APS-related stroke
→ Warfarin dominates
✔ Cancer/NBTE stroke
→ LMWH often preferred
These are not aspirin diseases.
🟡 YELLOW HOLDING PATTERN
Not every AF stroke should receive immediate anticoagulation.
Before takeoff:
• How big is the infarct?
• Any hemorrhagic transformation?
• BP controlled?
• Platelets safe?
• Mass effect?
• ICU instability?
• Post-thrombectomy status?
ELAN and OPTIMAS changed the conversation:
Small stable infarct?
Earlier DOAC may be safe.
Large infarct?
Delay may save the brain.
Timing is neuroimaging plus judgment.
Not calendar mathematics.
🔴 RED NO-FLY ZONE
Do NOT empirically anticoagulate:
Lacunar stroke
Atherosclerotic stroke
Most ESUS
Routine AIS <48h
Infective endocarditis embolic stroke
NAVIGATE-ESUS and RE-SPECT ESUS reminded us:
“Cryptogenic” is not a license for DOAC.
🚨 WHEN BLEEDING HAPPENS
The first drug is not PCC.
The first drug is:
STOP.
Then:
→ CT brain
→ INR / renal function / platelets
→ Identify last dose
→ Reverse selectively
→ Reassess mechanism
Because the hardest question in stroke anticoagulation is not:
What should I start?
It is:
When should I restart?
AHA/ASA.
ELAN.
OPTIMAS.
Modern CVT guidance.
The era of one anticoagulation rule for all strokes is over.
Treat the mechanism.
Not just the MRI.
#Neurotwitter #Medtwitter #Stroke #Anticogulation
Patient enters OPD.
MRI normal.
No major weakness.
No clear cerebellar signs.
But he says:
Doctor, I am okay sitting.
Problem starts while walking.
Especially in darkness.
Think bilateral vestibulopathy.
Most patients do not complain of spinning vertigo.
They complain of:
• imbalance
• bouncing vision while walking
• falls
• supermarket dizziness
• instability on uneven ground
The OPD key is simple:
Fine sitting.
Unsafe moving.
3 questions help immediately:
• Worse in darkness?
• Does the world bounce while walking?
• Better while sitting still?
If yes, stop calling it vague dizziness.
Oscillopsia is the bedside gold clue.
Patients describe it beautifully:
• road shakes
• faces blur
• letters bounce while walking
Now the modern approach is different.
Not just bilateral vestibular weakness.
Find the phenotype:
• gentamicin toxicity
• cisplatin injury
• Ménière’s disease
• CANVAS / RFC1
• FGF14
• neuropathy overlap
• cerebellar syndromes
Examination should not stop at Romberg.
Check:
• dynamic visual acuity
• tandem gait
• gait with head turns
• bedside HIT
• hearing
• neuropathy signs
And remember:
A normal bedside HIT can still miss disease.
What actually helps patients?
Not long-term vestibular suppressants.
But:
• vestibular rehabilitation
• gaze stabilization
• fall prevention
• darkness navigation training
• avoiding ototoxic drugs
Bilateral vestibulopathy is not a sitting disease.
It is a moving disease.
#Neurotwitter #Medtwitter #Vertigo
🧠⚡ Wernicke Encephalopathy is a medical emergency that is often MISSED.
A simple deficiency of vitamin B1 can rapidly lead to:
➡️ Confusion
➡️ Ataxia
➡️ Eye movement abnormalities
➡️ Permanent neurologic damage
🚨 Always think of it in:
• Chronic alcohol use
• Malnutrition
• Persistent vomiting
• Bariatric surgery patients
💉 Golden rule:
THIAMINE BEFORE GLUCOSE whenever possible.
Early recognition can completely reverse the disease. Delay can lead to irreversible Korsakoff syndrome.
#MedTwitter #Neurology #MedicalEducation #EmergencyMedicine #InternalMedicine #FOAMe
Antiplatelet therapy after stroke is not:
Aspirin for everyone.
DAPT for everyone.
Or clopidogrel because the patient had a stroke on aspirin.
It is a 3-question decision.
What is the mechanism?
What is the clock?
What is the bleeding risk?
That is the whole game.
Minor non-cardioembolic stroke or high-risk TIA, early presentation, low bleeding risk?
Think short DAPT.
Aspirin plus clopidogrel.
Usually 21 days.
Then single antiplatelet.
Not 3 months by habit.
Not lifelong because the first prescription was never reviewed.
Mild to moderate stroke or high-risk TIA with selected high-risk features?
Ticagrelor plus aspirin may enter the discussion.
But it is not simply stronger clopidogrel.
It is a selected-patient decision, with bleeding and dyspnoea on the other side of the scale.
Severe symptomatic intracranial stenosis?
This is the 90-day exception.
Aspirin plus clopidogrel may be justified, but only as part of aggressive medical therapy:
statin, BP, diabetes, smoking, lifestyle.
DAPT alone is not a treatment plan.
Lacunar stroke?
Respect SPS3.
Long-term aspirin plus clopidogrel is not wisdom.
It is bleeding dressed as prevention.
ESUS?
Do not guess with anticoagulation.
Start antiplatelet, investigate properly, and reclassify the mechanism when evidence appears.
AF-related stroke?
Antiplatelet therapy is not enough.
The patient needs an anticoagulation strategy when safe.
Stroke on aspirin?
First ask:
Was it really aspirin failure?
Or was it:
missed AF,
intracranial stenosis,
carotid plaque,
non-adherence,
wrong dose,
cancer-associated stroke,
or uncontrolled risk factors?
Never escalate before you re-diagnose.
The clean bedside rule:
DAPT is a bridge.
SAPT is the destination.
Anticoagulation is a different road.
Mechanism decides the map.
In stroke prevention, the most dangerous antiplatelet error is not choosing the wrong tablet.
It is forgetting to write the stop date.
#Neurotwitter #MedX #Stroke #Aspirin
Most temporal lobe seizures are not localised by one symptom in OPD.
Not by déjà vu.
Not by lip smacking.
Not by one abnormal EEG line.
They are localised by watching the seizure movie in order.
Think of TLE as a subway map.
Station 1: Aura Gate
Ask: what happened first?
Rising epigastric sensation, fear, déjà vu, smell or taste aura
Think mesial temporal.
Auditory buzzing, ringing, vertigo, sound in one ear
Think lateral temporal.
Station 2: Consciousness Station
When did the patient stop responding?
Temporal seizures often build gradually and leave confusion behind.
Absence is brief.
Frontal can be abrupt and dramatic.
Tempo matters.
Station 3: Automatism Junction
The mouth says temporal.
The hands may tell the side.
Lip smacking, chewing, swallowing
Temporal network.
Manual automatisms
Often ipsilateral.
Dystonic stiff arm
Contralateral.
One OPD question can be gold:
Which hand was fumbling, and which arm became stiff?
Station 4: Lateralisation Signal Box
Dystonia, clonus, forced version
Opposite hemisphere.
Postictal nose wipe
Same side.
Aphasia or postictal dysphasia
Dominant hemisphere.
Ictal speech or vomiting
Often non-dominant, but interpret with caution.
Station 5: Temporal-Plus Trap Exit
Some seizures only look temporal.
Think insula, operculum, orbitofrontal or TPO network when there is:
throat tightness
painful aura
perioral sensory symptoms
early hypermotor behaviour
discordant MRI, EEG and semiology
failed temporal surgery
The temporal lobe may be the platform.
The train may have entered from another line.
OPD rule worth saving:
Localise TLE by the movie:
First symptom
tempo
automatisms
lateralising signs
postictal language
EEG/MRI concordance
Not one sign.
The whole seizure sequence. #Neurotwitter #Medtwitter #TLE
🧠 COMPLETE NEUROLOGICAL EXAMINATION — A Systematic Clinical Approach 🩺
A good neuro exam doesn’t just detect disease…
It LOCALIZES the lesion. 📍
From cranial nerves 👁️ to motor power 💪, reflexes 🔨, sensation ✋, cerebellar signs 🎯, gait 🚶, and UMN vs LMN findings — this thread covers the essentials every medical student & doctor should know.
📌 High-yield. Clinical. Exam-oriented.
Save it. Revise it. Use it on rounds. 🔥
#Neurology #NeuroExamination #CranialNerves #ClinicalMedicine #MedTwitter #FOAMed #MedicalEducation #MBBS
Clinical Video for discussion
🔸60-year old lady presented with shivering (tremors) of both hands, predominantly affecting the left hand, for 10 years.
🔸There is no history of slowness of movements of rigidity.
🔸She is a known hypertensive, currently taking metoprolol for the same.
1. Describe the clinical findings.
2. What is the likely diagnosis?
#MedTwitter #NeuroTwitter
🚨 Burning Vertex Syndrome: A novel headache 🔥
A common problem in the Neurological OPD, well described by our colleague Pravin Thomas et al
🧠 Curr Opin Neurol 2025
➡️ Episodic, burning pain localized to the vertex (10–20 cm zone)
➡️ Mostly affects women (~65%), avg. age ~41
➡️ Duration: 1 min to 24 hrs, often <4 hrs
➡️ Frequency: daily to 1–3x/week
⚠️ Associated features in 76%:
•Nausea, vomiting
•Photophobia/phonophobia
•Autonomic signs
•Localized warmth (rare)
🧬Hypothesized mechanism? Small fiber scalp neuropathy
💉 Interesting finding: GON block helped in 2 patients
#NeuroTwitter #Headache
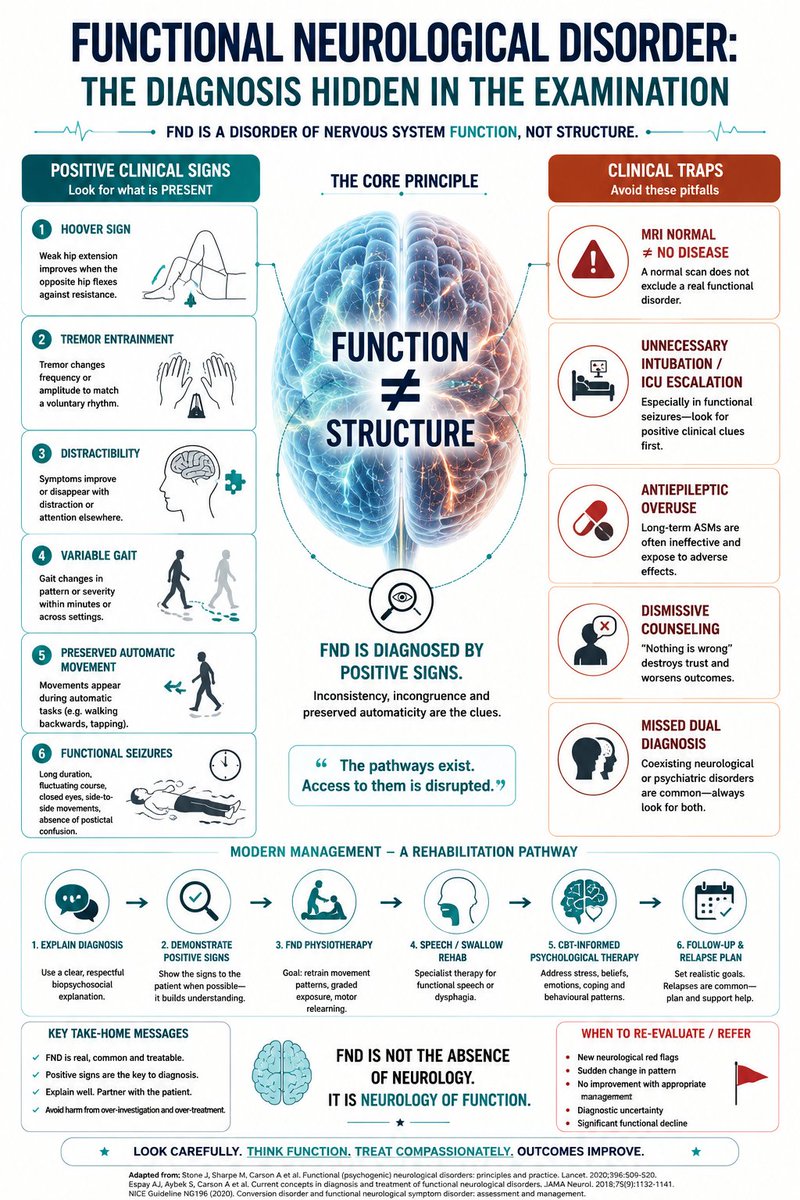
FUNCTIONAL NEUROLOGICAL DISORDER
One of the most important diagnoses in neurology…
is often missed because clinicians are looking too hard at the MRI
and not hard enough at the EXAMINATION.
A patient says:
I cannot move my leg.
But then:
• Hoover sign appears
• gait changes with distraction
• tremor entrains
• strength returns during automatic movement
That is not nothing.
That is a POSITIVE neurological pattern.
Modern FND is no longer:
“Diagnosis of exclusion.”
It is a diagnosis of:
✅ inconsistency
✅ incongruence
✅ preserved automatic circuitry
✅ positive bedside signs
The nervous system pathway exists.
The brain is failing to ACCESS it normally.
That single shift changes how you examine the patient.
Hoover sign stops becoming a trick.
It becomes a window into motor control.
The patient CAN generate movement.
But voluntary access becomes disrupted.
And this is exactly why:
• distraction may improve weakness
• backward walking may normalize gait
• tremor changes rhythm
• functional seizures fluctuate dramatically
FND sits at the intersection of:
movement
attention
prediction
emotion
agency
and motor control.
The dangerous part?
Patients are often harmed from BOTH sides.
⚠️ One clinician dismisses:
Everything is psychological.
⚠️ Another escalates:
benzodiazepines
antiepileptics
ICU admissions
intubation
Especially in functional seizures.
Real expertise is knowing:
when to stop escalating,
without losing diagnostic vigilance.
The best FND clinicians do 3 things well:
1️⃣ Rule out dangerous neurological disease carefully.
2️⃣ Rule IN FND positively.
3️⃣ Explain the diagnosis respectfully.
Because the explanation itself becomes treatment.
One sentence changes the entire consultation:
🧠
“Your nervous system pathways are still present.
The problem is in how the brain is accessing control of them.”
Not:
“Nothing is wrong.”
Modern FND management is not:
“Reassure and discharge.”
It is:
• targeted physiotherapy
• movement retraining
• speech/swallow rehabilitation
• psychiatric comorbidity management
• nervous-system retraining
FND is not anti-neurology.
It IS neurology.
And perhaps one of the purest examinations of how the brain converts intention into movement.
#neurotwitter #Medtwitter #FND #Functionaldisorders
A TBM patient is doing better for 10–14 days.
Fever settling.
Sensorium slightly improved.
Family finally starts relaxing.
Then suddenly:
more headache
vomiting
new cranial nerve palsy
sodium falls
patient becomes drowsy again.
At that moment, many people think:
“The medicines are not working.”
But in TBM, that is often the wrong question.
Because there are actually two diseases happening together.
One is the infection itself.
The second is the brain’s inflammatory reaction to that infection.
And steroids are mainly aimed at the second problem.
That is the part which changed the way I started thinking about TBM.
Dexamethasone is not just an adjunct.
It is an attempt to stop inflammation from damaging the brain while anti-TB drugs are killing the bacilli.
The difficult part is that inflammation in TBM is not subtle.
It produces:
basal exudates
vasculitis
infarcts
hydrocephalus
arachnoiditis
tuberculomas
raised ICP
sometimes devastating paradoxical worsening.
Which is why a patient can worsen despite being on the correct anti-TB regimen.
And honestly, one of the most dangerous periods in TBM is not admission.
It is steroid tapering.
That is where many cases suddenly become confusing.
The scan may look worse.
The headache returns.
The family says:
“Doctor saab pehle better tha…”
And now comes the real bedside question:
Is this treatment failure?
Or is this inflammation declaring itself again?
Before jumping to MDR-TB or changing the whole regimen, I think TBM forces us to pause and systematically ask:
Could this be hydrocephalus?
A new infarct?
Hyponatraemia?
A seizure issue?
Poor adherence?
Drug toxicity?
Paradoxical reaction?
TBM-IRIS?
Alternative diagnosis?
That thought process probably matters more than memorising steroid doses.
Of course, steroids are important.
In HIV-negative TBM, evidence for benefit is strong.
In HIV-associated TBM, the picture is more complicated. Benefit is less certain, though major harm has not clearly emerged. And in HIV patients, cryptococcal meningitis always needs active exclusion before becoming too comfortable with steroids.
But another important thing I learnt over time:
Steroids do not solve the whole disease.
They do not drain ventricles.
They do not fix sodium.
They do not stop every seizure.
They do not replace repeat imaging.
They do not treat MDR-TB.
And they definitely do not replace neurocritical care.
TBM is one of those diseases where you realise medicine is not only about choosing the correct drug.
It is about understanding which process is hurting the brain today.
Sometimes it is the bacillus.
Sometimes it is the inflammation.
And sometimes, despite treatment, the inflammation becomes the louder disease.
That is why I have started thinking of dexamethasone in TBM not as a routine steroid…
…but as a temporary brake trying to slow a fire inside a closed skull.
And like every brake, it only works properly if somebody is still carefully driving the vehicle.
#Neurotwitter #Medtwitter