Don't miss the editorial "The Myth of Depth of Anesthesia Monitors: When a “Normal” Bispectral Index Does not Mean What You Think It Means" from Drs. Paul Garcia and Peter Goldstein
Anesthetic “depth” and quality can’t be reduced to a single value: BIS cannot reliably ensure both optimization and safety. Recognizing monitor limits and adjusting care will.
https://t.co/Ydpp8MOCZU
The June @ASAMonitor serves as a clinical roadmap to help anesthesiologists navigate the transition from intraoperative specialists to holistic “guardians of the aging brain.”
Find articles about:
🔸Safeguarding #BrainHealth
🔸#Neurocognitive assessment
https://t.co/4jaaMb4WCo
New ASA & SPA alert: ND4 gene mutation linked to severe neuro complications after anesthesia in patients of Venezuelan ancestry. Guidance urges avoiding volatile agents & genetic screening. https://t.co/mkKYzfoe8B #Anesthesia#Genetics#PatientSafety#ND4mutation
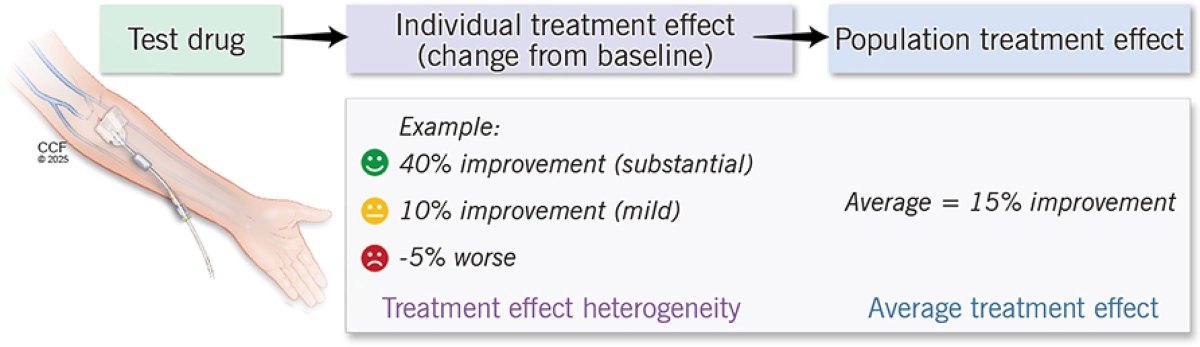
Can #AI identify who actually benefits from #steroids?
These investigators uncovered distinct #cardiac#surgery phenotypes with different responses to perioperative steroids. Are we getting closer to precision medicine in the OR?? 🤖💉
#ArtificialIntelligence#PrecisionMedicine #CardiacAnesthesia #PerioperativeMedicine #MachineLearning #anesthesia
https://t.co/1SS4YT6zBi
Perioperative Inflammation and Immune Response in Anesthesia
This JCVA review synthesizes 54 studies on how propofol, volatiles, opioids, and regional anesthesia differentially regulate cytokines, infection risk, and organ outcomes. https://t.co/aksudVu7iy
🧠💥Extubación después de una lesión cerebral aguda: ¡¡un dilema sin resolver!!🔎📚📜
La decisión de extubar a un paciente en cuidados neurocríticos se basa en 3️⃣ condiciones básicas:
1️⃣ Los predictores generales en la UCI incluyen la estabilidad hemodinámica y respiratoria, junto con un resultado positivo en la prueba de aliento espontáneo.
2️⃣ Estado neurológico🧠 según ventilación espontánea de soporte: lesión cerebral en proceso de resolución, no hay cirugía planificada, considerando la trayectoria de la condición neurológica y el nivel de conciencia sin establecer un umbral mínimo de puntuación de Glasgow.
3️⃣ Permeabilidad de la vía área, capacidad de manejar secreciones ambas evaluadas con la puntuación de Coplin o escalas similares.
👇🏽👇🏽👇🏽👇🏽
https://t.co/x9lyGLcSo7
🔓🗝
https://t.co/ba0rsRHrrL
A principios de los años 90, poco antes de morir, Bukowski pronosticó un mundo de incomunicación y tecnología. Han pasado casi treinta años y su poema se ha convertido en profecía cumplida. El fragmento pertenece al poema "Esta bandera no ondea con cariño".
Today's Paper of the Day is:
Nuts and bolts of lung ultrasound: utility, scanning techniques, protocols, and findings in common pathologies
https://t.co/JKgcYjlUQ5
Join us to read 1 paper per day and stay up-to-date as we cover the spectrum of critical care across 2026
🍽️ ICU nutrition: we’ve been doing it wrong for years?
More calories
More protein
Earlier feeding
Sounds logical
But physiology disagrees
⚠️ The key update
High-quality RCTs now show:
❌ Early full-dose nutrition
→ NO benefit
→ Potential harm
Especially in:
• Shock
• Multiorgan failure
• High metabolic stress
👉 This is not neutral
👉 This is dangerous practice
🧠 Critical illness is not static
It evolves through metabolic phases:
1. Acute catabolic phase
2. Stabilization phase
3. Recovery phase
👉 Feeding must follow physiology
Not protocols
🔥 Phase 1: Acute catabolic
• High inflammation
• Insulin resistance
• Endogenous substrate mobilization
👉 The body is NOT ready for full nutrition
💡 Strategy:
✔️ Permissive underfeeding
✔️ Low protein
Why?
Because early overload leads to:
• Hyperglycemia
• Hepatic dysfunction
• Renal stress
• Impaired autophagy
👉 You are feeding dysfunction, not recovery
⚖️ Phase 2: Stabilization
• Inflammation decreasing
• Organ function improving
👉 Now metabolism starts to tolerate nutrition
💡 Strategy:
✔️ Slow escalation
✔️ Daily reassessment
⚠️ Red flags:
• Hypophosphatemia
• Hyperglycemia
→ Patient is NOT ready
💪 Phase 3: Recovery
• Anabolism returns
• Mobility improves
👉 NOW nutrition matters most
💡 Strategy:
✔️ Higher calories
✔️ Higher protein
✔️ Combine with rehab
👉 This is where you rebuild muscle and function
📊 The real takeaway
Nutrition is NOT:
❌ A fixed prescription
❌ A calorie target
It is:
✔️ A dynamic therapy
✔️ A metabolic intervention
🎯 The new principle
“Start low
Advance judiciously
Individualize throughout”
👉 Precision ICU nutrition
⚠️ Final thought
Overfeeding early harms
Underfeeding late harms
👉 Timing is everything
📚 Stoppe C et al. Curr Opin Clin Nutr Metab Care 2026
DOI: 10.1097/MCO.0000000000001186
🫁 Lung Ultrasound 2.0, From Art to Science
The new international consensus on lung ultrasound marks a clear transition:
👉 From qualitative interpretation
➡️ To standardized, reproducible, and quantitative medicine
⚠️ What is truly NEW in this update
🔴 1. Standardization is now mandatory, not optional
LUS is highly operator- and machine-dependent
👉 The same patient can generate different findings depending on settings
New recommendation:
• Always report probe, frequency, MI, depth, protocol
• Move toward reproducible imaging frameworks
🧠 2. B-lines are no longer “simple artifacts”
They are:
• Frequency-dependent
• Physically complex
• Linked to lung microstructure
👉 Counting B-lines is semi-quantitative at best
➡️ Future: quantitative ultrasound spectroscopy
🤖 3. AI enters LUS, but with caution
AI is emerging in:
• Image segmentation
• Severity scoring
• Pattern recognition
BUT:
👉 Strong warning against overinterpretation and poor methodology
Key requirement:
• Proper dataset splitting
• Standardized acquisition
• Clinical validation
⚙️ 4. Multidisciplinary shift
This is not just a clinical update
👉 Engineers + physicists are now part of the consensus
Why?
• Ultrasound physics matters
• Signal processing matters
• Image formation matters
➡️ LUS is now a true bioengineering field
📊 5. From subjective to objective metrics
Major gap identified:
• Pleural line abnormalities
• Subpleural consolidations
• Artifact interpretation
👉 Need for:
• Measurable parameters (mm, not “small/large”)
• Quantitative imaging endpoints
🛑 6. Safety is finally addressed
New concern:
👉 Potential pulmonary capillary hemorrhage (animal data)
Recommendation:
• Apply ALARA principle
• Monitor Mechanical Index (MI)
• Limit exposure time
➡️ LUS is safe, but not risk-free
📚 7. Education becomes a core pillar
Clear statement:
👉 LUS must be formally taught and standardized
Including:
• Medical curriculum integration
• Structured training
• Remote mentoring
🎯 Take-home message
Lung ultrasound is evolving from:
❌ Operator-dependent bedside tool
✅ Standardized, physics-driven, AI-supported diagnostic modality
⚖️ My reflection
We are entering a phase where:
👉 Understanding how ultrasound interacts with lung tissue
is as important as interpreting the image itself
This is where critical care, cardiology, and engineering finally meet
📖 Libertario D et al J Ultrasound Med 2023
doi:10.1002/jum.16088
#LungUltrasound #CriticalCare #POCUS #MedicalAI #ICU #Ultrasound #PrecisionMedicine #ACVC
#DocenciaSEDAR📚 Artículo de revisión
Rotura uterina intraparto, manejo anestésico y resultados materno-fetales. Un artículo fundamental para prevenir no una catástrofe sino dos.
Lectura imprescindible para práctica clínica.
🔗 https://t.co/VgmKyQO6tu
#CardioToVascSEDAR 🫀📊 Revisión 2026: Anestesia en cardiopatías congénitas:
Cuatro ejes principales: ERAS, manejo de CEC, seguridad perioperatoria, adultos con patología compleja
Impacto directo en outcomes y organización de equipos.
🔗https://t.co/rsHTwc75v5
This excellent new #BJAEd Article by Kovac & Choksi on the prophyalxis and treatment of Postoperative Nausea and Vomiting, is available to read now: https://t.co/7VwFazUJj7
La mente que rumia se enfrasca en un bucle de #pensamientos negativos. Pero, aunque parezca complicado, la psicología demuestra que es posible escapar de la espiral.
https://t.co/z7ENYalFVh
Depression affects approximately a quarter of a billion people globally, of all ages and from all walks of life.
A new Seminar provides a comprehensive overview of the epidemiology, diagnosis, & management of depression in adults: https://t.co/f8qW9C7RLt
More about VAC in sepsis... 🤓
🫀 Why do some septic shock patients respond to treatment… and others don’t?
We often blame:
• “Refractory shock”
• “Severe sepsis”
• “Late presentation”
But physiology tells a different story.
⚙️ The real problem: ventriculo-arterial decoupling
Septic shock is not only vasodilation or myocardial depression.
👉 It is a failure of interaction between the heart and the arterial system
This interaction is called:
➡️ Ventriculo-arterial coupling (VAC)
And it defines:
✔️ Cardiac output
✔️ Arterial pressure
✔️ Perfusion efficiency
🧠 What can be often ignored in daily ICU practice
You can have:
✔️ Normal cardiac output
✔️ Acceptable MAP
❗ And still have inefficient circulation
Because:
👉 Energy transfer from the ventricle to the arterial system is impaired
📉 What happens in septic shock?
• Decoupling is common
• LV ejection becomes inefficient
• Cardiovascular treatments become less effective
💉 Clinical paradox
Same intervention. Different outcomes.
Example with norepinephrine:
🔵 Patient A
→ Adequate contractility (Ees preserved)
→ ↑ arterial tone
→ VAC improves
→ ↑ CO
🔴 Patient B
→ Depressed contractility
→ ↑ arterial tone (afterload)
→ VAC worsens
→ ↓ stroke volume
🔥 This explains a lot of what we see
• Why MAP increases but CO drops
• Why some patients “fail” vasopressors
• Why fluids work in some and not others
• Why lactate persists despite “normal numbers”
🧬 Even more important
VAC is:
👉 A determinant of treatment responsiveness, not just a descriptor of physiology
📊 Bedside implication
We should stop asking only:
❌ “What is the MAP?”
And start asking:
✅ “Is the system coupled?”
✅ “Are we improving efficiency or just pressure?”
⚡ Practical shift
Instead of protocol-only resuscitation:
➡️ Move toward physiology-guided resuscitation
Using:
• Ea (arterial load)
• Ees (contractility)
• VAC (their interaction)
🧠 Final thought
Septic shock is not just:
❌ A pressure problem
❌ A volume problem
👉 It is an interaction problem
And until we treat it as such:
➡️ Some patients will continue to “not respond”
📚 Pinsky MR, Guarracino F. (2023)
Intensive Care Medicine Experimental
https://t.co/3bYkZ1G7wG