The CANTOS trial made a striking point a few years ago: target inflammation directly, and cardiovascular events drop, independent of cholesterol or blood pressure. Inflammation isn't just a bystander in chronic disease. It's a driver.
That's the lens worth applying to tirzepatide.
Published research suggests CRP falls 20-40% over 12-18 months, with IL-66 and TNF alpha following the same pattern. Part of that is visceral fat loss, the body's largest source of inflammatory cytokines and part of it appears to be a direct effect of GLP-1 receptor activation on immune cells.
Why it matters: the same inflammation reduction plausibly feeds into the cardiovascular, kidney, liver, and metabolic benefits people already associate with the medication. Viewed that way, inflammation is the thread connecting them.
The honest caveat: it's not an FDA-approved inflammation indication, and the long-term outcome trials are still maturing. But it may be the most underdiscussed part of the tirzepatide story.
10 reasons, broken down:
https://t.co/09NpXvR1aB
Everyone asks about tirzepatide and cholesterol, and the conversation almost always starts with LDL.
LDL is the number tracked in primary care and the one statins target. But it's also where the tirzepatide story gets undersold.
The LDL drop is real but modest: 5-12% on average. A moderate statin does 30-40%. So if you need meaningful LDL lowering, tirzepatide isn't a substitute, it's an add-on.
The bigger story is in your triglycerides, where the drop runs 15-30%. That's more than fibrates, niacin, or omega-3s typically deliver. And it matters, because elevated triglycerides are the lipid signature of insulin resistance, one of the strongest single predictors of cardiometabolic risk in exactly the population most likely to be on this medication.
Why the larger effect? The mechanism sits further upstream. As insulin sensitivity improves, the liver produces less VLDL, the carrier particle for triglycerides. Fibrates work downstream of that, which is part of why the effect here tends to be bigger and more durable.
The rest of the panel moves in the right direction too: HDL up 3–8%, ApoB down 8–15% (often a better risk marker than LDL alone), and LDL particles trending larger and less dense. Lp(a) doesn't budge but almost nothing moves Lp(a).
The real takeaway: it's not any single number, it's the whole profile shifting away from atherogenic dyslipidemia. Give it time, first changes show around 8-12 weeks, but the 12 month panel is what reflects the full effect.
If you've only been watching your LDL, you've been watching the smallest part of the story.
Only a small proportion of men prescribed testosterone therapy received recommended diagnostic testing for androgen deficiency, and many received testosterone therapy despite contraindications, a single-center study showed.
“Testosterone prescriptions have quadrupled in the last three decades in the United States, despite stable rates of hypogonadism diagnoses, a pattern consistent with overuse and potentially inappropriate prescribing,” lead author Maria Papaleontiou, MD, associate professor in the Division of Metabolism, Endocrinology and Diabetes, University of Michigan, Ann Arbor, told Medscape Medical News. https://t.co/MJpgB5RBBj
Quem nega que o excesso de exames complementares pode causar danos importantes está desinformado.
A literatura científica sobre falsos positivos, sobrediagnóstico e tratamentos desnecessários é extremamente inequívoca e robusta.
O senso comum é que continua desinformado.
Researchers at Stanford University have elucidated a mechanism behind the occurrence of myocarditis following mRNA COVID-19 vaccination, particularly in young males.
Analysis of blood samples from vaccinated individuals revealed elevated levels of two cytokines—CXCL10 and interferon-gamma (IFN-γ)—in those who developed post-vaccination myocarditis.
These signaling proteins initiate a two-step inflammatory cascade: CXCL10, primarily produced by macrophages in response to the vaccine, recruits T cells that release IFN-γ, which in turn attracts aggressive immune cells (such as neutrophils and macrophages) to the heart, leading to tissue damage.
In preclinical models (including mice and human cardiac tissue), neutralizing CXCL10 and IFN-γ significantly reduced cardiac injury and immune cell infiltration without impairing the vaccine's overall immunogenicity.
Additionally, pretreatment with genistein—a soy-derived anti-inflammatory compound—attenuated the cytokine surge and mitigated heart damage in these models.
Vaccine-associated myocarditis typically presents with symptoms like chest pain, shortness of breath, and palpitations shortly after the second dose and remains exceedingly rare.
Importantly, SARS-CoV-2 infection itself poses a substantially higher risk of myocarditis—along with severe multisystem complications—reinforcing that the benefits of mRNA vaccination far exceed the risks.
Statistics report 1 case of myocarditis in 9,000–25,000 doses for the highest-risk groups, adolescent and young adult males, particularly after the second dose. Rates were much lower in females, older adults, and after first or booster doses. For context, myocarditis risk from actual COVID-19 infection was substantially higher—often 10 times or more in comparable age groups.
[Cao, X., Manhas, A., Chen, Y.-I., et al. (2025). Inhibition of CXCL10 and IFN-γ ameliorates myocarditis in preclinical models of SARS-CoV-2 mRNA vaccination. Science Translational Medicine. DOI: 10.1126/scitranslmed.adq0143]
It's intoxicating to think that whole body scans for the entire world's population will be life saving.
What I'm going to tell you is counterintuitive. You don't want it to be true.... THIS WILL CAUSE NET HARM
You don't want it to be true. I get it. I don't want it to be true either. But it is fixed probability theory (Bayes Theorem), not a difference of opinion. It's not something where you can be "in one camp" or "in another camp." It's not philosophy. It's math.
Applying a full-body scan to an asymptomatic population is like waving a metal detector over a beach covered in bottle caps and saying, "I'm not in the camp that worries about bottle caps, we'll just shovel the entire beach into a lab and sort it out later."
You're looking for a ring... but in this case all the bottle caps look like rings.
The problem isn't the sensitivity of your detector; I don't care if it's the best most advanced detector ever made. it's the mathematical certainty that the junk drastically outnumbers the treasure.
When pretest probability is near zero, Bayes' theorem dictates that the Positive Predictive Value crashes to near zero. Even if a future machine achieves a hypothetical 99% specificity, testing for a disease with a 0.01% prevalence means a 1% PPV. For every 1 true cancer you catch, you get 100 false positives.
Because a full-body scan acts as dozens of independent tests, a standard 95% specificity per organ system mathematically guarantees a false positive rate over 60% per patient. You cannot "catalog and learn" your way out of that reality without subjecting millions of healthy people to real-world harm first.
We've seen this movie before. It isn't different now just "because AI" or because "we will have more and better data" or "we'll learn" our way out of it.
Math doesn't have philosophical camps. It's just... well, boring math.
Spot on.
Its the core issue with “Longevity Clinics” right now.
Full body “screening” MRI = net harm. cCTA in asymp to “detect soft plaque” = net harm
Fortunately (unfortunately), “Longevity” / Prevention.. is “boring”.. exercise/bmi/nutrition/sleep/stress/bp/glucose/apob..
everything else = low value, and potentially harmful
@PeterDiamandis@altcap@CanesDavid@drjohnm
Sim.
Se, por acaso, decidíssemos fazer ressonância de corpo inteiro em toda a população, a saúde populacional provavelmente pioraria, e não melhoraria.
🚨 BREAKING: COVID vaccine linked to broader heart protection in new study researchers report nearly 40% lower risk of COVID-related cardiovascular events, including heart attack and stroke
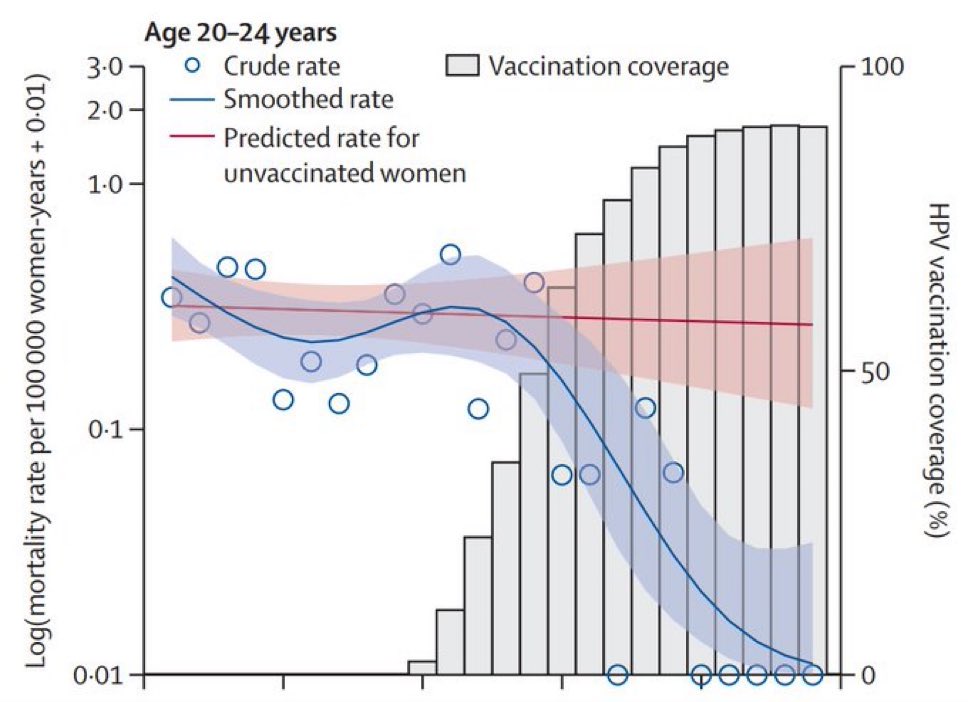
In a time such conflict & uncertainty, we need to hold on to every bit of good news - & this is truly magnificent story. Thanks to the wonders of medical vaccination, women who receive an HPV vaccine in early adolescence now have virtually zero risk of dying from cervical cancer before the age of 30. A safe, simple jab has almost eradicated one of the cruellest cancers women ever experience.
Cervical cancer is the fourth most common cancer in women (about 3300 new cases are diagnosed in England every year) & human papillomaviruses (HPV) cause 99% of cases. We already knew that the HPV vaccine prevented about 90% of cervical cancers, but this new study used official cancer mortality & vaccination data to assess the vaccine’s impact on survival. That impact is so great that the authors estimate the likelihood of girls who are vaccinated at age 12 or 13 dying from cervical cancer before the age of 30 is almost zero.
But there’s a sting in the tail.
Vaccine hesitancy means take up of the vaccine is falling. Only 75% of girls who could receive the vaccine are doing so, no doubt in part because of the tsunami of anti-vaxx disinformation & scaremongering out there online. Some of these girls are destined, one day, to develop an avoidable cervical cancer that will claim their life, and that is a tragedy.
Please know the safety data for the HPV vaccine is robust and clear - it’s incredibly safe and it could save a teenager's life. The NHS has excellent info on vaccines - please read up on vaccines from reliable sources. Or talk to a doctor - we want to help & are only too happy to discuss your concerns. Thank you.
💉 The HPV vaccine for cervical cancer has reduced the risk of dying from the disease before the age of 30 in England to almost zero, the first study of its kind showed Thursday.
➡️ https://t.co/42YN9gPjqy
Among US adults, 2024–2025 COVID-19 vaccination was associated with a 26% lower risk of COVID-19 ED/UC visits, 35% lower risk of hospitalization, and 41% lower risk of critical illness, with effectiveness declining >6 months post vaccination. https://t.co/IizOkQde2N
Among US veterans, the 2024-2025 COVID-19 vaccine was associated with a 37.7% lower risk of COVID-19–associated #MACE, with the largest benefit in adults >75 years and those with comorbidities. https://t.co/2vMsEX2uY3
A major new study involving more than 1.03 million U.S. veterans has found that receiving the updated 2024-2025 COVID-19 vaccine was associated with significantly lower rates of serious heart-related complications and death.
Researchers observed a 37.7 percent reduction in the risk of major adverse cardiovascular events directly linked to COVID-19, including heart attacks, strokes, heart failure hospitalizations, and cardiovascular deaths.
The protective effects extended beyond COVID-associated outcomes. Vaccinated individuals also showed a modest but meaningful decrease in overall major cardiovascular problems, even when not tied to a confirmed infection. The study reported an approximate 6 percent lower risk of broad cardiovascular disease events and a 7 percent reduction in all-cause hospitalizations and deaths during the eight-month follow-up period.
These seemingly modest relative reductions translate into substantial public health benefits at the population level. For every 10,000 vaccinated individuals, researchers estimated the prevention of about 23 major cardiovascular events, 30 hospitalizations, and 16 deaths over eight months. Scaled to one million people, this could mean thousands of avoided heart attacks, strokes, hospitalizations, and fatalities.
The greatest benefits appeared among adults aged 75 and older and those with pre-existing conditions such as cardiovascular disease, diabetes, or chronic lung disease. Scientists attribute much of this protection to the vaccine’s ability to prevent SARS-CoV-2 infection and the virus’s known damaging effects on the cardiovascular system, including inflammation, blood vessel injury, and increased clotting.
Notably, vaccinated veterans experienced fewer cardiovascular issues even in the absence of documented COVID-19, possibly reflecting protection against mild or undetected infections. While further research is needed to clarify this mechanism, the findings strengthen the evidence that COVID-19 vaccination offers broad cardioprotective benefits beyond the prevention of acute respiratory illness.
[Cai M, et al. (2026). 2024-2025 COVID-19 Vaccine and Major Adverse Cardiovascular Events Among US Veterans. JAMA Internal Medicine. DOI: 10.1001/jamainternmed.2026.1929]
New research adds to a growing body of evidence suggesting that shingles vaccination may reduce the risk for dementia.
Published in Annals of Internal Medicine, the research found Medicare beneficiaries who received the recombinant zoster vaccine had a 24% lower relative risk for dementia than their unvaccinated peers. While experts remain divided on whether the brain-protecting benefit stems from a biological reaction or simply from preventing virus-induced neuroinflammation, some frontline clinicians are already leveraging the findings as a selling point to counter vaccine hesitancy. https://t.co/hqkgMlOD80




















![Rainmaker1973's tweet photo. Researchers at Stanford University have elucidated a mechanism behind the occurrence of myocarditis following mRNA COVID-19 vaccination, particularly in young males.
Analysis of blood samples from vaccinated individuals revealed elevated levels of two cytokines—CXCL10 and interferon-gamma (IFN-γ)—in those who developed post-vaccination myocarditis.
These signaling proteins initiate a two-step inflammatory cascade: CXCL10, primarily produced by macrophages in response to the vaccine, recruits T cells that release IFN-γ, which in turn attracts aggressive immune cells (such as neutrophils and macrophages) to the heart, leading to tissue damage.
In preclinical models (including mice and human cardiac tissue), neutralizing CXCL10 and IFN-γ significantly reduced cardiac injury and immune cell infiltration without impairing the vaccine's overall immunogenicity.
Additionally, pretreatment with genistein—a soy-derived anti-inflammatory compound—attenuated the cytokine surge and mitigated heart damage in these models.
Vaccine-associated myocarditis typically presents with symptoms like chest pain, shortness of breath, and palpitations shortly after the second dose and remains exceedingly rare.
Importantly, SARS-CoV-2 infection itself poses a substantially higher risk of myocarditis—along with severe multisystem complications—reinforcing that the benefits of mRNA vaccination far exceed the risks.
Statistics report 1 case of myocarditis in 9,000–25,000 doses for the highest-risk groups, adolescent and young adult males, particularly after the second dose. Rates were much lower in females, older adults, and after first or booster doses. For context, myocarditis risk from actual COVID-19 infection was substantially higher—often 10 times or more in comparable age groups.
[Cao, X., Manhas, A., Chen, Y.-I., et al. (2025). Inhibition of CXCL10 and IFN-γ ameliorates myocarditis in preclinical models of SARS-CoV-2 mRNA vaccination. Science Translational Medicine. DOI: 10.1126/scitranslmed.adq0143]](https://pbs.twimg.com/media/HK_7ANSXUAAzckG.jpg)





![Rainmaker1973's tweet photo. A major new study involving more than 1.03 million U.S. veterans has found that receiving the updated 2024-2025 COVID-19 vaccine was associated with significantly lower rates of serious heart-related complications and death.
Researchers observed a 37.7 percent reduction in the risk of major adverse cardiovascular events directly linked to COVID-19, including heart attacks, strokes, heart failure hospitalizations, and cardiovascular deaths.
The protective effects extended beyond COVID-associated outcomes. Vaccinated individuals also showed a modest but meaningful decrease in overall major cardiovascular problems, even when not tied to a confirmed infection. The study reported an approximate 6 percent lower risk of broad cardiovascular disease events and a 7 percent reduction in all-cause hospitalizations and deaths during the eight-month follow-up period.
These seemingly modest relative reductions translate into substantial public health benefits at the population level. For every 10,000 vaccinated individuals, researchers estimated the prevention of about 23 major cardiovascular events, 30 hospitalizations, and 16 deaths over eight months. Scaled to one million people, this could mean thousands of avoided heart attacks, strokes, hospitalizations, and fatalities.
The greatest benefits appeared among adults aged 75 and older and those with pre-existing conditions such as cardiovascular disease, diabetes, or chronic lung disease. Scientists attribute much of this protection to the vaccine’s ability to prevent SARS-CoV-2 infection and the virus’s known damaging effects on the cardiovascular system, including inflammation, blood vessel injury, and increased clotting.
Notably, vaccinated veterans experienced fewer cardiovascular issues even in the absence of documented COVID-19, possibly reflecting protection against mild or undetected infections. While further research is needed to clarify this mechanism, the findings strengthen the evidence that COVID-19 vaccination offers broad cardioprotective benefits beyond the prevention of acute respiratory illness.
[Cai M, et al. (2026). 2024-2025 COVID-19 Vaccine and Major Adverse Cardiovascular Events Among US Veterans. JAMA Internal Medicine. DOI: 10.1001/jamainternmed.2026.1929]](https://pbs.twimg.com/media/HLF9xqtW0AAA0L_.jpg)































