Rheumatologist at Institute for Rheumatic and Autoimmune Disease at Overlook Hospital, proud Hopkins alum, health care advocate, Eagles fan entering Giants land
Aggarwal #RNL26@RheumNow
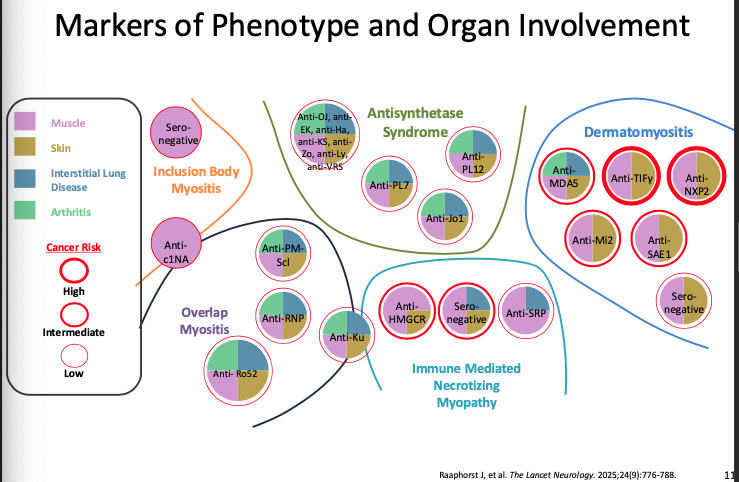
Most common antibody in myositis? ANA
2/3 pts have myositis-specific antibody (MSA), 1/3 sero-neg
Each MSA highly specific (95%), not sensitive. Overall Myositis Panel 70% sens
Can help phenotype of disease, cancer risk/screening
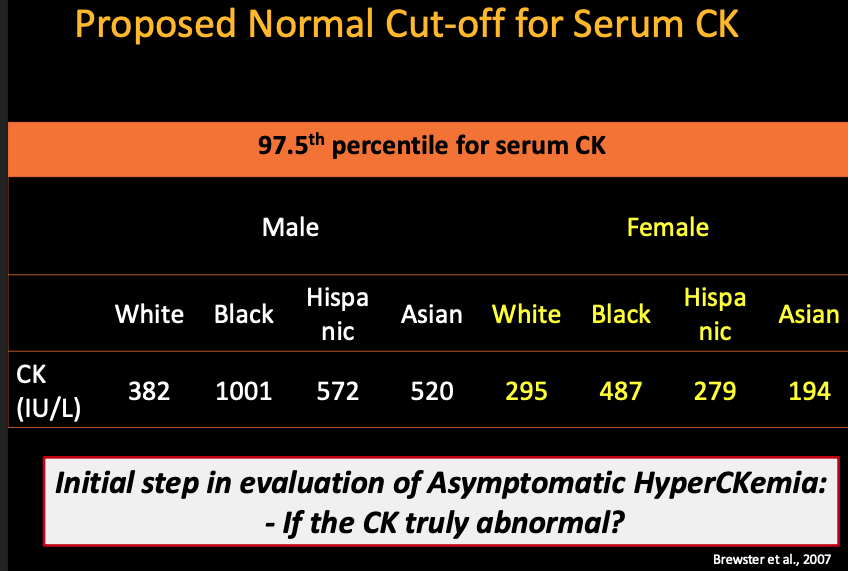
High CK:
Truly abnormal?
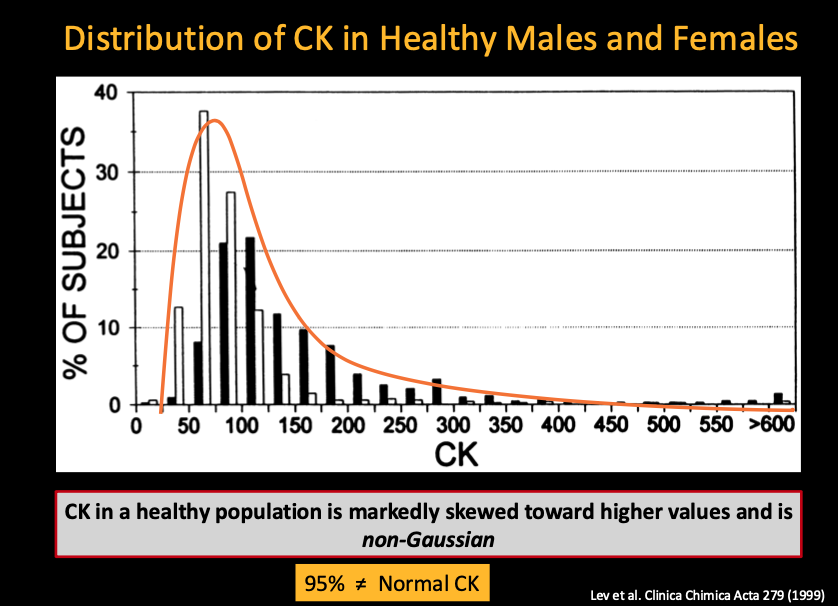
Non-Gaussian distribution - should not use 95% cut-off
97.5% cut-off preferred by gender, race, & ethnicity
From exercise?
Exercise can increase by 10-30x. Avoid exercise for 1 week & repeat
Non-neuromusc causes: Endocrine, meds, MacroCK
@RheumNow#RNL26
Other options in AxSpA
Filgotinib: not approved in US due to male repro concerns
Brodalumab: warning for suicidality
Izokipep: fusion protein, nanobody, similar efficacy to IL-17Ai, may be lower cost
Sonelokimab, another IL-17A nanobody
TYK2 - Deucr, zasocitinib
@RheumNow#ACR26
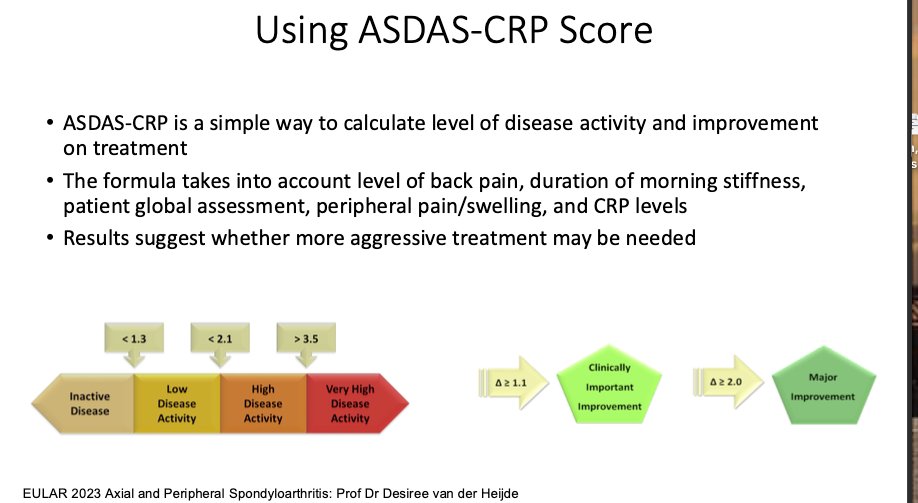
ADAS-CRP Score
Formula looking at back pain, duration of morning stiffness, pt global assessment, peripheral jts, and CRP
Low or high disease activity - no moderate range to encourage getting to disease control
TICOSPA did not show clear T2T benefit
#RNL26@RheumNow
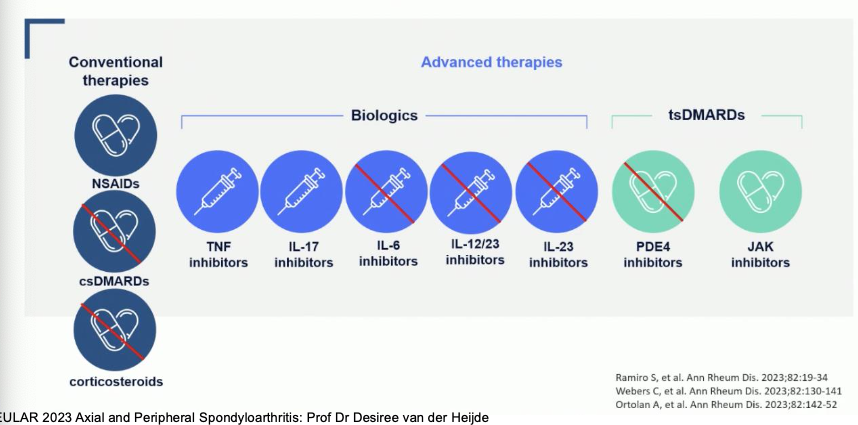
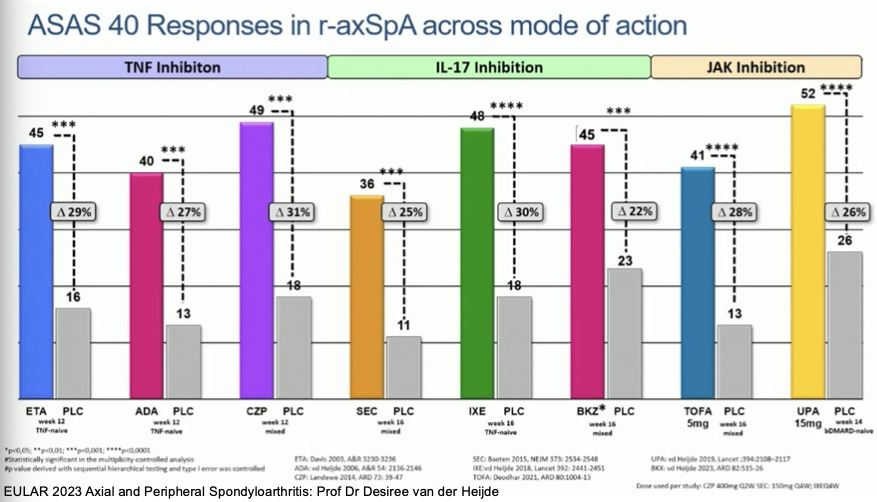
Blakewell: There is not one agent that is superior between TNF, IL-17, JAKi
Patient characteristics and manifestations can help make decision
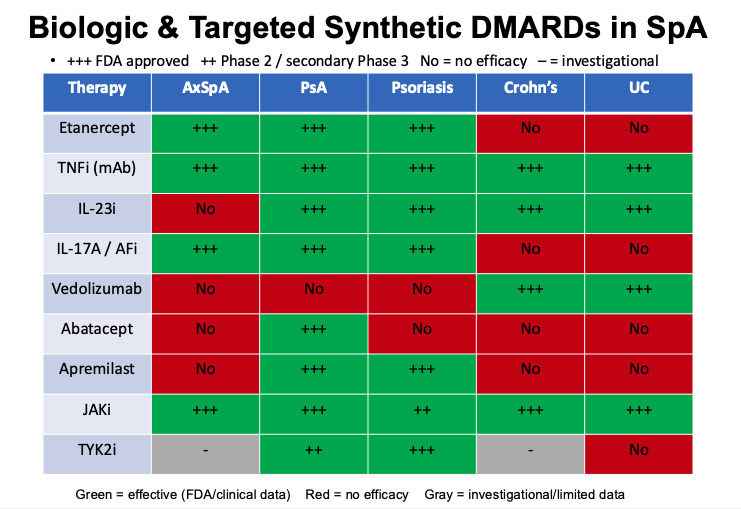
Some meds clearly shown to be not helpful
@RheumNow#RNL26
Advances in SpA
#RNL26@RheumNow
Uveitis: Adalimumab, bimekizumab, and upadacitinib reduce uveitis flares in SpA
Ada and MTX have data for efficacy in non-infectious posterior uveitis (NIPPU)
Brepocitinib study ongoing for NIPPU
Knee involvement in AxSpA
#RNL26@RheumNow
15-50% of pts
Adults <50yr - 2.7x higher risk of AxSpA
Risks of large jt involvement:
Early age of AxSpA
RIsk for THA - male
Risk for TKA - obesity & smoking, h/o THA
Decreased risk with b/csDMARD
Complications of SpA
#RNL26@RheumNow
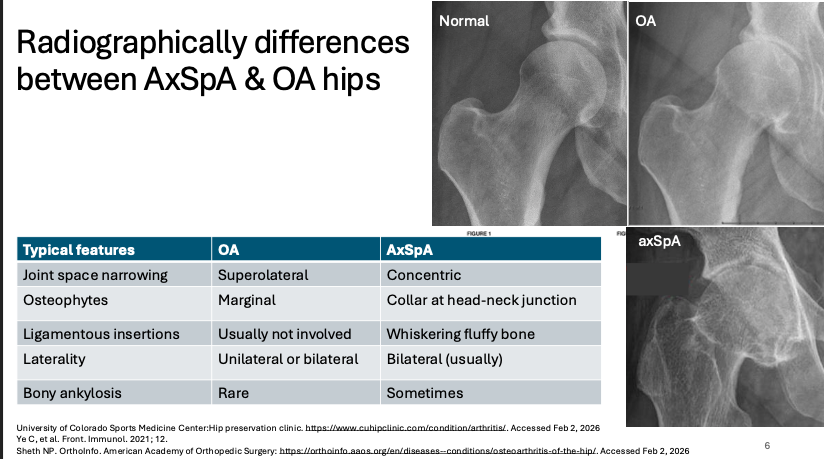
Hip involvement common in AxSpA - 10-60%, up to 40% of pts with minimal symptoms
THA risk: 3-4x higher in r-axSpA
Xr-ay: concentric jt space narrowing (not superolateral), collar of osteophytes at head-neck junction (not marginal osteophytes)
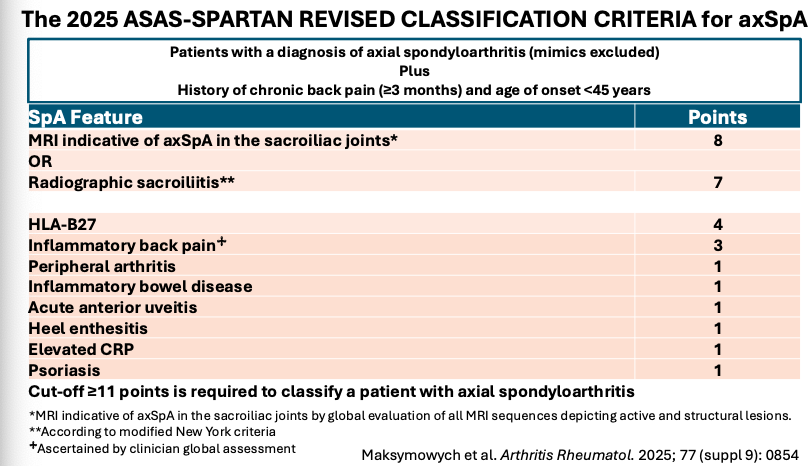
Update of 2025 ASAS-SPARTAN Revised Classification Criteria for AxSpA
@RheumNow#RNL26
Notes must exclude mimics
MRI findings involve active & structural lesions, not just bone marrow edema
Difficult to meet clinically without any imaging criteria (xray or MRI)
Pub pending
AxSpA Imaging
@RheumNow#RNL26
Xray SI jt - 1st line in most pts, but young pts short duration can consider MRI as 1st-line
Challenge in imaging:
SI jt edema in athletes/postpartum Mimics like osteitis condensans ilii - diff by anterior localization, absence of erosions
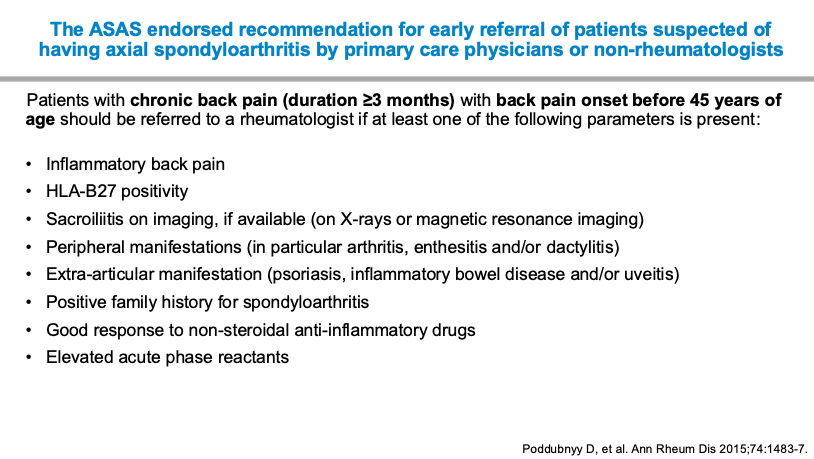
Poddubnyy at #RNL26@RheumNow:
"Treating spondyloarthritis is easy, the challenge is when the diagnosis is not correct"
PROCLAIR Study: mean diagnostic delay 5.7 yrs
Prevalence of axSpA in pts w chronic back ~5%
ASAS endorses early referral recommendations for higher risk pts
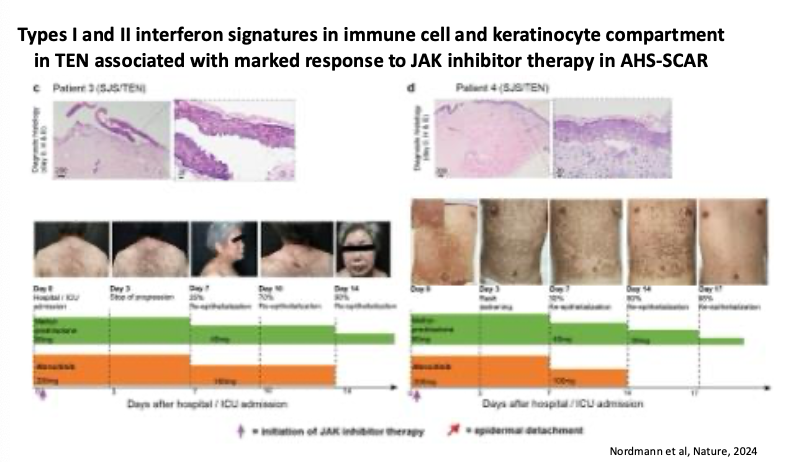
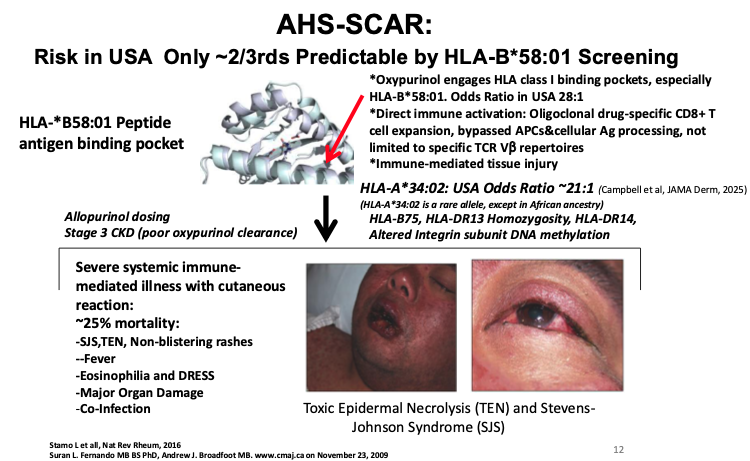
Can you predict Allopurinol Hypersensitivity (AHS-SCAR) with HLA screening?
#RNL26@RheumNow
Not completely - only 2/3 predictable by HLA-B*58:01 screening
Others like HLA-A*34:02 also associated, but unable to commercially test for
Treatment: Marked response to JAK inhibitor Rx
Terkeltaub on improving gout in real world
#RNL26@RheumNow
-Earlier switch to 2nd line febux
-More T2T ULT gout clinic
-Broader colchicine PPx
-Better co-manage links to metab, CVD, renal dis
-Phamacogenomics (eg HLA-B58:01)
-ULT, drug pipeline
TRUST: primary care T2T ULT trial
Where is gout in the real world?
@RheumNow#RNL26
-Healthcare disparities
-Failure of T2T
-Poor urate control worsens CVD, mortality
-Recent gout flare, gout dx, ULT initiation markedly increase CVD events
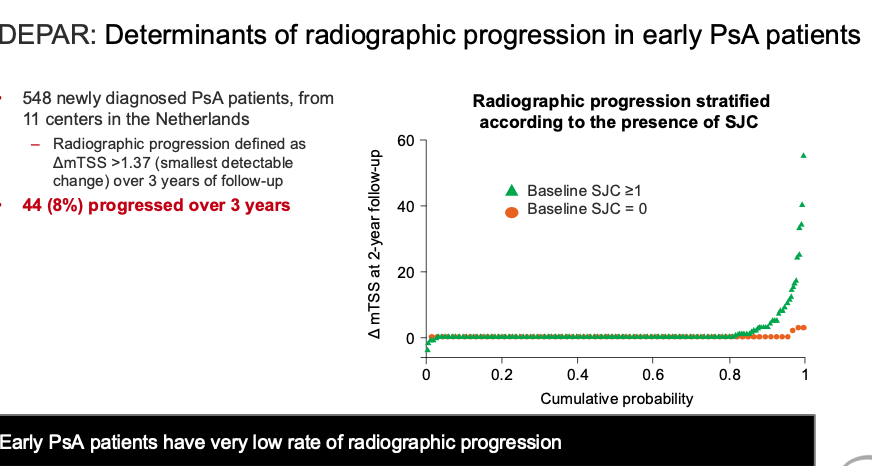
DEPAR study:
Early PsA patients have low rate of radiographic progression, esp if dx is controlled
Kavanaugh: Are Xrays needed in PsA?
- Changes minimal in PsA, only in few pt, seen w active synovit
- Short trials won't see diff
-Newer imaging modalities better
@RheumNow#RNL26
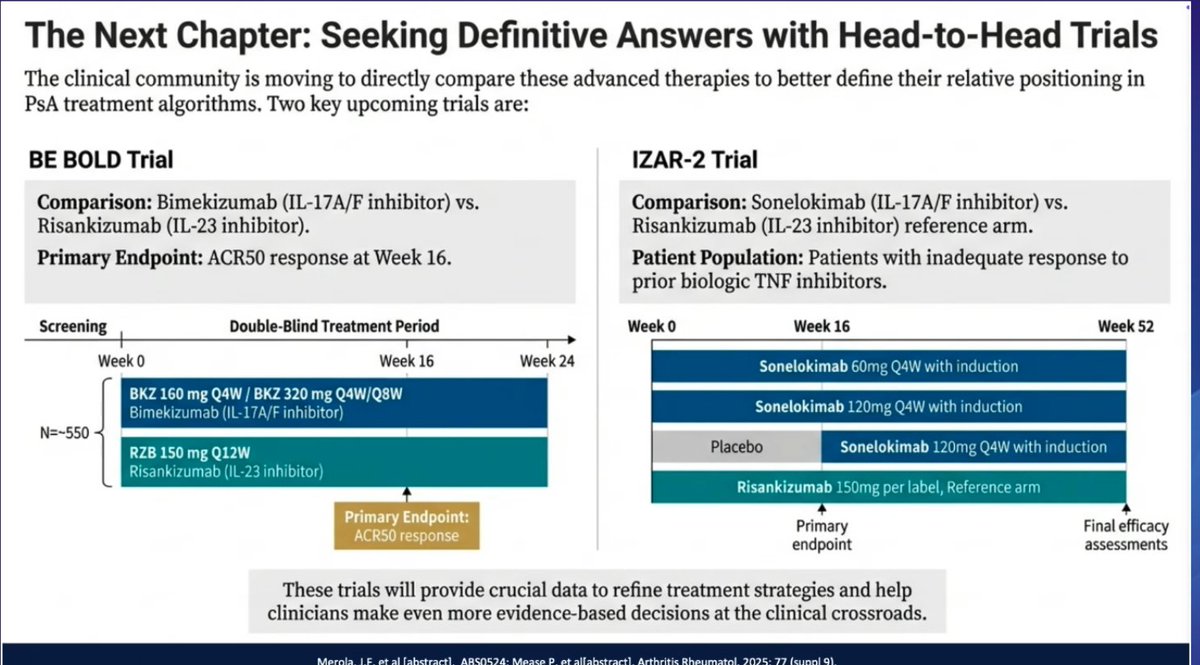
Upcoming H2H studies in PsA
2 studies of IL-17A/F vs IL-23
BE-BOLD: Bimekizumab v Risankizumab
IZAR-2: Sonelokimab v Risankizumab in TNF failure
Will provide useful info in differentiating new IL17 mechanism v IL23
#RNL26@RheumNow
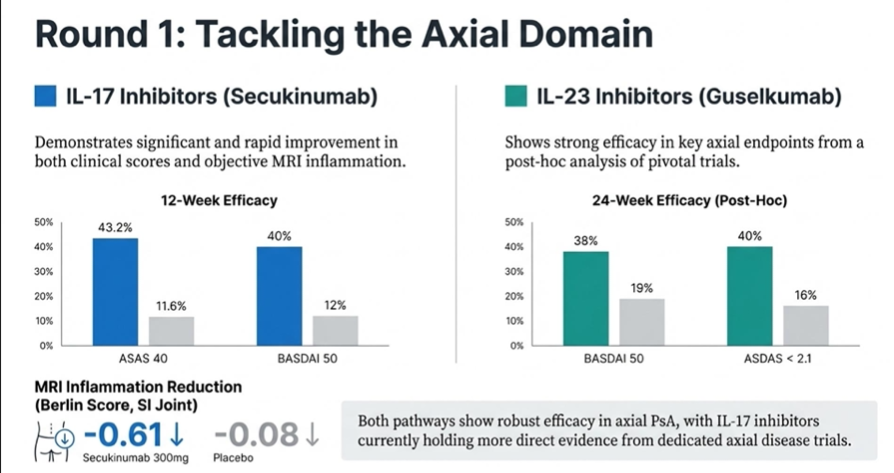
IL-17 v IL-23
#RNL26@RheumNow
Axial domain- good IL-17 data as well IL-23 post-hoc data
Both show data of prevention of damage
Real-world data suggest IL-23 longer persistence
Safety: higher candidiasis and IBD risks w IL17