“We found evidence of SARS-CoV-2 infected cells both in the gut and female reproductive tract… more than 4 years after the initial infection,” said Dr. Marta Mirabent, who is part of the Roan lab team investigating SCV2 persistence in these sites as driver of Long Covid. Their initial findings suggested SCV2 RNA and proteins can persist in the endometrium, endo-cervix and ecto-cervix; with more patient biopsies currently underway.
Hmmmm.....
Seems like the #Leonardi_Effect is finally making its way into the mainstream media, @fitterhappierAJ
Probs a little late 🙄
Better late than never
Reports from Cuba describe a mysterious multi-symptom epidemic (fever, rash, vomiting, diarrhea, joint pain) infecting as much as one-third of the population, overwhelming hospitals, and prompting travel advisories.
Local authorities are accused of under-reporting deaths amid crisis.
If you're new to these updates, check out our website for more statistics and methodologic details (https://t.co/xmDnq5NN8N).
I run the Population Science program at the Tulane Cancer Center (people with cancer are the largest group as high risk of COVlD). We have provided weekly updates the past 2.5 years and will continue to do so long-term.
The left-side tables below are useful if you'd like to get a sense of what's happening elsewhere around the country. I'll put out a Midwest regional update soon too, as it's also quite bad there. 🙏
https://t.co/SC7napc246
The Price of Denial: Early Warnings, Arrogant Dismissal, and the Lingering Cost of COVID's Immune Legacy
There have been a recent number of articles framing the immune harm from Covid as a new insight. While I am pleased this has entered the mainstream, I am afraid it is too gracious to the lagging scientific consensus of how covid has been wearing away at our immune responses. Especially given how when I raised this based on T cell phenotypes, I was dismissed and attacked with extreme prejudice.
Reframing Covid's immune harm as a new insight rather than a long-fought hypothesis contrary to 'immunity debt' achieves several aims:
1) It deemphasizes the role in propagating false narratives that several individuals had along with choice medical journals. For example, the BMJ extensively platformed Alasdair Munro's claims of the 'immunity debt' hypothesis. When an editor was approached with a proposal for how covid was harming immunity by individuals who had published in the BMJ before and myself, they refused to accept it.
2) It saves face for the individuals who staunchly attacked the hypothesis and dismissed it as a joke. Those people also strongly attacked me, and they would go on to claim that it is my fault such a false and ridiculous narrative of immune harm from covid even existed. These are lay people but also others.
3) it preserves a semblance of credibility for the established sources who previously denied the hypothesis and obfuscated it.
4) It shirks accountability for the duty of discernment, consideration, and equipoise that stewards of information and knowledge, like the BMJ, had to the public. They had access to the hypothesis and rationales previously and chose to trounce on it and dismiss it with extreme prejudice. To me, it highlights how many of the experts were ill-equipped to grasp early immunological changes and project them to their outcomes.
This was not just an oversight, it was an editorial choice. The author of the BMJ article, Nick Tsergas, confided that the editors wanted to avoid controversy and drama. They wanted to whitewash its history. What did I do to earn such controversy? Tell the truth before other scientists could see. By the time immune harm manifests there is much damage already done.
In the first half of 2020, I noted that SARS-CoV-2 had been shown in preprints to downregulate MHC Class I, overstimulate and kill CD8 T cells, and would likely accumulate harm with reinfections. I noted this even in mild cases and was dismissed by many figures, including Francois Balloux Marc Veldhoen, Zeynep Tufekci, and Antonio bertoletti. They did not dismiss kindly. Bertoletti, a senior professor at Duke NUS would reply under my posts calling me a clown and insulting me constantly. I was a medical student at the time and this behavior seemed inappropriate and offensive, especially considering how I was engaging him with genuine concern when I was discussing T cell death with him in the summer of 2020.
By late 2022, I was pointing out that many people, after even mild infections, appeared to have reductions in plasmacytoid dendritic cells and other immune changes without reporting symptoms that would fit the conventional definition of Long COVID. These were not dramatic claims; they were mechanistic observations grounded in emerging data. However, the implications were stark. I had numerous media appearances discussing that immune harm was occurring. This was discussed in The Tyee by Andrew Nikiforuk.
https://t.co/qwDICB5xrr
In April 2023, https://t.co/jcfALtlfsM published a piece that characterized concerns about lasting immune effects from mild infections as exaggerated. They quoted Professor Danny Altmann, who stated there was “no phenotype” resembling immunodeficiency, only “nuanced differences” that did not translate to real-world consequences. The article framed early warnings as misinformation, implying that those raising them were overstating risks. This was not neutral correction; it was authoritative closure of debate. The message was clear: mild infection left no meaningful immune scar outside severe disease or formally diagnosed Long COVID. Discussion effectively ended there for many. https://t.co/Ia0h8xW5TO
Where did factcheck find the authority to promise that no such immune harm was occurring? Did they truly seek to understand what the consequences of broad t cell activation, differentiation, and death would manifest in? The dismissal was reckless and arrogant. And now proven wrong.
The personal cost for telling the truth when people were actually concerned about covid was immediate and lasting. I was tagged in threads alongside senior immunologists who dismissed the ideas outright, accused (implicitly or explicitly) of fearmongering or misinterpreting preliminary data. These characterizations spread quickly on social media, embedding themselves in timelines and memories. People lied about me. Zeynep and Jeremy Kamil said that I had paid for my own PhD, when it was actually paid directly by the National Cancer Institute for my discovery of a linked mechanism of T cell death and differentiation. Years later, a search of my name still surfaces echoes of those accusations, unaccompanied by context or correction. Professional relationships cooled; invitations to collaborate quietly dried up. I lost a fellowship offer at the National Cancer Institute as Tom Misteli, the head of NCI research, wrote how, "I needed to learn what I can and can not say." The energy spent defending basic mechanistic possibilities was energy not spent on research or clinical work. It was isolating, and it was unnecessary.
This manifested into something remarkably shocking and completely unprecedented in scientific literature. My two greatest and most eminent antithetical-fans teamed up and published an article mocking my twitter handle, saying that mild breakthrough infections correlated with 'fit and happy' t cells. https://t.co/B5z7CGPt3W
It was shared across social media with an interpretation to mock my claim that T cells were harmed. People that mocked me cheered, like the Harvard professor Mark Davis, along with zeynep saying that it was a good rebuttal to 'looney twitter-only claims.' On Indie Sage, Christina Pagel did not disagree with the scientific content but expressed disappointment at the devolution of my interlocutors, that she was not a fan of shaming and mocking no matter how outlandish my claims were. She was wrong on both counts. Their mockery is now a testament to their ignorance and the devolution. This is not something they can retract, only deny publicly.
When it occurred I reached out to the editor and he asked me if I would like to reply about the scientific content. I wanted to, but, on advice of a friend who was mortified at the conduct of the individuals and the journal itself, asked for an investigation of bullying from professors. The journal concluded the investigation saying that only my followers would know that I was the one being referenced, so were under no fault or obligation to amend the title. They retracted the offer for my response. (I included this saga and the emails to Nick and the BMJ. They chose not to include it.)
I continued to watch the literature. The signals did not vanish: persistent T-cell alterations, exhausted phenotypes, subtle shifts in innate compartments. These were not the province of fringe voices; they appeared in mainstream journals, yet the narrative remained that mild infection was immunologically inconsequential for most. The possibility that repeated or even single mild infections could erode immune resilience was treated as speculative at best, irresponsible at worst. I paid a price for insisting otherwise, not in fame or notoriety, but in the quieter currency of reputation and peace of mind.
Now, in early 2026, the conversation has shifted. A recent Daily Mail article discusses widespread reports of people “getting sicker more often,” with doctors noting struggling immune defences against routine bugs. The piece quotes Danny Altmann again, this time describing the hypothesis of lasting immune harm from mild COVID as “reasonable.”
The idea is presented as fresh and worthy of consideration. There is no mention of the earlier certainty that no such phenotype existed, no acknowledgement that some of us were attacked for articulating precisely this possibility years ago.
The system lacks both memory and foresight.
The absence of reckoning is striking. Those who confidently declared “no phenotype” now entertain the same hypothesis without reference to prior denial. No correction, no apology, no credit to those who endured the backlash. This is not personal grievance alone; it reflects a broader pattern in science where consensus resists challenge until the evidence becomes overwhelming, then absorbs the insight as if it were always obvious. History is replete with such examples (Semmelweis, Warren and Marshall), yet we seem incapable of learning the lesson.
The societal toll compounds the individual one. Delayed acceptance meant delayed mitigation: fewer precautions against reinfection, less urgency in studying immune reconstitution, slower recognition that population-level immune dysregulation might follow waves of mild cases. Excess respiratory illness, rising cancer concerns, unexplained reactivations. These are not abstract. They represent preventable burden born of a refusal to countenance uncomfortable possibilities when they were first raised.
Vindication, when it arrives quietly and without acknowledgement, is a hollow reward. The smears linger longer than the evidence ever did. Yet the deeper failure is not personal. It is the persistent hubris that treats early, mechanistic warnings as threats rather than contributions. Until we cultivate the humility to listen when the data are still emerging, rather than demanding certainty before engagement, we will pay this price again in the next crisis. I hope the record shows that some of us tried to warn you, not for credit, but because the immune system deserved better stewardship than it received.
I am glad I can look upon this period knowing that I did my very best, was ruthless, about conveying what seemed so clear to me, in very unambiguous terms. What is happening was more important than my professional standing as a fragile, early-career immunologist, because I was placed in a niche position as a specialist in T cell aging and death.
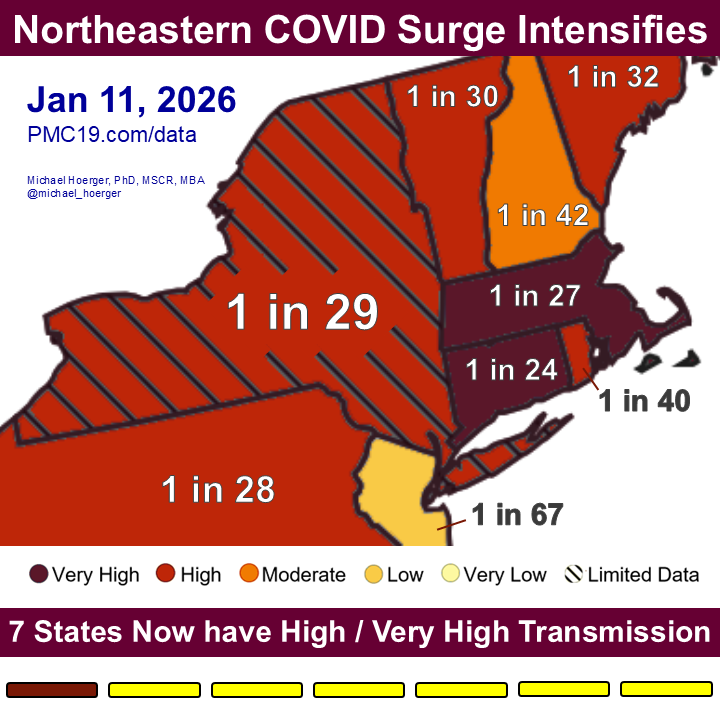
BREAKING: COVlD Surge in the Northeast Intensifies
The CDC indicates 7 states have High or Very High levels. We use harmonized wastewater surveillance data to estimate the prevalence of how many people are actively infectious by state.
Let me highlight a few examples...
🧵1/7
#LongCOVID is an infection-associated chronic condition that usually begins within 3 months of acute COVID-19 and persists ≥3 months, with symptoms that may be continuous or relapsing.
➡️ Global burden: Long COVID is estimated to affect 80–400 million people worldwide.
Incidence: 5–20% in community cases and up to 50% after hospitalization for acute COVID-19.
➡️ Common neuropsychiatric features include:
• Memory & executive dysfunction
• Anxiety, depression
• Headache, sleep disturbance
• Neuropathy
• Loss of taste/smell
• Dizziness, dysautonomia & post-exertional malaise. 1/
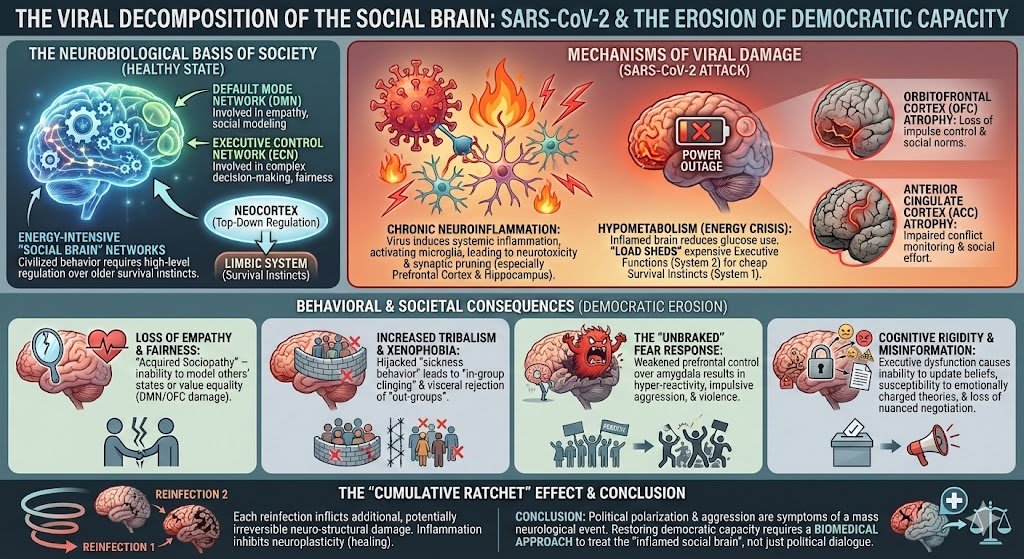
Has police & military behaviour become harsher, more rigid & more escalation-prone since 2020?
This isn’t just about politics or “bad apples”.
There’s a deeper, biological factor being ignored…
SARS-CoV-2
I’m a neurologist, and I’ll explain what’s going on here 🧵.
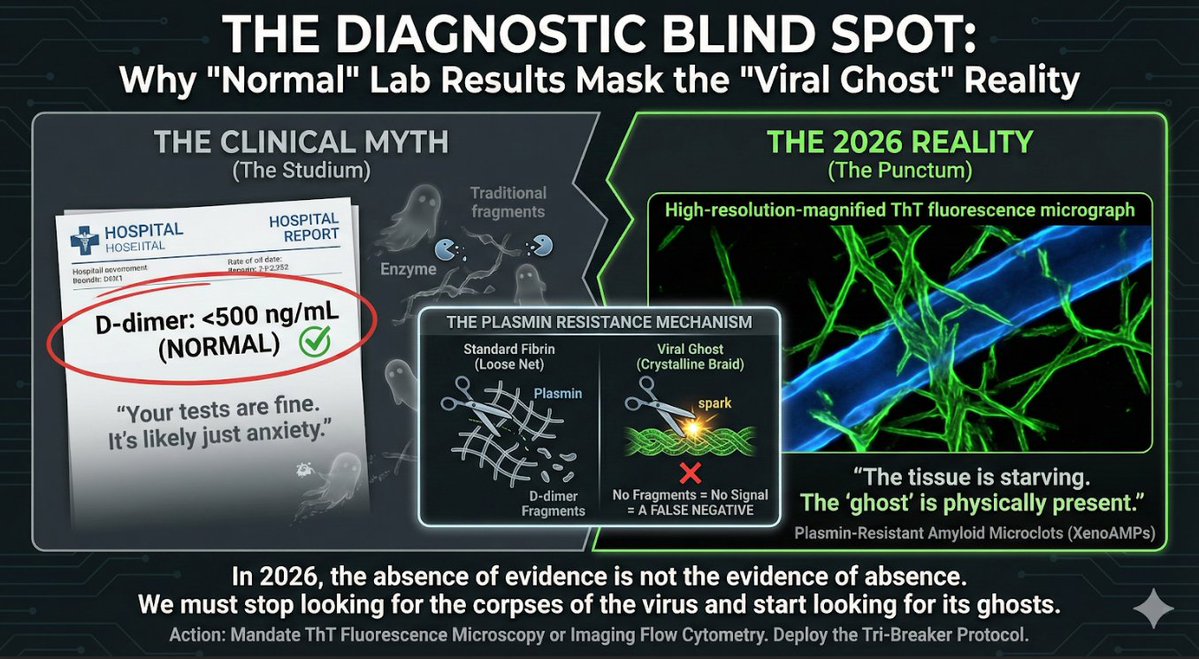
We treat the D-dimer as a diagnostic "all-clear." It is instead a diagnostic blindfold.
SARS-CoV-2 amyloid microclots resist lysis, releasing no D-dimer. You can be starving for oxygen while the labs say you are healthy.
The trap of the invisible: (1/3) 🧵
Statistically 7 out of 10 Americans had COVID in 2025.
Where is the promised immunity?
And how many of them will end up with Long COVID?
@19joho
https://t.co/sZ8tH3gBOR
SARS-CoV-2 damages key brain regions involved in empathy, impulse control, and executive function, leading to impaired social cognition and democratic erosion.
Reinfections compound neuroinflammation, fueling tribalism, misinformation, and fear-driven behavior.🧵
Just published on @PNASNews how #COVID can lead to loss of Dopamine Neurons. In mice, it can be mitigated with treatment, but in humans we don't know yet. Below you see the reduction in TH (rate-limiting enzyme to produce dopamine). This is #LongCovid and also viral Parkinsonism.
Starting the year with a manuscript accepted as first author! 😎 In this study, we show that E. Coli infection during pregnancy can induce loss of neurons in the fetal brain that is not rescued by antibiotic treatment.
More evidence of the impact pathogens can have on the brain!
Massive new vitamin D study just dropped — and it’s getting zero mainstream attention
A 4-year trial with 25,000 adults across the US (led by 140 researchers) found:
Vitamin D3 supplementation significantly preserved telomere length (only 1 year of aging in 4 years).
This follows a 10-year Canadian study (12,000 people) showing ~40% reduced dementia risk with vitamin D.
The message is clear:
Start early, preserve what you have — telomeres don’t reverse once shortened.
2:04 clip inside — game-changing science you need to hear.
SARS Cov 2 causes T cell loss for at least 22 months according to a new study
Sometimes I wonder if RFK's installation and pulling vaccines was meant as a smokescreen for surging illnessess as a result from covid. The so-called "leonardi effect"
https://t.co/0trYzrz8tA
With the high rate of severe influenza we are seeing do NOT take part in family gatherings if you are unwell especially if you are going to be with very young, elderly, or immunocompromised folks.
JUST DON’T DO IT.
Recently, the FDA approved the first vagus nerve neuroimmune modulation device for treatment of rheumatoid arthritis. Today @NatureMedicine the pivotal randomized trial, sham- controlled is published
https://t.co/RUYOpWO8Sf
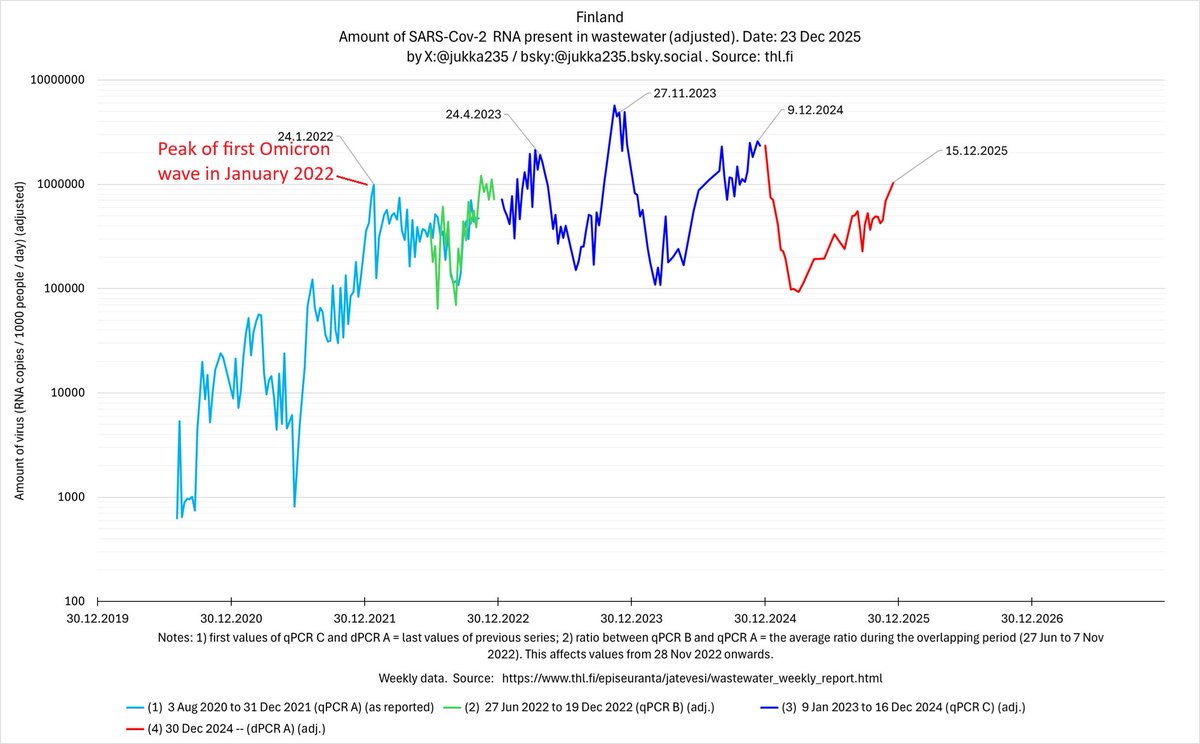
Finland's epidemic 23 Dec 2025: amount of virus in wastewater appears to have risen above the first Omicron wave. Post-Omicron baseline is permanently higher than pre-Omicron; repeated waves are showing no diminishing.
1/x