Just out at @JCOPO_ASCO:
we analyzed nearly
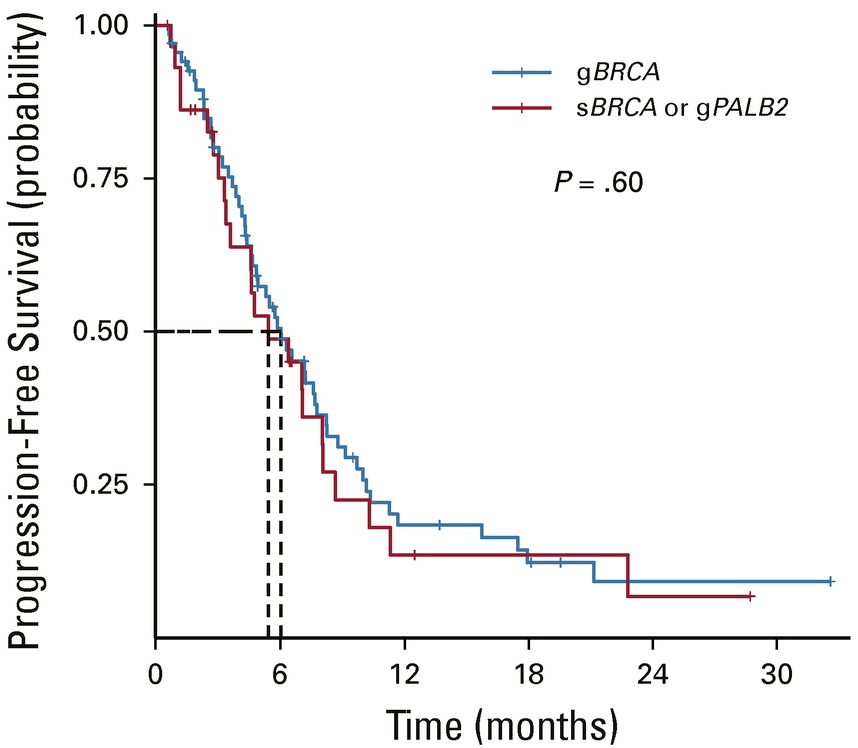
30K breast cancers and reported the specific frequencies of alterations in the HRD pathways. Also showed that somatic BRCA and germline PALB2 derive similar benefit to gBRCA @MayoClinic@BIDMChealth@DanaFarber https://t.co/Wbb7NijEka
@gilmarmendes Vocês do @STF_oficial são uma vergonha nacional. Defendem bandidos e não tem nenhum compromisso com o cidadão de bem, só com os companheiros.
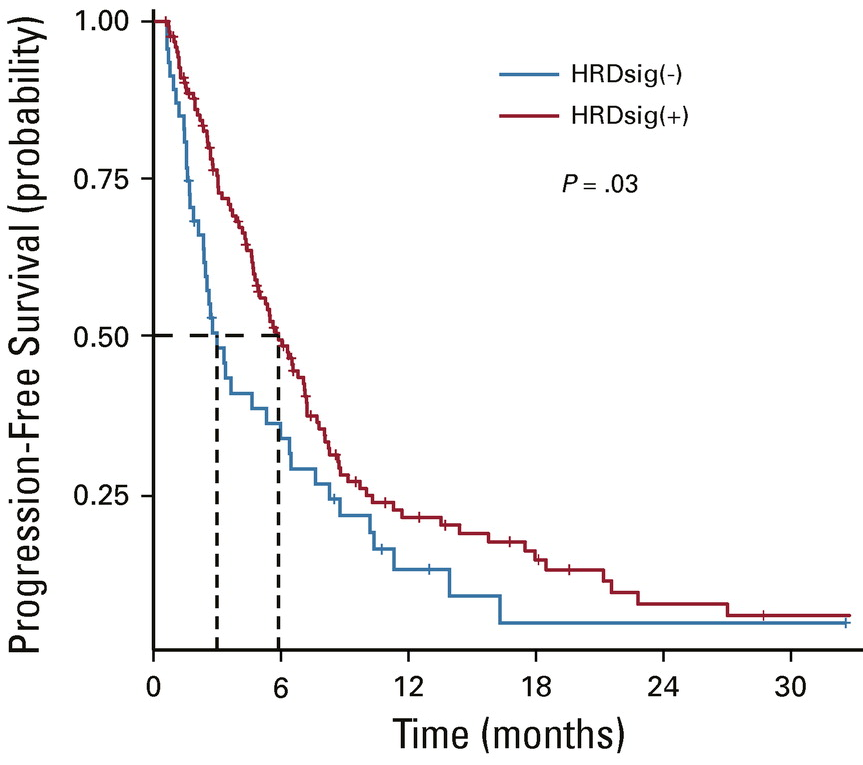
Our manuscript is out exploring real-world outcomes on PARPi in breast cancer. Patients with germline and somatic BRCA alterations have similar benefit (OS and PFS). A scar-based biomarker of HRD (HRDsig) is associated with favorable outcomes. https://t.co/CViUReG3vb
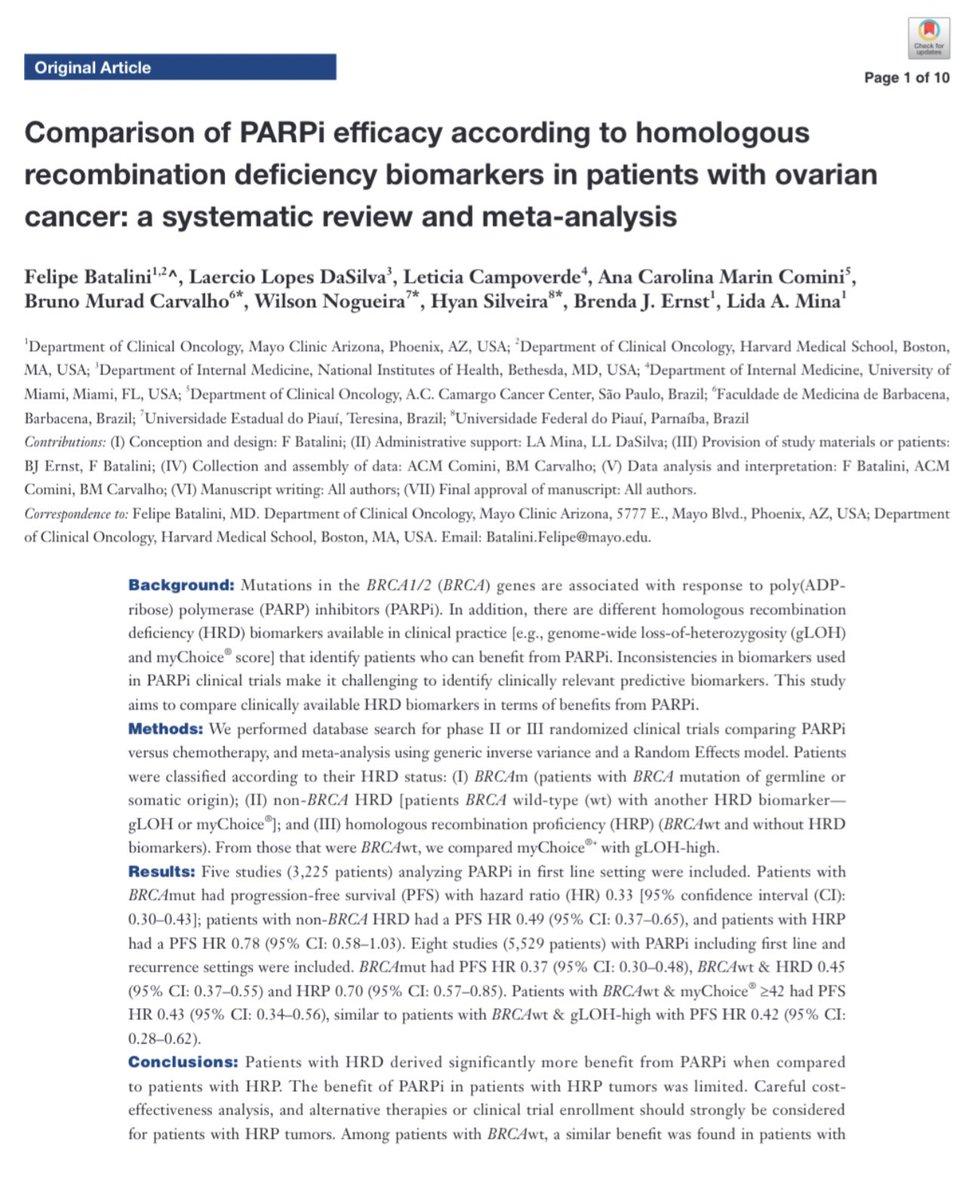
Check out our new publication about PARPi in ovarian cancer https://t.co/jBJVUcM7tW. I’m so lucky to have met and worked with @FelipeBatalini and @laerciolopesMD who are such an inspiration to me. #LatinosInOncology
@Dr_RShatsky Yes, this is a big problem in Arizona as well. Patients being ripped off paying tens or hundreds of thousands of dollars for “alternative” treatments. Big scam!
The non-coding RNA miR-22 promotes EMT transition and metastasis in breast cancer. Inhibiting miR-22 with ASO suppressed mets and prolonged survival in mice. Thanks to collaborators and mentor @ivlacho for allowing me to help with the bioinformatics! https://t.co/5OSP9uc51Q
Pretty clear after @SABCSSanAntonio and @ASCO meetings that "HER2 low" is not a biological thing. HER2 0 and HER2 low tumors behave the same clinically. Serial testing shows that lots of HER2 1+/2+ are HER2 0 on later testing, or vice versa.
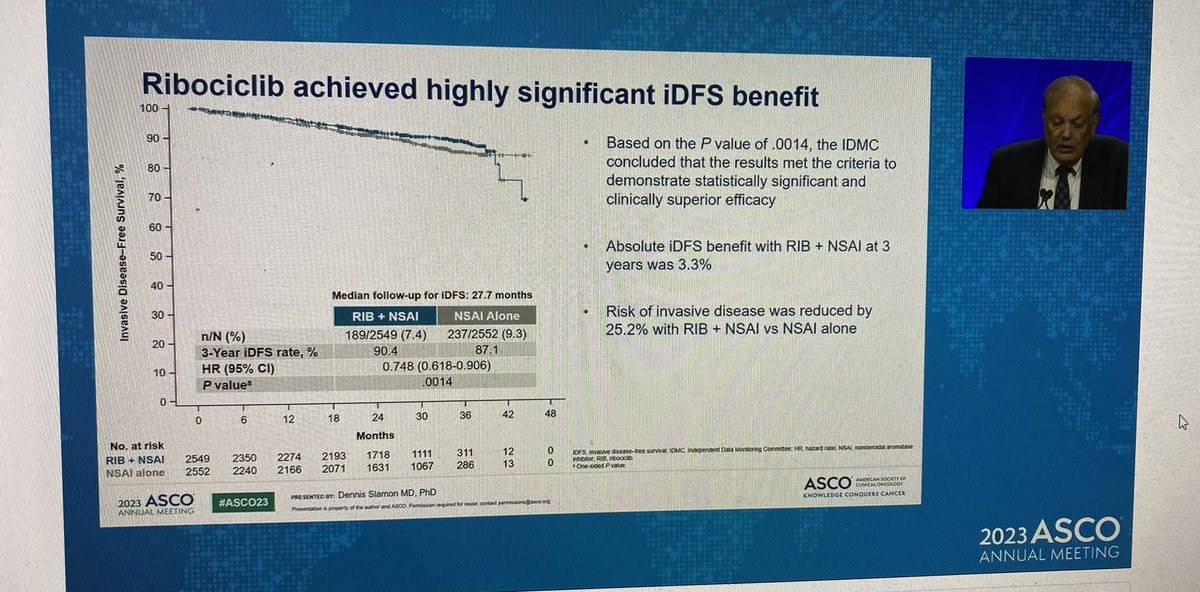
We’ll need to reconcile NATALEE and MonarchE. Different populations, side effect profile, and duration of therapies. Someone from the audience also brought up the estimated cost of half million dollars for the 3 years of adjuvant ribociclib. Abemaciclib probably not far behind.
@ASCO NATALEE trial shows positive results, iDFS benefit with addition of ribociclib to adjuvant ET
✨included pts w/o LN+ disease (anatomic stage II) & used ribo dose of 400mg BID
✨inc LFT & neutropenia significant in ribo arm
✨potential for practice change, pending OS
We compared commercially available HRD biomarkers in terms of response to PARPi in ovarian cancer. BRCA respond the best, Myriad MyChoice and gLOH are comparable. HR proficient should not be on PARPi. Thanks to @laerciolopesMD@LetyCampoverde and others https://t.co/AnU5SzhgMA
I’m glad the FDA went back and made sure olaparib was approved only for the right patients with metastastic prostate cancer, THOSE WITH BRCA mutations. I’m sure we still missing other HRD alterations, so we will keep working on biomarkers.
Register now to attend @OncLive's Institutional Perspectives in Cancer virtual event for #BreastCancer, led by @MayoClinic experts @mpgoetz and @DrJudyBoughey. See the overview, featured topics and register here: https://t.co/CfuCbQZBGj
On #MemorialDay, we remember those who lost their lives in service to our country. From the BCRF family to yours, wishing you a peaceful holiday weekend.
Photo: Valentino Funghi/Unsplash
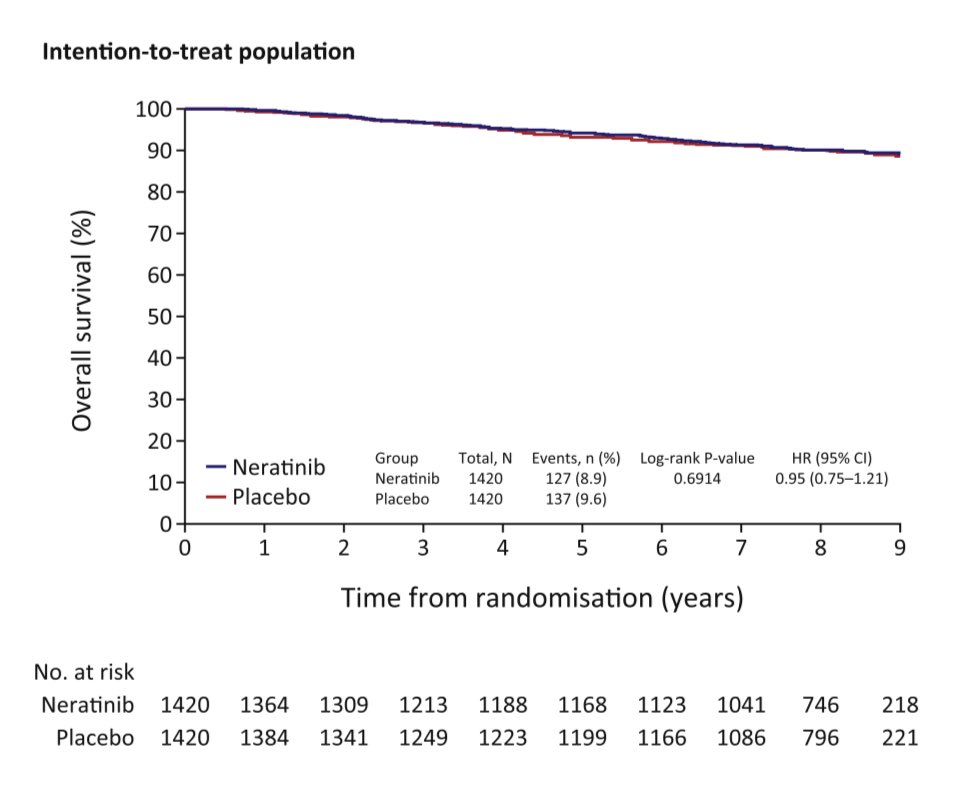
Final analysis of overall survival in ExteNET. After 8 years of follow up, there was no OS benefit with extended neratinib in the ITT, with an 8-year OS of 90% in both arms. A trend in better OS with neratinib is seen among HR+ patients (OS HR 0.80).
https://t.co/yXKwokSi09
@PTarantinoMD In real life, the benefit is only likely to be less, now that we all use T-DM1 for pts without a pathCR. I see very little role (perhaps none) for neratinib in the adjuvant setting.
@PTarantinoMD Yes, thanks for sharing these important OS data, a major need for pts with platinum-resistant ovarian cancer. It’s also nice to see biomarker-driven therapies: the folate receptor αlpha (FR��) in this case. We will need testing to become more widely available!!