@WilliamWallace Wonder how this curves out with the Clover method now used a most Starbucks. Higher pressure, over a couple minutes. Almost espresso like.
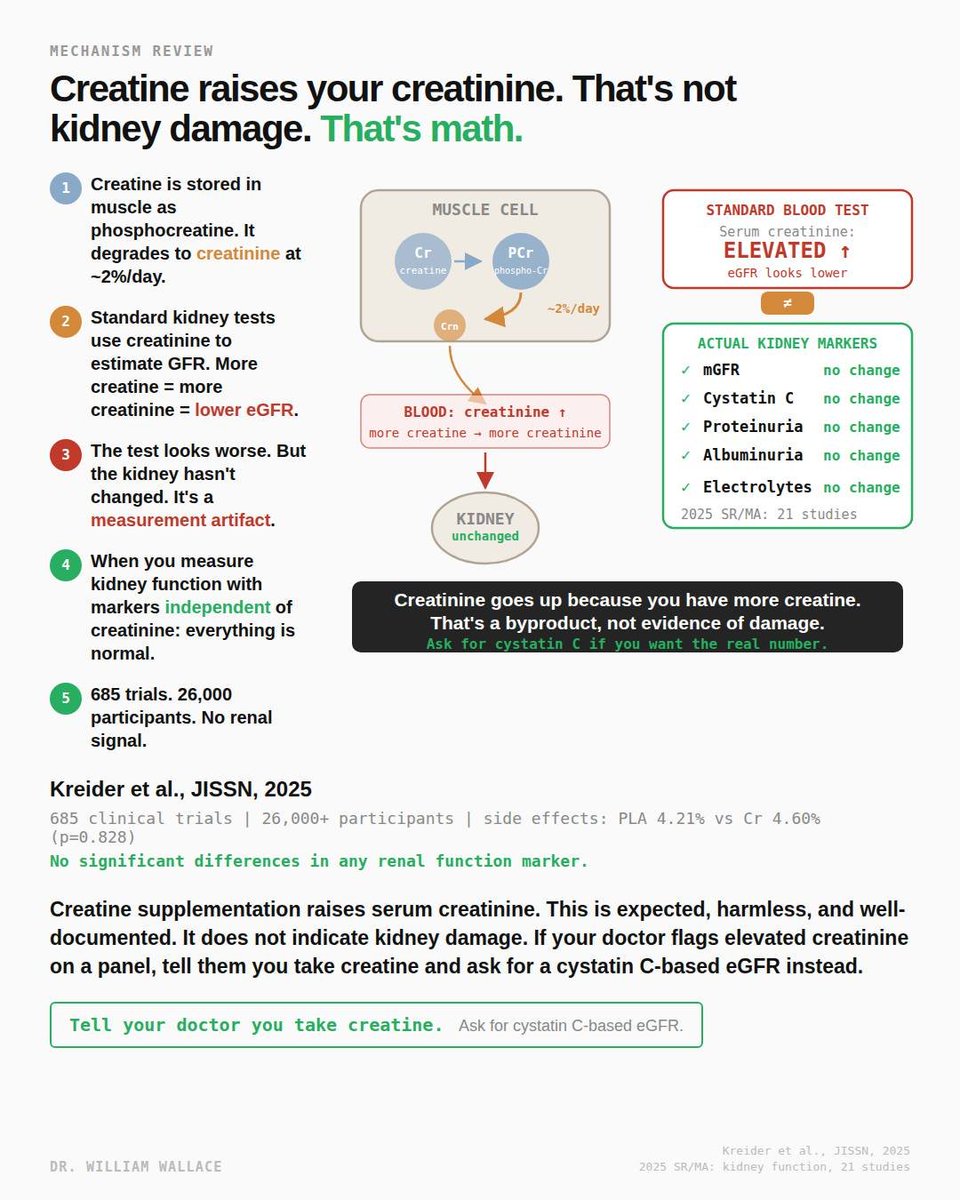
The most persistent myth about creatine is that it damages your kidneys. The concern comes from a real observation interpreted incorrectly: creatine supplementation raises serum creatinine. On a standard metabolic panel, elevated creatinine triggers a lower estimated glomerular filtration rate, which is the primary marker doctors use to assess kidney function. The number looks worse. The kidney is fine.
Here is why. Creatine is stored in skeletal muscle primarily as phosphocreatine. It degrades spontaneously and irreversibly into creatinine at a rate of approximately 2% per day. Creatinine is a waste product. It is filtered by the kidneys and excreted in urine. Standard kidney function tests measure serum creatinine and use it to calculate eGFR. The assumption built into the equation is that creatinine production is relatively constant. When you supplement creatine and increase total body creatine stores, you produce more creatinine. The equation interprets this as reduced kidney filtration. It is not. It is more substrate producing more waste at the same filtration rate.
A 2025 systematic review and meta-analysis of 21 studies examining the effect of creatine supplementation on kidney function confirmed this directly. Creatine was associated with a small but statistically significant increase in serum creatinine (mean difference: 0.07 micromol/L). However, there were no changes in measured GFR, cystatin C, proteinuria, or albuminuria. These are the markers that actually reflect kidney health independent of creatinine metabolism. The creatinine went up. Every other renal marker was unchanged.
Kreider et al. (2025, JISSN) conducted the largest safety analysis of creatine to date, reviewing 685 human clinical trials involving over 26,000 participants. Side effect prevalence was virtually identical between creatine and placebo groups: 4.60% vs 4.21% (p=0.828). No significant differences were observed in any of the 49 side effects evaluated, including all markers of renal function and health. Some of these trials ran for up to 14 years.
The case reports that occasionally surface involving creatine and kidney injury almost always involve individuals with pre-existing kidney conditions, concurrent use of other substances known to affect renal function, or extreme exercise leading to rhabdomyolysis. These are confounded cases, not evidence of a causal relationship between creatine and kidney damage in healthy individuals.
One practical issue worth noting: if you take creatine and get routine bloodwork, your doctor may flag the creatinine and eGFR numbers. This is not because your kidneys are failing. It is because the standard test was not designed with creatine supplementation in mind. The solution is straightforward. Tell your doctor you take creatine and ask for a cystatin C-based eGFR instead. Cystatin C is produced at a constant rate by all nucleated cells and is not affected by creatine intake. It gives you the real kidney function number without the artifact.
For individuals with pre-existing kidney disease, the data is more limited. Most creatine studies have been conducted in healthy populations. While pilot studies in hemodialysis patients have not shown adverse effects beyond the expected creatinine increase, caution is warranted for anyone with diagnosed renal impairment until more data is available.
https://t.co/99gNpJRd0c
https://t.co/PmZXxOGqWg