Top Tweets for #teachingpoints

Collapsing glomerular lesions are aptly named, given the prominent “collapse” of glomerular tuft capillary loops. There is also hyperplasia and hypertrophy of overlying epithelial cells, and protein resorption droplets may be abundant (see arrow).
#TeachingPoints #kidneypath #renal #pathology


🌍✨ IGCC 2025 – Pancreas Session Highlights ✨🌍
🎤 Great talk by prof. @AntonioFaccior6 with #teachingpoints, Italy 🇮🇹
📍 International Gastrointestinal Cancer Conference (IGCC 2025)
🔬 1️⃣ Functioning vs Non-Functioning PanNETs
Functioning ≈ 10% (insulinoma most common) → always treat to control symptoms 💉
Non-Functioning ≈ 90% → often incidental and managed based on size and risk 📏
📊 2️⃣ Guideline Highlights (ENETS / NANETS)
< 10 mm → Observation 👀
11–20 mm → Individualized management depending on growth and location ⚖️
> 20 mm → Surgery indicated 🔪
📚 3️⃣ ASPEN Study Insights
20% of patients showed aggressive histologic features 😮
Risk factors: pancreatic duct dilatation and tumor > 1 cm
Many surgical decisions were driven by patient or surgeon preference 💭
Highlights the importance of active surveillance for low-risk lesions 🕊️
🔥 4️⃣ EUS-RFA in NF-PanNET ≤ 20mm
Safe and effective for small, stable lesions 💪
⚠️ Caution: proximity to the main pancreatic duct (MPD) increases risk 🚫
Decision balance:
🟢 Stable → Surveillance
🟠 Intermediate → EUS-RFA
🔴 MPD dilation → Surgery
🧪 5️⃣ EUS-RFA vs Surgery (Propensity-Matched Study)
Comparable clinical efficacy ⚖️
Fewer adverse events and shorter hospital stay 🏥⬇️
Supports a minimally invasive future for selected PanNET patients 🌟
🚀 Expanding the Role of EUS-RFA in Pancreatic Tumors
✅ Present and Future Indications
First-line treatment for insulinomas > 1 mm from the MPD
Palliation of symptoms in functional PanNETs unfit for surgery
Small NF-PanNETs (≤ 20 mm) with patient preference for minimally invasive therapy
MEN-1 patients with multifocal disease or high surgical risk — RFA as adjunct therapy
💉 Why Ablate Pancreatic Cancer?
Only a minority of patients are eligible for resection 🩺
EUS-RFA offers local tumor control and potential synergy with systemic therapy 💊
Improves tumor perfusion → enhanced drug delivery to hypoperfused zones 📈
🧠 Immunologic and Biologic Synergy
RFA triggers antigen presentation and anti-tumor immune responses 🧩
Acts as an in-situ vaccine, potentially enhancing immunotherapy efficacy
Represents a new frontier in endoscopic oncology and immune modulation 🔥
📈 PELICAN Trial Highlights
Patients with unresectable locally advanced pancreatic cancer (LAPC)
Randomized to chemotherapy ± RFA 🧪
Median overall survival ≈ 12 months in both arms — proving feasibility and safety ✅
❓ Unanswered Questions / Future Directions
When to integrate RFA — before, during, or after chemotherapy?
Best sequence with radiotherapy?
What defines the ideal candidate and optimal thermal dose?
Impact on long-term survival → needs multicenter randomized trials 🧪
🏁 Conclusions and Future Recommendations
> ✅ EUS-RFA is feasible, safe, and effective for selected pancreatic lesions.
⚖️ Careful patient selection is vital to maximize benefit and minimize risk.
🧩 The future lies in well-designed multicenter trials integrating EUS-RFA into multimodality care.
🌟 A truly exceptional session blending science, innovation, and clinical judgment — showcasing how advanced endoscopic therapies are shaping the future of pancreatic cancer care. 👏🔥
#IGCC2025 #PancreasSession #EUSRFA #PancreaticCancer #PanNET #Endoscopy #Innovation #Gastroenterology #MedicalEducation #Immunotherapy #MinimallyInvasive #EvidenceBasedMedicine #SaudiArabia 🇸🇦

#TeachingPoints There is a histopathologic spectrum to the casts that can be seen in light chain cast nephropathy. A portion of this spectrum is shown in these photomicrographs of renal biopsies stained with PAS. All three of these cases had casts with light chain restriction by immunofluorescence. Photomicrograph A shows the classic PAS-negative cast with a cellular reaction. The casts in Photomicrograph B have an elongated crystalline appearance. The casts in Photomicrograph C stain weak by PAS and have more of a granular appearance. It is important for the renal pathologist to be aware of this histopathologic spectrum though there is no known clinical significance to the variation in appearance by light microscopy.
#Renal #RenalPath



#TeachingPoints Patients with warfarin-related nephropathy present with an acute rise in serum Cr after becoming supratherapeutic on warfarin therapy (INR>3). The renal biopsy findings of warfarin nephropathy include acute tubular injury, occlusive RBC casts in tubular lumens, and RBCs in Bowman’s space. The diagnosis of warfarin nephropathy cannot be made exclusively on biopsy and requires clinical correlation as other glomerulonephritides can have similar changes. Nevertheless, the renal pathologist should suspect warfarin nephropathy when the number of RBC casts is disproportionate to the degree glomerular injury (e.g. mild mesangial immune complex deposition without proliferative changes yet there are numerous RBC casts).
#Renal #RenalPath


#TeachingPoints The patient is a 70 years old male who presents with a creatinine of 5 mg/dl and a history of primary myelofibrosis. The biopsy shows a kidney with severe glomerular and tubulointerstitial chronicity, approaching end-stage kidney disease from arterionephrosclerosis. Interestingly, circulating nucleated red blood cells were identified in the arteries and peritubular capillaries. Although not representing a specific kidney disease, the presence of nucleated red blood cells within the circulation points toward premature release of erythroid precursors from the bone marrow. This finding is has been reported in the setting of a space occupying lesion in the bone marrow from metastases or in myeloproliferative disorders.
#Renal #RenalPath



#TeachingPoints A 54-year-old man with a history of hypertension and hypercholesterolemia presented with complaints of generalized “muscle stiffness” and cola-colored urine. He was found to have markedly elevated serum creatinine and creatine kinase levels. A renal biopsy showed acute tubular injury with numerous pigmented casts (Fig 1), which were proven to be myoglobin casts by immunohistochemistry (Fig 2).
The etiology of the patient’s myoglobinuria was thought to be statin medication, the dose of which had recently been increased.
Here is a link to a recent article describing the morphologic spectrum of myoglobin casts in renal biopsies: https://t.co/C3tOJarqqX. #Renal #RenalPath


#TeachingPoints The silver impregnation stain is a key method of identifying basement membranes in human tissue, and its application in renal pathology is nearly universal. Notice in this image (Fig 1) how clearly demonstrating the capillary basement membrane using the silver stain allows one to distinguish cells within the capillary lumens from those “extracapillary” cells which are forming the glomerular crescent.
In 1951, David B. Jones, MD, reported the development of a periodic acid silver reaction adapted specifically for the kidney which better highlighted basement membranes (American Journal of Pathology, Dec 1951: 991-1009). Most renal pathologists still rely heavily on the Jones stain in their daily diagnostic pathology practice and are grateful to the many contributions made by Dr. Jones to the field of renal pathology (Fig 2).
#Renal #Pathology


#TeachingPoints A renal biopsy was performed on this 78 year old male with history of diabetes mellitus, hypertension and monoclonal gammopathy of undetermined significance (IgG kappa).
The serum creatinine at presentation was 3.2 mg/dl and UPCR was 1.8 g/g. The glomeruli diffusely show nodular mesangial expansion with segmental sclerosis and negative Congo red staining, consistent with diabetic glomerulosclerosis. On the other hand, the arteries and arterioles diffusely show deposition of a PAS pale, weakly argyrophilic, Congo red positive amorphous material which shows apple green birefringence upon polarization, consistent with amyloid deposits (Fig 1 and 2, Congo red). Similar deposits are not identified within the glomeruli or tubulointerstitium.
Immunofluorescence shows strongly positive vascular “smudgy” staining for kappa light chain, along with diffusely negative staining for heavy chains and lambda light chain. These findings are characteristic of AL amyloidosis (kappa-type) with exclusive vascular involvement.
Patients with underlying plasma cell dyscrasias or lymphoproliferative disorders may develop different forms of renal disease related to deposition of monoclonal immunoglobulins, an example of which is AL amyloidosis. AL amyloidosis may affect any, and frequently all compartments of the renal parenchyma, including glomeruli, vessels and tubulointerstitium. Such as in this case, a small subset of patients may display amyloid deposits restricted to the vascular structures. These patients have been shown to present with worse renal function and lower levels of proteinuria when compared to patients with diffuse involvement (see reference). Furthermore, kappa light chain-type amyloidosis is proportionally more frequent then lambda-type in patients with vascular-limited disease than in those patients with diffuse involvement.
#PathTwitter #RenalPath




#TeachingPoints The IgA nephropathy Oxford Classification was first published in 2009 by a working group of nephrologists and renal pathologists representing the Renal Pathology Society and International IgA Nephropathy Network. The lesions currently scored include mesangial hypercellularity, endocapillary hypercellularity, segmental sclerosis, tubular atrophy/interstitial fibrosis, and cellular/fibrocellular crescent formation. Two of these lesions, crescent formation (A) and mesangial hypercellularity (B), are shown here. For the purposes of the Oxford classification, mesangial hypercellularity is defined as >3 mesangial cell nuclei in a mesangial area not adjacent to the vascular pole (in sections cut to 3 micron thickness). #IgANDay #IgANaware


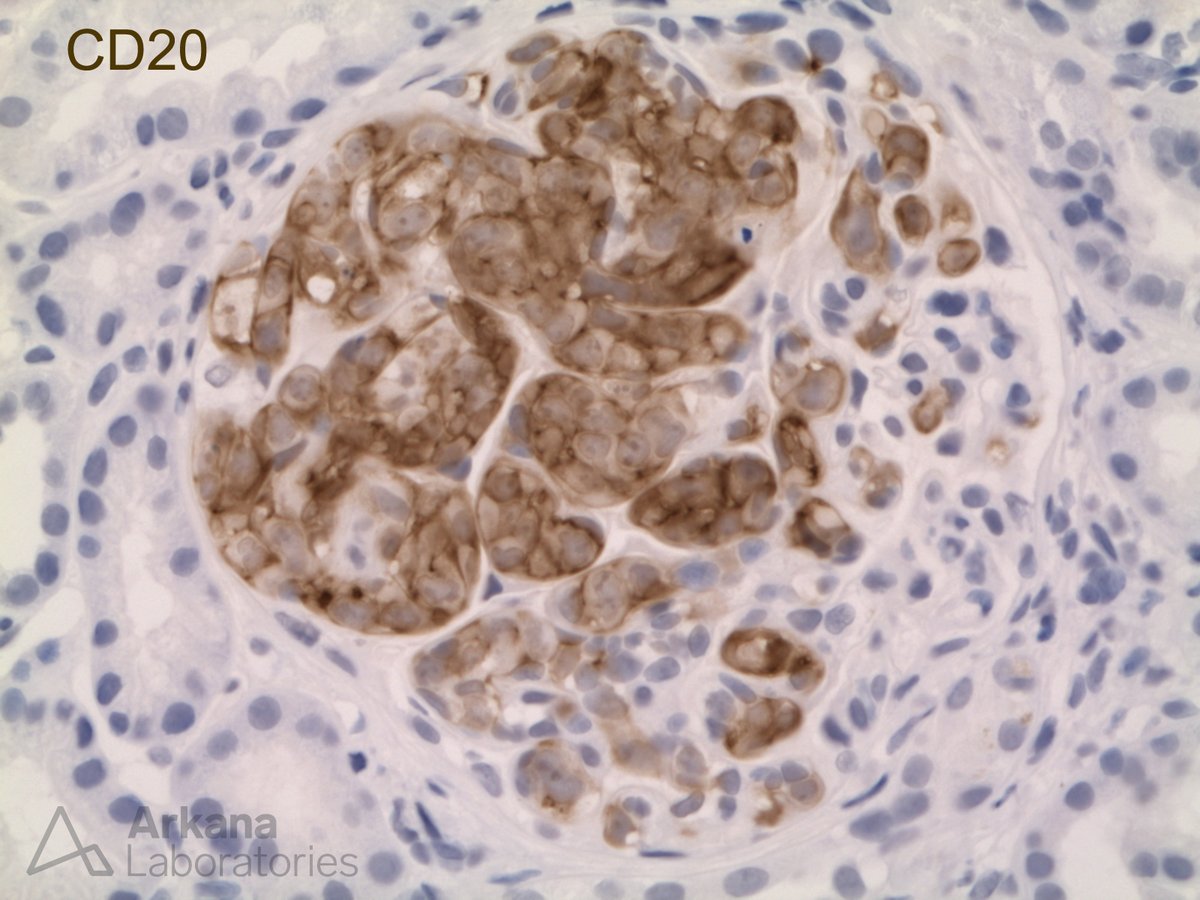
#TeachingPoints A 75 year old woman presented for her annual checkup with no complaints. She had a past medical history of hypertension and her blood pressure at this visit was 160/80. Laboratory findings were significant for an elevated serum creatinine at 2.1 mg/dL (baseline 1.0 mg/dL) as well as proteinuria of 855 mg/24 hr. All serologies, including proteinase-3, myeloperoxidase, and anti-nuclear antibodies were negative. A kidney biopsy was performed to evaluate the decreased kidney function and proteinuria. It revealed a total of five glomeruli were present, three of which showed a global endocapillary proliferation of large atypical cells with frequent mitotic figures (Photomicrographs A and B). These atypical cells were isolated to the glomeruli and stained positive for CD20 . The remaining glomeruli did not contain any proliferative changes. Electron microscopy and immunofluorescence were both negative for immune deposits.
This is a rare subtype of extranodal diffuse large B cell lymphoma that has been known in the past by several different names and was originally thought to be a proliferation of endothelial cells; however, it is currently classified by the WHO as “intravascular large B-cell lymphoma” (IVBCL). IVLBCL most frequently affects adults over 60 and is typically widely disseminated in the small vessels of many organs at presentation. It most often presents without tumor masses or lymphadenopathy and lymphoma cells are usually not seen in peripheral blood smears. Clinical symptoms are highly variable and usually result from the occlusion of small vessels. The vast majority of cases are diagnosed in the bone marrow, liver, spleen, or skin. However, there are case reports of the diagnosis being made by kidney biopsy. In these cases, it usually manifests with slowly progressive renal failure and proteinuria which is frequently in the nephrotic range.
#RenalPath


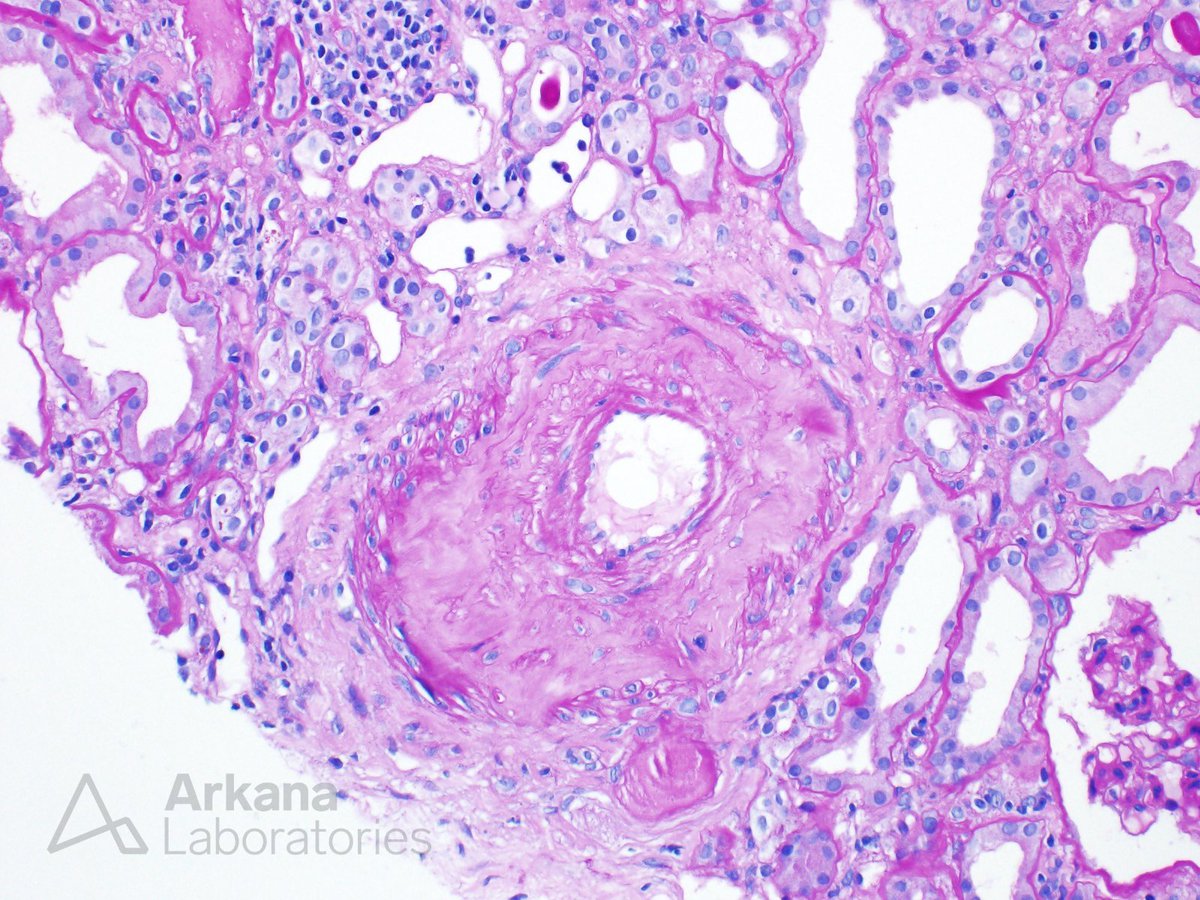
#TeachingPoints A very common vascular histologic finding in patients with hypertensive nephrosclerosis is arteriosclerosis. In advanced lesions, such as this example, there is prominent intimal fibrosis with narrowing of the vessel lumen. The replacement of smooth muscle cells in the tunica media by fibrous tissue is thought to result from collagen and elastic tissue synthesis by myointimal cells. The degree of intimal fibrosis is thought to be more closely associated with elevated blood pressure than the degree of hyaline arteriolosclerosis.
#TeachingPoints The patient is a 32 year-old African American female who presents with hypertensive urgency, positive ANA, positive anti-RNA polymerase III antibody, schistocytes on the peripheral smear, forgetfulness, and a creatinine of 2. On physical examination, the skin is tight and thickened along the face ("masked face"), back, and proximal arms. Urinalysis shows 250 mg of proteinuria and no active urine sediment. Serologies for c-ANCA, p-ANCA, dsDNA, and anti-GBM are negative.
The patient has scleroderma renal crisis. Learn more about this case on our blog:
https://t.co/IOoi1WQqOd
#TeachingPoints The differential diagnosis of kidney injury in CLL/SLL patients.
There are many causes of decreased kidney function in patients with chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL), and a renal biopsy may provide a definitive diagnosis.
Prerenal etiologiesinclude poor oral intake, sepsis, and heart failure. Intrarenal causes include diseases of the glomeruli (e.g. minimal change disease, MPGN pattern glomerulopathy, membranous glomerulopathy), tubules (e.g. toxic or ischemic tubular injury/necrosis, light chain cast nephropathy), interstitium (e.g. acute interstitial nephritis caused by infection or drugs), and vasculature (e.g. TMA). The biopsy shown in this image illustrates infiltration of the kidney parenchyma by the lymphoid neoplasm (characteristic immunophenotypic studies not shown). Postrenal causes include obstruction (e.g. extrarenal tumor mass, lymphadenopathy) and uric acid nephropathy related to tumor lysis syndrome, among others.
Reference:
Rimda Wanchoo, et al. Renal involvement in chronic lymphocytic leukemia. Clinical Kidney Journal, sfy026, https://t.co/RkGHD8tg1X

#TeachingPoints Cortical microabscess formation is a clue to the presence of an infectious organism. Various bacteria, viruses, fungi, and even parasites may cause similar appearing lesions. This biopsy is taken from a renal transplant patient with acute kidney injury and microscopic hematuria. The low-power image shows a densely mixed cellular infiltrate involving the tubulointerstitium (Fig. 1). Higher magnification shows tubulitis with intratubular leukocytes and rare structures suspicious for fungal elements (Fig. 2). Gomori methenamine silver staining confirms the presence of budding yeast forms (Fig. 3 arrow) with hyphae and pseudohyphae. Fungal isolates from urine culture showed colony morphology characteristics consistent with Candida species.



#TeachingPoints The patient is a 75 year-old female who presents with proteinuria, a necrotic skin lesion on her lower extremity, and a creatinine of 5.5 mg/dL. Her serum complement levels (C3/C4) are low. Serologies for ANA, dsDNA, rheumatoid factor, c-ANCA, p-ANCA, anti-GBM, and ASO are negative. Her cryoglobulins are positive. Image 1 shows hyaline thrombi and image 2 shows mild interstitial fibrosis. Images 3, 4, 5, and 6 are IgG, IgM, kappa, and lambda, respectively. This is a case of Type 1 cryoglobulinemia.
Type 1 cryoglobulins are composed of a single monoclonal immunoglobulin that reversibly participates at low temperature (<37C). Type 1 cryoglobulinemia develops in the setting of protein-secreting monoclonal gammopathies such as MGUS or a B-cell lineage malignancy (multiple myeloma, CLL, Waldenstrom's). Type 1 cryoglobulinemia frequently has cutaneous manifestations such as ulcerations and necrosis. In the largest study of type 1 cryoglobulinemia published in 2014, 32% of the patients had renal involvement. The level of cryoglobulins in the blood does not correlate with renal involvement. Severe manifestations are more frequent in patients with IgG cryoglobulins (as in this case) as compared with IgM cryoglobulins. The majority of patients with type 1 cryoglobulinemia receive a cytoreductive treatment to address their underlying lymphoproliferative disorder or monoclonal gammopathy. Recent data has shown that patients who lack overt malignancy (monoclonal gammopathy of renal significance) should receive chemotherapy to treat the "dangerous small B cell clone." Overall, long-term survival is similar to patients with mixed cryoglobulinemia.
https://t.co/sPCzdeiQqx
https://t.co/DZvNPUJzuP




#TeachingPoints Tubulointerstitial nephritis with uveitis (TINU) was first described as a distinct entity by Dobrin, et al. in 1975. TINU primarily affects young females (medial age 15 years) who commonly have associated systemic signs and symptoms of the disease including weight loss, fever, fatigue, malaise, abdominal or flank pain, arthralgias or myalgias, and headache. The syndrome is likely underdiagnosed as a result of the asynchronous presentation of the renal and ocular symptoms. In fact, the ocular symptoms lag behind the interstitial nephritis diagnosis in two-thirds of cases by up to 14 months. TINU should be considered a diagnosis of exclusion only after other etiologies of uveitis have been excluded such as Sjögren syndrome, sarcoidosis, syphilis, SLE, Behçet disease, IgG4-related disease, toxoplasmosis, and ANCA-associated disease. The renal biopsy findings of TINU are relatively nonspecific, consisting of interstitial inflammation and tubulitis. The interstitial inflammatory cells are predominantly lymphocytes in most cases (as shown in the photomicrographs here). However, the infiltrate is reported to include eosinophils in one-third of cases, neutrophils are in 25% of biopsies, and non-caseating granulomas in approximately 10% of renal biopsy specimens. The tubulitis is often most severe in proximal tubules which, as shown here, can also display lymphocyte cuffing. Immunofluorescence studies are negative throughout the tissue including the tubular basement membranes. #RenalPath
References:
Dobrin RS, Vernier RL, Fish AJ. Acute eosinophilic interstitial nephritis and renal failure with bone marrow-lymph node granulomas and anterior uveitis. Am J Med 1975; 59: 325-333.
Mandeville JTH, Levinson RD, Holland GN. The Tubulointerstitial nephritis and uveitis syndrome. Survey of ophthalmology 2001; 46: 195-208.
Herlitz LC, Chun MJ, Stokes MB, et al. Uveitis and acute renal failure. Kidney Int 2007; 72: 1554-1557.



#TeachingPoints The image shows two globally sclerotic glomeruli exhibiting the so-called “obsolescent” pattern of glomerular sclerosis. The two key histologic features in this pattern are the shrunken and retracted glomerular capillary tuft (arrowhead) and the fibrous matrix which replaces Bowman’s space (arrow). This pattern of sclerosis is thought to result from reduced glomerular perfusion secondary to arteriosclerosis of small renal arteries. In contrast, the so-called “solidified” pattern of glomerular sclerosis (not shown), in which the entire remnant glomerulus is replaced by fibrous matrix, shows the strongest association with underlying APOL1 risk variants in the setting of chronic kidney disease.

#TeachingPoints Chronic uric acid nephropathy results from deposition within the renal parenchyma of monosodium urate monohydrate. While the disease may occur in the setting of increased uric acid production, it is overwhelmingly more common in the setting of decreased uric acid excretion. Histologically, chronic uric acid nephropathy is characterized by the presence of tubulointerstitial microtophi within the renal medulla, associated with interstitial fibrosis and inflammation. Microtophi are deposits of monosodium urate crystals surrounded by giant cells, epithelioid histiocytes and lymphocytes, which may have a radial needle-like cleft (Fig 1 – blue arrow; Fig 2) or amorphous morphology (Fig 1 – orange arrow; Fig 3 [trichrome]). While the crystals are dissolved during formalin fixation, their birefringence is readily seen on frozen or alcohol-fixed tissue. In addition to the tubulointerstitial changes, the glomeruli may show mesangial sclerosis, thickening of the glomerular basement membranes and segmental subendothelial widening by electron microscopy.
![arkanalabs's tweet photo. #TeachingPoints Chronic uric acid nephropathy results from deposition within the renal parenchyma of monosodium urate monohydrate. While the disease may occur in the setting of increased uric acid production, it is overwhelmingly more common in the setting of decreased uric acid excretion. Histologically, chronic uric acid nephropathy is characterized by the presence of tubulointerstitial microtophi within the renal medulla, associated with interstitial fibrosis and inflammation. Microtophi are deposits of monosodium urate crystals surrounded by giant cells, epithelioid histiocytes and lymphocytes, which may have a radial needle-like cleft (Fig 1 – blue arrow; Fig 2) or amorphous morphology (Fig 1 – orange arrow; Fig 3 [trichrome]). While the crystals are dissolved during formalin fixation, their birefringence is readily seen on frozen or alcohol-fixed tissue. In addition to the tubulointerstitial changes, the glomeruli may show mesangial sclerosis, thickening of the glomerular basement membranes and segmental subendothelial widening by electron microscopy.](https://pbs.twimg.com/media/GGZ-cZ9W8AEcOvA.jpg)
![arkanalabs's tweet photo. #TeachingPoints Chronic uric acid nephropathy results from deposition within the renal parenchyma of monosodium urate monohydrate. While the disease may occur in the setting of increased uric acid production, it is overwhelmingly more common in the setting of decreased uric acid excretion. Histologically, chronic uric acid nephropathy is characterized by the presence of tubulointerstitial microtophi within the renal medulla, associated with interstitial fibrosis and inflammation. Microtophi are deposits of monosodium urate crystals surrounded by giant cells, epithelioid histiocytes and lymphocytes, which may have a radial needle-like cleft (Fig 1 – blue arrow; Fig 2) or amorphous morphology (Fig 1 – orange arrow; Fig 3 [trichrome]). While the crystals are dissolved during formalin fixation, their birefringence is readily seen on frozen or alcohol-fixed tissue. In addition to the tubulointerstitial changes, the glomeruli may show mesangial sclerosis, thickening of the glomerular basement membranes and segmental subendothelial widening by electron microscopy.](https://pbs.twimg.com/media/GGZ-a8cXgAA7UbJ.jpg)
![arkanalabs's tweet photo. #TeachingPoints Chronic uric acid nephropathy results from deposition within the renal parenchyma of monosodium urate monohydrate. While the disease may occur in the setting of increased uric acid production, it is overwhelmingly more common in the setting of decreased uric acid excretion. Histologically, chronic uric acid nephropathy is characterized by the presence of tubulointerstitial microtophi within the renal medulla, associated with interstitial fibrosis and inflammation. Microtophi are deposits of monosodium urate crystals surrounded by giant cells, epithelioid histiocytes and lymphocytes, which may have a radial needle-like cleft (Fig 1 – blue arrow; Fig 2) or amorphous morphology (Fig 1 – orange arrow; Fig 3 [trichrome]). While the crystals are dissolved during formalin fixation, their birefringence is readily seen on frozen or alcohol-fixed tissue. In addition to the tubulointerstitial changes, the glomeruli may show mesangial sclerosis, thickening of the glomerular basement membranes and segmental subendothelial widening by electron microscopy.](https://pbs.twimg.com/media/GGZ-ZWTWcAAiP7v.jpg)
#TeachingPoints IgG4-related disease is a systemic inflammatory and sclerosing disorder which may affect a wide range of different organs including the pancreas, salivary glands, lacrimal glands, lungs, blood vessels, lymph nodes, thyroid and kidneys among others. Patients may have multisystemic disease at the time of presentation, or different organs may progressively become involved over time. While the renal involvement may have different histopathologic patterns of injury, by far the most common is in the form of acute or chronic tubulointerstitial nephritis (IgG4-related tubulointerstitial nephritis). The renal biopsy shown (Fig 1-4) is from a 35 year old male with history of lymphadenopathy and elevated liver enzymes, who presents with acute pancreatitis and renal insufficiency. A prior liver biopsy showed non-specific plasma cell-rich portal inflammation with frequent eosinophils. The renal biopsy in discussion shows patchy and dense plasma cell-rich interstitial inflammation with frequent eosinophils, which alternates with areas of essentially uninvolved renal parenchyma (Fig 1 and 2). The infiltrate is accentuated around interlobular-sized arteries. Within and surrounding the areas of interstitial inflammation, varying degrees of tubulitis is present. While focal areas show early fibrosis displaying a reticular pattern (Fig 3), the biopsy lacks the characteristic sclerosing pattern seen in more advanced cases. An IgG4 immunoperoxidase stain shows numerous positive plasma cells which well exceed the diagnostic criteria of >10 IgG4+ cells per hpf (Fig 4). Of note, an IgG4+/IgG+ ratio of more than 40% has also been reported as an alternative diagnostic histologic criterion for this disorder; however, an IgG stain was determined to be irrelevant in this case and was not performed. Immunofluorescence shows positive tubular basement membrane granular staining for IgG, kappa and lambda limited to the tubules present within the areas of dense tubulointerstitial inflammation, which is an expected finding in this disorder. Finally, the biopsy shows no evidence of a membranous glomerulopathy, which is another form of renal involvement by IgG4-related disease.




#TeachingPoints This kidney biopsy is from a 16-year-old boy with a history of chronic reflux nephropathy. Imaging findings showed unilateral segmental cortical scarring. Although regions of the biopsy show intact renal cortex with normal appearing glomeruli and tubules (Fig. 1), well demarcated adjacent cortical segments are aglomerular and show severe tubular dropout and interstitial fibrosis (Fig. 2). No definite dysplastic features are noted. This pattern of renal injury supports the clinical impression of unilateral segmental renal hypoplasia (Ask-Upmark kidney). Vesicoureteral reflux is thought to be the main cause of injury in an Ask-Upmark kidney. The condition was first described by the Swedish pathologist Eric Ask-Upmark in 1929.
Reference:
Ask-Upmark E. Uber juvenile maligne Nephrosclerose und ihr Verhaltris zu Storunger in der Nierenentwick-lung . Acta Path Microbiol Scand 1929; 6: 383–44


Last Seen Hashtags on Sotwe
Trends for you
Most Popular Users

Elon Musk 
@elonmusk
240.9M followers

Barack Obama
@barackobama
119.2M followers

Donald J. Trump
@realdonaldtrump
111.8M followers

Cristiano Ronaldo
@cristiano
111.4M followers

Narendra Modi
@narendramodi
107M followers

Rihanna
@rihanna
97.9M followers

NASA
@nasa
92.2M followers

Justin Bieber
@justinbieber
91.1M followers

KATY PERRY
@katyperry
88.1M followers

Taylor Swift
@taylorswift13
82M followers

Lady Gaga
@ladygaga
73.5M followers

Virat Kohli
@imvkohli
70.6M followers

Kim Kardashian
@kimkardashian
70M followers

YouTube
@youtube
68.7M followers

Bill Gates
@billgates
64.1M followers

Neymar Jr
@neymarjr
63.4M followers

The Ellen Show
@theellenshow
62.4M followers

CNN
@cnn
61.9M followers

Selena Gomez
@selenagomez
61.2M followers

X
@x
60.8M followers