D-1 before the World Day 🌍 #WDRAPM#HongKong is hosting a FREE webinar on Central Neuraxial Blocks for the occasion!
⌚ 8am-1pm local time
👉 https://t.co/VylDnjyX4o
Zoom ID: 916 7406 1649
Passcode: 202401
Thank you to Prof M.K. Karmakar for this great initiative 👏
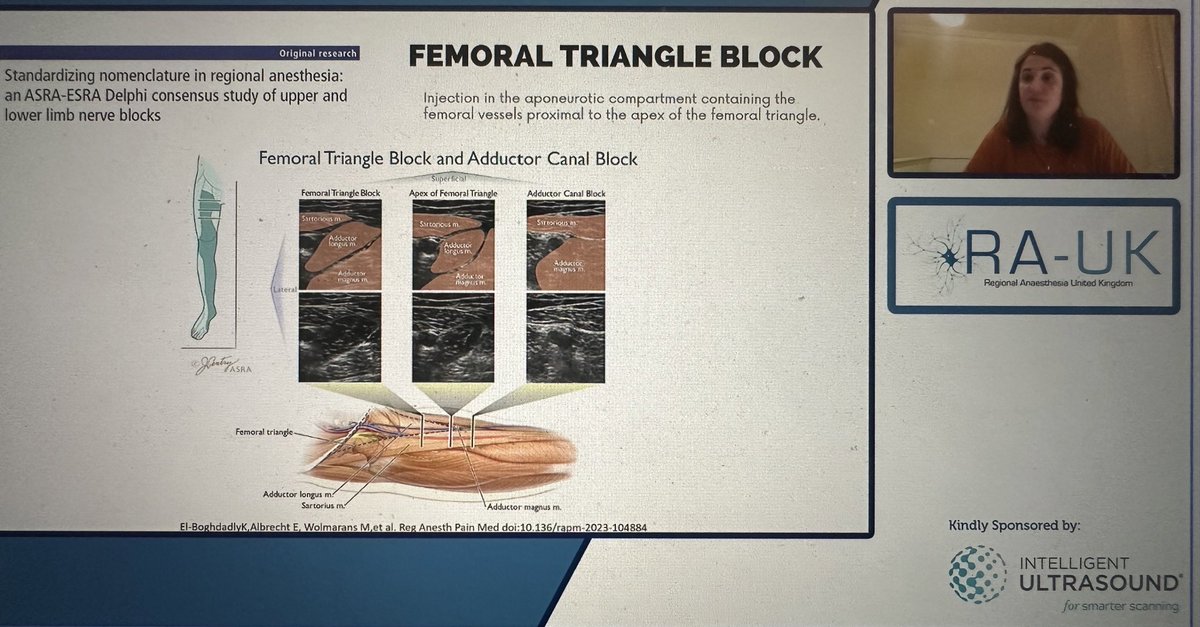
@mariapsebastian reminding us of adductor canal anatomy during @RegionalAnaesUK Plan A webinars
vs femoral triangle (look for pray 🙏🏼 sign)
Does it matter….?
➡️Less likely to block NVM if ACB - unless significant prox spread
➡️Little chance spread to popliteal plexus if FTB
Ultrasound guided genicular nerve blocks non inferior to LIA for TKA
Allows for 20ml of 0.2% of ropivacaine to do the same job as 150ml of 0.2% ropivacaine via LIA
@BlockIt_Hot_Pod@Assoc_Anaes
https://t.co/XvavAGxfpl
Sudden cardiac arrest on the field-of-play is a rare but devastating event.
Our new guidelines have been developed to help save lives across all community and professional sporting events. Read and learn more about Resuscitation on the Field of Play here: https://t.co/AKdMo9Cr0L
Annual Xmas reminder: Just because they’re family doesn’t mean you have to put up with their shite. ‘But BloOd’s tHicKer tHaN wAter.’ …So is custard. What’s your point?
Yes, you share genes. Humans share 60% DNA with a banana. I’m still not inviting a bunch for Xmas dinner.
Belonging at work really matters. Employees with a strong sense of belonging outperform others on almost every metric, from engagement & retention to performance & wellbeing. Good leadership supports belonging: People with an effective manager are 6X more likely to feel this sense of belonging. Six ways to gauge belonging at work based on research:
1) Overall sense of belonging: I feel a strong sense of belonging at my organisation
2) Welcomed: I feel warmly welcomed at in my organisation (first day, new team, new role)
3) Known: I feel known as an individual at work
4) Included: I feel included at work (can be myself, my opinions are valued, can respectfully disagree)
5) Supported: I am supported at work in achieving my personal & professional development goals
6) Connected: I feel a strong connection with peers and colleagues
Download a great free toolkit ("blueprint") for building belonging: https://t.co/omyRE2aFku Thank you @Achievers
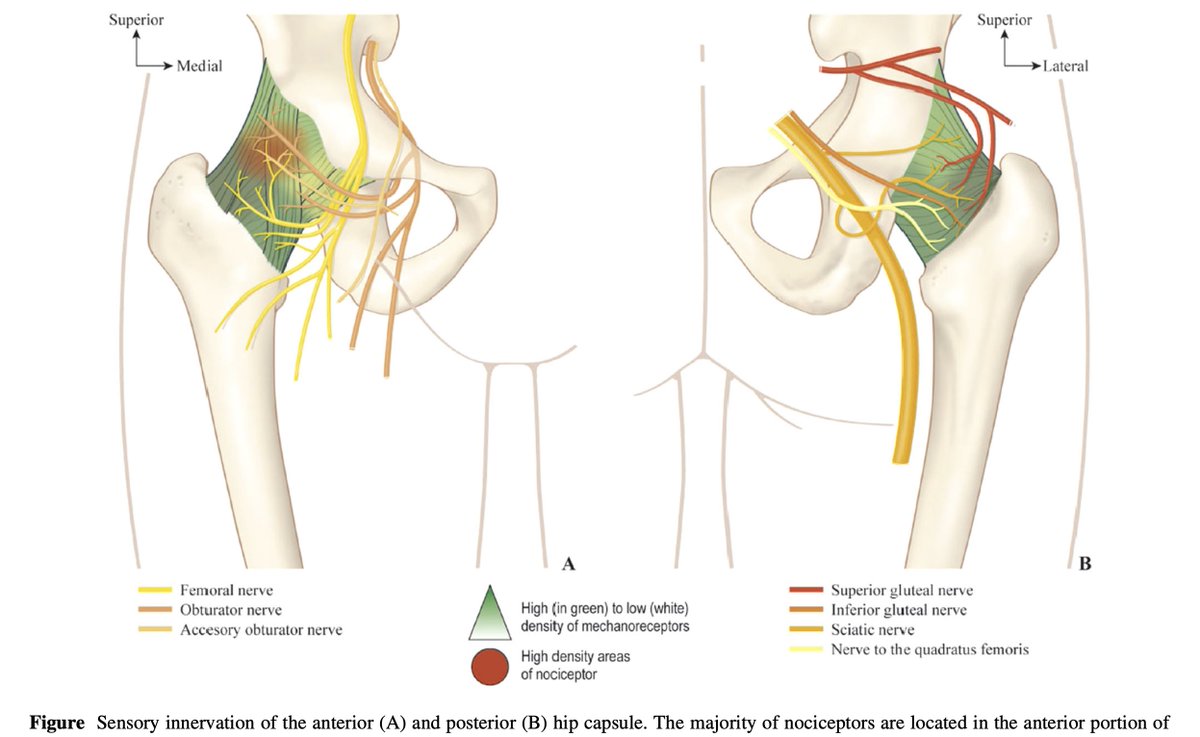
🆕Editorial on barriers and facilitators for peripheral nerve blocks for hip fracture surgery @CJA_Journal
🔗https://t.co/LzHApPd9ax
*⃣Spoilt by choice – which blocks to use and when?
⬇️Understanding the innervation of the hip is crucial
➡️Thanks @RevaRamlogan@camilla_wong
Debate: What causes the therapeutic effect of the erector spinae plane block (ESPB)❓❗
Fascinating new study hypothesizes the key 🔑 to the observed clinical analgesia may be the dorsal root ganglion (DRG), follow the link below to find out more👇
Link: https://t.co/VSliJr8tOA
“RA in Breast Sx: Knowing Targets as per Sx is the Key.”
#RAinBreastSx#BreastSx#PainManagementinBreastSx
My 10 Points:
A. BREAST ANATOMY
1. Modified Sweat gland lying over Pec.Fascia (covering PMM) & separated by Retromammary space.
A small extension of Upper lateral quadrant (Axillary tail of Spence) passes through an opening in Deep fascia (Foramen of Langer).
2. Breast structure:
Skin: Nipple (4th ICS) is pierced by 15-20 lactiferous ducts, having few modified Sweat & Sebaceous glands Rich Ns supply/FNEs. Areola (pigmented skin) Rich in modified sebaceous glands. Enlarged glands during pregnancy/lactation-Raised tubercles of Montgomery. Lactiferous sinuses (where milk is stored) lie below areola.
Parenchyma: Consists of tubulo-alveolar glands that secrete milk. Each gland consists of 15-20 lobes, cluster of alveoli drained by a lactiferrrous duct.
Stroma: Supporting framework -Fibrous+ Fatty. Fibrous stroma forms septa (suspensory ligaments of Cooper), anchoring Skin & gland to the Pec.Fascia.
Fatty stroma forms main bulk distributed all over the breast.
3. Breast innervation:
Cut. supply (Dermatomes) - Cervical plexus(SCN), ICBN(T2), ICNs(T3-T6).
Myofascial supply (Myotomes) - Brachial plexus[MPN (C8-T1), LPN (C5-C7),TDN (C6-C8), LTN (C5-C7)].
Milk Secretion- Controlled by Prolactin.
B. BREAST-CONSERVING SURGERIES (BCS)
4. Lumpectomy, Wide excision, Quadrantectomy, & partial mastectomy. High recurrence rate.
Target Innervation: Involved Dermatome.
RA technique: LIA.
C. NON BCS
5. Simple mastectomy:
Incision: Superiorly till clavicle, Laterally till PMM Lateral border, Medially to sternum, & Inferiorly till inframammary fold.
Excision: Entire subcut breast tissue + overlying skin.
Intact: PMM & its Fascia not disrupted. LN & Muscle.
Target Innervations: ICBN, ACNs, LCNs, & SCN.
RA techniques: EA/PVB + Superficial cervical plexus/Selective SCN Block or LIA.
6. Radical Mastectomy:
Most extensive Sx.
Incision: Superiorly till clavicle, Laterally till anterior margin of LDM, Medially to sternum, and inferiorly till Costal margin.
Excision: Breast tissues, axillary LN, & Pectoral muscles.
Complications: Bad scarring, deformity, reduced shoulder movement, Chronic pain.
Target Innervations: ICBN, ACNs, LCNs, SCN, LPN & MPN.
RA techniques: EA/PVB + Sup CPB/Selective SCNB or LIA, PEC 2, or SAP + PEC 1.
7. Modified Radical Mastectomy:
Incision: Superiorly till clavicle, Laterally till anterior margin of LDM, Medially to sternum, & Inferiorly till Costal margin.
Excision: Breast tissues & axillary LN.
Intact: Pectoral Ms.
Target Innervations: ICBN, ACNs, LCNs, SCN, LPN & MPN.
RA techniques: EA/PVB + Sup. CPB/Selective SCNB or LIA, PEC 2, or SAP + PEC 1.
D. COSMETIC BREAST Sx
8. Breast Augmentation Sx:
Incisions: Peri-areolar, Inframammary, Trans-axillary, or Trans-umbilical.
Surgery: Involves pocket formation disrupting pectoral Ms.
Reduction Mammoplasty. Breast-Lift Sx (Mastopexy).
Target innervations & RA techniques: As per approaches.
9. Reconstructive Mammoplasty:
LD Myocutaneous flap, Transversus Rectus Abdominis Myocutaneous (TRAM) flap.
Surgery: Implants are placed between PMM-PMnM & laterally elevating SAM.
Target innervations: Pectoral Ns. (MPN & LPN), LCBs of ICNs, LTN, and TDN (if LD flap is used).
RA technique: EA/PVB + Sup.CPB/Selective SCNB or LIA, PEC 2, SAP + PEC 1, RSB/TAP (for TRAM).
E. RA OPTIONS
10. For Anesthesia:Thoracic EA (Bilateral Sx), Thoracic PVB (Unilateral Sx) +/- LIA/SCNB.
For Analgesia:LIA (for BCS), PEC 2(Non-BCS), SAP+PEC 1 or PEC (Non-BCS with axillary clearance).
Surgical Perspective:
Large LA volume can affect surgical dissection & electrical cautery function. Sometimes, use neurostimulation to identify & preserve LTN - Ineffective with LA solution.
Anesthesia Perspective: Optimal analgesia, reduced GA drug req./opioid consumption,Clear surgical field,reduced Stress response (Symp. block),& Avoids chronic pain.























![KartikBSonawane's tweet photo. “RA in Breast Sx: Knowing Targets as per Sx is the Key.”
#RAinBreastSx
#BreastSx
#PainManagementinBreastSx
My 10 Points:
A. BREAST ANATOMY
1. Modified Sweat gland lying over Pec.Fascia (covering PMM) & separated by Retromammary space.
A small extension of Upper lateral quadrant (Axillary tail of Spence) passes through an opening in Deep fascia (Foramen of Langer).
2. Breast structure:
Skin: Nipple (4th ICS) is pierced by 15-20 lactiferous ducts, having few modified Sweat & Sebaceous glands Rich Ns supply/FNEs. Areola (pigmented skin) Rich in modified sebaceous glands. Enlarged glands during pregnancy/lactation-Raised tubercles of Montgomery. Lactiferous sinuses (where milk is stored) lie below areola.
Parenchyma: Consists of tubulo-alveolar glands that secrete milk. Each gland consists of 15-20 lobes, cluster of alveoli drained by a lactiferrrous duct.
Stroma: Supporting framework -Fibrous+ Fatty. Fibrous stroma forms septa (suspensory ligaments of Cooper), anchoring Skin & gland to the Pec.Fascia.
Fatty stroma forms main bulk distributed all over the breast.
3. Breast innervation:
Cut. supply (Dermatomes) - Cervical plexus(SCN), ICBN(T2), ICNs(T3-T6).
Myofascial supply (Myotomes) - Brachial plexus[MPN (C8-T1), LPN (C5-C7),TDN (C6-C8), LTN (C5-C7)].
Milk Secretion- Controlled by Prolactin.
B. BREAST-CONSERVING SURGERIES (BCS)
4. Lumpectomy, Wide excision, Quadrantectomy, & partial mastectomy. High recurrence rate.
Target Innervation: Involved Dermatome.
RA technique: LIA.
C. NON BCS
5. Simple mastectomy:
Incision: Superiorly till clavicle, Laterally till PMM Lateral border, Medially to sternum, & Inferiorly till inframammary fold.
Excision: Entire subcut breast tissue + overlying skin.
Intact: PMM & its Fascia not disrupted. LN & Muscle.
Target Innervations: ICBN, ACNs, LCNs, & SCN.
RA techniques: EA/PVB + Superficial cervical plexus/Selective SCN Block or LIA.
6. Radical Mastectomy:
Most extensive Sx.
Incision: Superiorly till clavicle, Laterally till anterior margin of LDM, Medially to sternum, and inferiorly till Costal margin.
Excision: Breast tissues, axillary LN, & Pectoral muscles.
Complications: Bad scarring, deformity, reduced shoulder movement, Chronic pain.
Target Innervations: ICBN, ACNs, LCNs, SCN, LPN & MPN.
RA techniques: EA/PVB + Sup CPB/Selective SCNB or LIA, PEC 2, or SAP + PEC 1.
7. Modified Radical Mastectomy:
Incision: Superiorly till clavicle, Laterally till anterior margin of LDM, Medially to sternum, & Inferiorly till Costal margin.
Excision: Breast tissues & axillary LN.
Intact: Pectoral Ms.
Target Innervations: ICBN, ACNs, LCNs, SCN, LPN & MPN.
RA techniques: EA/PVB + Sup. CPB/Selective SCNB or LIA, PEC 2, or SAP + PEC 1.
D. COSMETIC BREAST Sx
8. Breast Augmentation Sx:
Incisions: Peri-areolar, Inframammary, Trans-axillary, or Trans-umbilical.
Surgery: Involves pocket formation disrupting pectoral Ms.
Reduction Mammoplasty. Breast-Lift Sx (Mastopexy).
Target innervations & RA techniques: As per approaches.
9. Reconstructive Mammoplasty:
LD Myocutaneous flap, Transversus Rectus Abdominis Myocutaneous (TRAM) flap.
Surgery: Implants are placed between PMM-PMnM & laterally elevating SAM.
Target innervations: Pectoral Ns. (MPN & LPN), LCBs of ICNs, LTN, and TDN (if LD flap is used).
RA technique: EA/PVB + Sup.CPB/Selective SCNB or LIA, PEC 2, SAP + PEC 1, RSB/TAP (for TRAM).
E. RA OPTIONS
10. For Anesthesia:Thoracic EA (Bilateral Sx), Thoracic PVB (Unilateral Sx) +/- LIA/SCNB.
For Analgesia:LIA (for BCS), PEC 2(Non-BCS), SAP+PEC 1 or PEC (Non-BCS with axillary clearance).
Surgical Perspective:
Large LA volume can affect surgical dissection & electrical cautery function. Sometimes, use neurostimulation to identify & preserve LTN - Ineffective with LA solution.
Anesthesia Perspective: Optimal analgesia, reduced GA drug req./opioid consumption,Clear surgical field,reduced Stress response (Symp. block),& Avoids chronic pain.](https://pbs.twimg.com/media/GA9Y-bxawAA_1Kk.jpg)
![KartikBSonawane's tweet photo. “RA in Breast Sx: Knowing Targets as per Sx is the Key.”
#RAinBreastSx
#BreastSx
#PainManagementinBreastSx
My 10 Points:
A. BREAST ANATOMY
1. Modified Sweat gland lying over Pec.Fascia (covering PMM) & separated by Retromammary space.
A small extension of Upper lateral quadrant (Axillary tail of Spence) passes through an opening in Deep fascia (Foramen of Langer).
2. Breast structure:
Skin: Nipple (4th ICS) is pierced by 15-20 lactiferous ducts, having few modified Sweat & Sebaceous glands Rich Ns supply/FNEs. Areola (pigmented skin) Rich in modified sebaceous glands. Enlarged glands during pregnancy/lactation-Raised tubercles of Montgomery. Lactiferous sinuses (where milk is stored) lie below areola.
Parenchyma: Consists of tubulo-alveolar glands that secrete milk. Each gland consists of 15-20 lobes, cluster of alveoli drained by a lactiferrrous duct.
Stroma: Supporting framework -Fibrous+ Fatty. Fibrous stroma forms septa (suspensory ligaments of Cooper), anchoring Skin & gland to the Pec.Fascia.
Fatty stroma forms main bulk distributed all over the breast.
3. Breast innervation:
Cut. supply (Dermatomes) - Cervical plexus(SCN), ICBN(T2), ICNs(T3-T6).
Myofascial supply (Myotomes) - Brachial plexus[MPN (C8-T1), LPN (C5-C7),TDN (C6-C8), LTN (C5-C7)].
Milk Secretion- Controlled by Prolactin.
B. BREAST-CONSERVING SURGERIES (BCS)
4. Lumpectomy, Wide excision, Quadrantectomy, & partial mastectomy. High recurrence rate.
Target Innervation: Involved Dermatome.
RA technique: LIA.
C. NON BCS
5. Simple mastectomy:
Incision: Superiorly till clavicle, Laterally till PMM Lateral border, Medially to sternum, & Inferiorly till inframammary fold.
Excision: Entire subcut breast tissue + overlying skin.
Intact: PMM & its Fascia not disrupted. LN & Muscle.
Target Innervations: ICBN, ACNs, LCNs, & SCN.
RA techniques: EA/PVB + Superficial cervical plexus/Selective SCN Block or LIA.
6. Radical Mastectomy:
Most extensive Sx.
Incision: Superiorly till clavicle, Laterally till anterior margin of LDM, Medially to sternum, and inferiorly till Costal margin.
Excision: Breast tissues, axillary LN, & Pectoral muscles.
Complications: Bad scarring, deformity, reduced shoulder movement, Chronic pain.
Target Innervations: ICBN, ACNs, LCNs, SCN, LPN & MPN.
RA techniques: EA/PVB + Sup CPB/Selective SCNB or LIA, PEC 2, or SAP + PEC 1.
7. Modified Radical Mastectomy:
Incision: Superiorly till clavicle, Laterally till anterior margin of LDM, Medially to sternum, & Inferiorly till Costal margin.
Excision: Breast tissues & axillary LN.
Intact: Pectoral Ms.
Target Innervations: ICBN, ACNs, LCNs, SCN, LPN & MPN.
RA techniques: EA/PVB + Sup. CPB/Selective SCNB or LIA, PEC 2, or SAP + PEC 1.
D. COSMETIC BREAST Sx
8. Breast Augmentation Sx:
Incisions: Peri-areolar, Inframammary, Trans-axillary, or Trans-umbilical.
Surgery: Involves pocket formation disrupting pectoral Ms.
Reduction Mammoplasty. Breast-Lift Sx (Mastopexy).
Target innervations & RA techniques: As per approaches.
9. Reconstructive Mammoplasty:
LD Myocutaneous flap, Transversus Rectus Abdominis Myocutaneous (TRAM) flap.
Surgery: Implants are placed between PMM-PMnM & laterally elevating SAM.
Target innervations: Pectoral Ns. (MPN & LPN), LCBs of ICNs, LTN, and TDN (if LD flap is used).
RA technique: EA/PVB + Sup.CPB/Selective SCNB or LIA, PEC 2, SAP + PEC 1, RSB/TAP (for TRAM).
E. RA OPTIONS
10. For Anesthesia:Thoracic EA (Bilateral Sx), Thoracic PVB (Unilateral Sx) +/- LIA/SCNB.
For Analgesia:LIA (for BCS), PEC 2(Non-BCS), SAP+PEC 1 or PEC (Non-BCS with axillary clearance).
Surgical Perspective:
Large LA volume can affect surgical dissection & electrical cautery function. Sometimes, use neurostimulation to identify & preserve LTN - Ineffective with LA solution.
Anesthesia Perspective: Optimal analgesia, reduced GA drug req./opioid consumption,Clear surgical field,reduced Stress response (Symp. block),& Avoids chronic pain.](https://pbs.twimg.com/media/GA9Y-F2bAAA83OT.jpg)
![KartikBSonawane's tweet photo. “RA in Breast Sx: Knowing Targets as per Sx is the Key.”
#RAinBreastSx
#BreastSx
#PainManagementinBreastSx
My 10 Points:
A. BREAST ANATOMY
1. Modified Sweat gland lying over Pec.Fascia (covering PMM) & separated by Retromammary space.
A small extension of Upper lateral quadrant (Axillary tail of Spence) passes through an opening in Deep fascia (Foramen of Langer).
2. Breast structure:
Skin: Nipple (4th ICS) is pierced by 15-20 lactiferous ducts, having few modified Sweat & Sebaceous glands Rich Ns supply/FNEs. Areola (pigmented skin) Rich in modified sebaceous glands. Enlarged glands during pregnancy/lactation-Raised tubercles of Montgomery. Lactiferous sinuses (where milk is stored) lie below areola.
Parenchyma: Consists of tubulo-alveolar glands that secrete milk. Each gland consists of 15-20 lobes, cluster of alveoli drained by a lactiferrrous duct.
Stroma: Supporting framework -Fibrous+ Fatty. Fibrous stroma forms septa (suspensory ligaments of Cooper), anchoring Skin & gland to the Pec.Fascia.
Fatty stroma forms main bulk distributed all over the breast.
3. Breast innervation:
Cut. supply (Dermatomes) - Cervical plexus(SCN), ICBN(T2), ICNs(T3-T6).
Myofascial supply (Myotomes) - Brachial plexus[MPN (C8-T1), LPN (C5-C7),TDN (C6-C8), LTN (C5-C7)].
Milk Secretion- Controlled by Prolactin.
B. BREAST-CONSERVING SURGERIES (BCS)
4. Lumpectomy, Wide excision, Quadrantectomy, & partial mastectomy. High recurrence rate.
Target Innervation: Involved Dermatome.
RA technique: LIA.
C. NON BCS
5. Simple mastectomy:
Incision: Superiorly till clavicle, Laterally till PMM Lateral border, Medially to sternum, & Inferiorly till inframammary fold.
Excision: Entire subcut breast tissue + overlying skin.
Intact: PMM & its Fascia not disrupted. LN & Muscle.
Target Innervations: ICBN, ACNs, LCNs, & SCN.
RA techniques: EA/PVB + Superficial cervical plexus/Selective SCN Block or LIA.
6. Radical Mastectomy:
Most extensive Sx.
Incision: Superiorly till clavicle, Laterally till anterior margin of LDM, Medially to sternum, and inferiorly till Costal margin.
Excision: Breast tissues, axillary LN, & Pectoral muscles.
Complications: Bad scarring, deformity, reduced shoulder movement, Chronic pain.
Target Innervations: ICBN, ACNs, LCNs, SCN, LPN & MPN.
RA techniques: EA/PVB + Sup CPB/Selective SCNB or LIA, PEC 2, or SAP + PEC 1.
7. Modified Radical Mastectomy:
Incision: Superiorly till clavicle, Laterally till anterior margin of LDM, Medially to sternum, & Inferiorly till Costal margin.
Excision: Breast tissues & axillary LN.
Intact: Pectoral Ms.
Target Innervations: ICBN, ACNs, LCNs, SCN, LPN & MPN.
RA techniques: EA/PVB + Sup. CPB/Selective SCNB or LIA, PEC 2, or SAP + PEC 1.
D. COSMETIC BREAST Sx
8. Breast Augmentation Sx:
Incisions: Peri-areolar, Inframammary, Trans-axillary, or Trans-umbilical.
Surgery: Involves pocket formation disrupting pectoral Ms.
Reduction Mammoplasty. Breast-Lift Sx (Mastopexy).
Target innervations & RA techniques: As per approaches.
9. Reconstructive Mammoplasty:
LD Myocutaneous flap, Transversus Rectus Abdominis Myocutaneous (TRAM) flap.
Surgery: Implants are placed between PMM-PMnM & laterally elevating SAM.
Target innervations: Pectoral Ns. (MPN & LPN), LCBs of ICNs, LTN, and TDN (if LD flap is used).
RA technique: EA/PVB + Sup.CPB/Selective SCNB or LIA, PEC 2, SAP + PEC 1, RSB/TAP (for TRAM).
E. RA OPTIONS
10. For Anesthesia:Thoracic EA (Bilateral Sx), Thoracic PVB (Unilateral Sx) +/- LIA/SCNB.
For Analgesia:LIA (for BCS), PEC 2(Non-BCS), SAP+PEC 1 or PEC (Non-BCS with axillary clearance).
Surgical Perspective:
Large LA volume can affect surgical dissection & electrical cautery function. Sometimes, use neurostimulation to identify & preserve LTN - Ineffective with LA solution.
Anesthesia Perspective: Optimal analgesia, reduced GA drug req./opioid consumption,Clear surgical field,reduced Stress response (Symp. block),& Avoids chronic pain.](https://pbs.twimg.com/media/GA9Y9v4b0AAs00O.jpg)





















![KartikBSonawane's tweet photo. “RA in Breast Sx: Knowing Targets as per Sx is the Key.”
#RAinBreastSx
#BreastSx
#PainManagementinBreastSx
My 10 Points:
A. BREAST ANATOMY
1. Modified Sweat gland lying over Pec.Fascia (covering PMM) & separated by Retromammary space.
A small extension of Upper lateral quadrant (Axillary tail of Spence) passes through an opening in Deep fascia (Foramen of Langer).
2. Breast structure:
Skin: Nipple (4th ICS) is pierced by 15-20 lactiferous ducts, having few modified Sweat & Sebaceous glands Rich Ns supply/FNEs. Areola (pigmented skin) Rich in modified sebaceous glands. Enlarged glands during pregnancy/lactation-Raised tubercles of Montgomery. Lactiferous sinuses (where milk is stored) lie below areola.
Parenchyma: Consists of tubulo-alveolar glands that secrete milk. Each gland consists of 15-20 lobes, cluster of alveoli drained by a lactiferrrous duct.
Stroma: Supporting framework -Fibrous+ Fatty. Fibrous stroma forms septa (suspensory ligaments of Cooper), anchoring Skin & gland to the Pec.Fascia.
Fatty stroma forms main bulk distributed all over the breast.
3. Breast innervation:
Cut. supply (Dermatomes) - Cervical plexus(SCN), ICBN(T2), ICNs(T3-T6).
Myofascial supply (Myotomes) - Brachial plexus[MPN (C8-T1), LPN (C5-C7),TDN (C6-C8), LTN (C5-C7)].
Milk Secretion- Controlled by Prolactin.
B. BREAST-CONSERVING SURGERIES (BCS)
4. Lumpectomy, Wide excision, Quadrantectomy, & partial mastectomy. High recurrence rate.
Target Innervation: Involved Dermatome.
RA technique: LIA.
C. NON BCS
5. Simple mastectomy:
Incision: Superiorly till clavicle, Laterally till PMM Lateral border, Medially to sternum, & Inferiorly till inframammary fold.
Excision: Entire subcut breast tissue + overlying skin.
Intact: PMM & its Fascia not disrupted. LN & Muscle.
Target Innervations: ICBN, ACNs, LCNs, & SCN.
RA techniques: EA/PVB + Superficial cervical plexus/Selective SCN Block or LIA.
6. Radical Mastectomy:
Most extensive Sx.
Incision: Superiorly till clavicle, Laterally till anterior margin of LDM, Medially to sternum, and inferiorly till Costal margin.
Excision: Breast tissues, axillary LN, & Pectoral muscles.
Complications: Bad scarring, deformity, reduced shoulder movement, Chronic pain.
Target Innervations: ICBN, ACNs, LCNs, SCN, LPN & MPN.
RA techniques: EA/PVB + Sup CPB/Selective SCNB or LIA, PEC 2, or SAP + PEC 1.
7. Modified Radical Mastectomy:
Incision: Superiorly till clavicle, Laterally till anterior margin of LDM, Medially to sternum, & Inferiorly till Costal margin.
Excision: Breast tissues & axillary LN.
Intact: Pectoral Ms.
Target Innervations: ICBN, ACNs, LCNs, SCN, LPN & MPN.
RA techniques: EA/PVB + Sup. CPB/Selective SCNB or LIA, PEC 2, or SAP + PEC 1.
D. COSMETIC BREAST Sx
8. Breast Augmentation Sx:
Incisions: Peri-areolar, Inframammary, Trans-axillary, or Trans-umbilical.
Surgery: Involves pocket formation disrupting pectoral Ms.
Reduction Mammoplasty. Breast-Lift Sx (Mastopexy).
Target innervations & RA techniques: As per approaches.
9. Reconstructive Mammoplasty:
LD Myocutaneous flap, Transversus Rectus Abdominis Myocutaneous (TRAM) flap.
Surgery: Implants are placed between PMM-PMnM & laterally elevating SAM.
Target innervations: Pectoral Ns. (MPN & LPN), LCBs of ICNs, LTN, and TDN (if LD flap is used).
RA technique: EA/PVB + Sup.CPB/Selective SCNB or LIA, PEC 2, SAP + PEC 1, RSB/TAP (for TRAM).
E. RA OPTIONS
10. For Anesthesia:Thoracic EA (Bilateral Sx), Thoracic PVB (Unilateral Sx) +/- LIA/SCNB.
For Analgesia:LIA (for BCS), PEC 2(Non-BCS), SAP+PEC 1 or PEC (Non-BCS with axillary clearance).
Surgical Perspective:
Large LA volume can affect surgical dissection & electrical cautery function. Sometimes, use neurostimulation to identify & preserve LTN - Ineffective with LA solution.
Anesthesia Perspective: Optimal analgesia, reduced GA drug req./opioid consumption,Clear surgical field,reduced Stress response (Symp. block),& Avoids chronic pain.](https://pbs.twimg.com/media/GA9Y-uXa4AASt32.jpg)




















