I would like to reflect on this one. In ACS the guidelines suggest the use of IV enoxaparin as bolus. There are two different scenarios in case if the patient is going towards PCI:
1. Previously treated patients with enoxaparin: If a patient has received a subcutanous dose of
2. LMWH = Low Molecular Weight Heparin
Brands we use: Enoxaparin = Clexane 40mg, 60mg. Dalteparin = Fragmin. Tinzaparin
Mechanism: Mainly blocks Factor Xa
When we use it:
- DVT/PE treatment → 1mg/kg SC BD
- DVT prophylaxis → 40mg SC OD for bedridden, post-op patients
- Pregnancy → Drug of choice. Safe in pregnancy
- NSTEMI → 1mg/kg SC BD
Route: SC only. Never IV, Never IM
Half life: 4-6 hours
Monitoring: Usually NO monitoring needed. Only check Anti-Xa if pregnancy or renal failure
Antidote: Protamine → only 60% reversal
Downside: Don’t use in severe kidney disease.
Similarly, with fibrinolytic therapy; if the age is <75 y, 30 mg IV bolus followed in 15 min by 1 mg/kg SC BID.
If the age is >75 y no bolus dose is needed. But 0.75 mg/kg SC BID is needed.
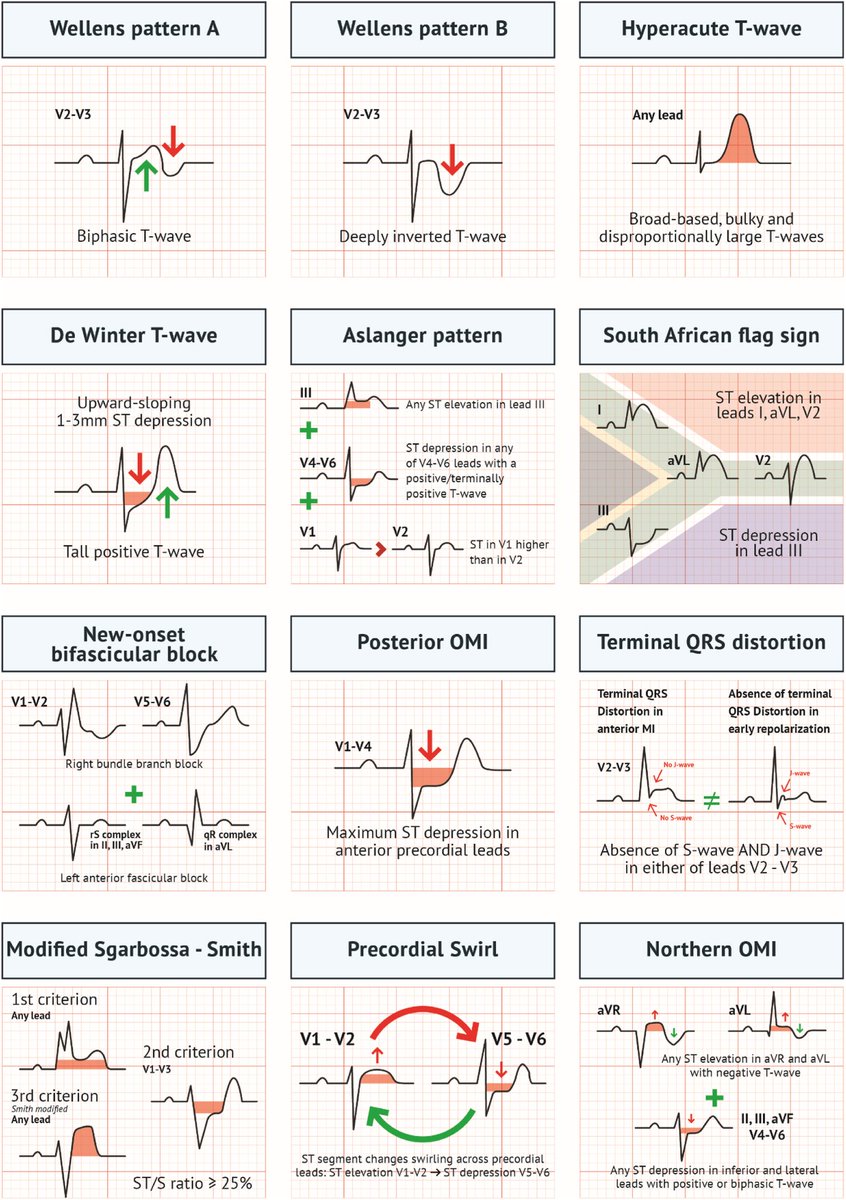
Acute MI is not always STEMI.
A major 2025 review highlights why relying only on classic STEMI criteria can miss dangerous coronary occlusions.
A thread on OMI (Occlusion Myocardial Infarction): 🧵
𝗙𝗲𝗺𝗮𝗹𝗲 𝗗𝗼𝗰𝘁𝗼𝗿 𝗶𝗻𝘀𝘂𝗹𝘁𝗲𝗱 𝗯𝘆 𝗮 𝗕𝘂𝗿𝗲𝗮𝘂𝗰𝗿𝗮𝘁:
This video has two parts, and together they explain why so many doctors choose to leave Pakistan.
Part 1 allegedly shows an ACP in Burewala, Punjab misbehaving with an on duty female doctor inside a hospital. Reportedly, she was being questioned about not ordering a CT scan, something that according to our understanding could only be ordered by a consultant, which she was not.
What stood out even more was the arrogance, tone, and public humiliation. Calling an on duty female physician “Bibi” instead of “Dr Sahiba,” recording inside a crowded hospital with a mic attached, posturing like an interrogation officer, while patients stood nearby, is deeply inappropriate. It raises serious concerns about patient privacy, disruption of care, and abuse of authority.
Unfortunately, this happens because many powerful officials in Pakistan, especially bureaucrats, behave as if they are above the law. In most civilized countries, such conduct by a government officer inside a hospital would likely end careers.
Part 2 shows the complete opposite. In 2011, a senior surgeon at Guy's Hospital publicly confronted then UK Prime Minister David Cameron and Deputy PM Nick Clegg for violating hospital hygiene rules during a photo opportunity.
The surgeon spoke up despite their power because patient safety and professional standards came first. That is what happens in systems where doctors are respected and authority is held accountable.
Compare these two incidents carefully, and you will understand that doctors do not leave Pakistan only for money. They leave for dignity, professional respect, safety, and integrity.
#doctorsinpakistan #burewala #punjabgovernment #mbbs
The American Heart Association mourns the passing of the legendary cardiologist Eugene Braunwald, M.D., widely recognized as one of the most influential figures in the history of cardiovascular medicine. Over seven decades, his work reshaped the understanding and treatment of heart disease, leading many to call him the father of modern cardiology.
Braunwald was a lifelong contributor to the American Heart Association, helping advance its research and scientific mission, and was honored with some of the Association’s highest honors for his lasting influence on cardiovascular care and research. His influence extended well beyond his own discoveries, as generations of Association‑supported investigators, clinicians and academic leaders were trained by Braunwald or guided by the clinical trial standards and mentorship models he helped establish.
https://t.co/ieZuHYMyOP
Big RCA tumor blush in a suspected atrial myxoma
Even a “simple” coronary angiogram can reveal amazing images 🤩💯
See something interesting? Share it 🫡
#CardioTwitter#CathLab#Radial
The guy they chose to deliver the lines of the racist Tandoor joke looks every bit as deranged as the joke itself.
And PMLN’s disgraceful media cell headed by Atta Tarar needs to realise that the kind of racist & utterly brainless politics they are peddling belonged in the 80s and 90s and has rotted now. Nobody is impressed & absolutely nobody is laughing.
Pull your heads out of the gutter because this is embarrassing & totally unbearable.
This is so incredibly dangerous and will be seen by millions of people.
I'm a cardiologist who opens the arteries of people with heart attacks.
1. Secondary vs primary prevention - Here, Malhotra is talking about someone taking a statin who has *already had a heart attack*.
First of all, if you survive a heart attack without any major damage, you're lucky. A lot of people aren't as lucky. I know this because I do this work for a living.
Primary prevention is for people who've never had any clinical event. If you've had a heart attack, you are NOT THE SAME as someone your same age, etc who has NOT had one. The game is changed and much riskier for you. You are at a HIGHER RISK of ANOTHER heart attack. You need to be MORE AGGRESSIVE to lower that risk. If your first one spared your life, the second one might not. That is secondary prevention.
2. "Benefit over 5 years" - This is such a classic, silly misinformation trick. OK sure - but that assumes you're only planning on living another 5 years and then are ok with just dying.
That's obviously absurd and I don't believe anyone agrees with that. As your cardiologist, I'm not trying to keep you alive and well for just 5 years. I'm talking 10, 20, 30 years, decades.
The real true benefit of statin therapy is over decades. As in, they help keep you alive longer. You can't just measure it at an arbitrary 5 year cut off.
3. Not magic bullet - Prevention is not just statins. It is changing your entire lifestyle, diet, exercise, etc, and meds. Statins are not magic either. People on statins have heart attacks too.
But life is about risks and probabilities. You do what you can to reduce risk as much as possible. You cannot reduce risk to 0, but you can bring it pretty damn close to 0.
It is so fascinating to me that there are so many highly intelligent and accomplished people who have an intimate understanding of risk and probabilities, and who make major decisions in their daily lives based on this understanding. But when it comes to statins and vaccines, they just abandon all logic.
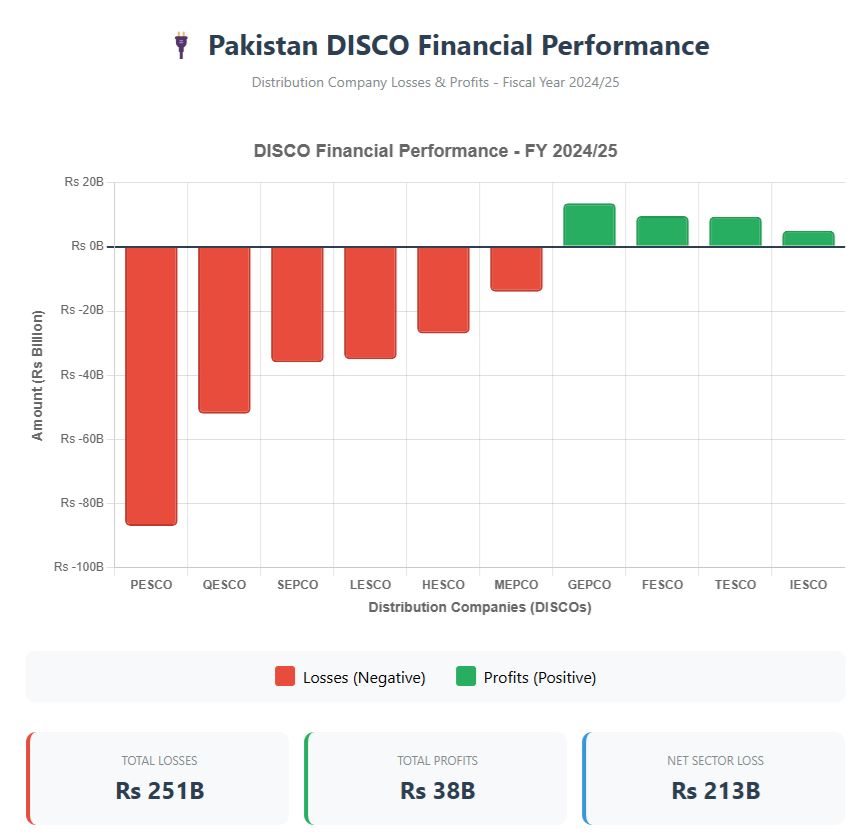
They're robbing us in broad daylight and calling it "policy."
Pakistan's salaried class paid Rs. 600 BILLION in taxes last year.
Electricity companies lost Rs. 213 BILLION.
Do the math—1/3rd of YOUR salary tax is going straight into covering these losses.
And what happened when people tried to escape this mess by installing solar panels? The government slashed net metering benefits. Because why let people find solutions when you can just squeeze more money out of them, right?
Here's what nobody's asking: Why aren't these losses being fixed?
Why is it always easier to tax the struggling middle class than to hold inefficient institutions accountable?
We work hard. We pay our taxes. We deserve a system that works FOR us, not AGAINST us.
It's time to demand better. Share if you agree. 📷
I was on duty that day, a final-year medicine trainee.
A call came from orthopedics.
“45-year-old man, fall from bike — fracture left distal radius, rib fracture on right side. Now complaining of left-sided chest pain.”
They’d given him diclofenac for pain.
Pain had improved… but 30 minutes later, he started clutching his chest.
“Probably rib pain,” they thought.
But the rib fracture was on the right side.
He kept insisting —
“Doctor, this pain is on the left… and it’s getting worse.”
So they called me.
When I reached, he was in visible distress — sweating, anxious, restless.
No addictions. No comorbidities. No prior drug allergy.
He said, “Initially my pain was in the right chest and left forearm… now it’s heaviness on the left side of my chest.”
The X-ray had ruled out any left rib fracture.
No local tenderness.
Something didn’t add up.
I asked him to describe the pain.
He said quietly,
“Feels like someone’s sitting on my chest.”
He was nauseated, sweating more.
While talking, I noticed something else — red rashes scattered across his abdomen and thighs.
They looked fresh.
“When did this start?”
He thought for a second.
“About 45 minutes ago.”
I checked his drug chart — IM diclofenac for pain.
I looked at the rash again, then at his face turning pale.
The timing fit perfectly.
My orthopedic colleague asked,
“What are you thinking?”
I said, “Let’s get an ECG — now.”
He replied, “We already have one, it was normal for pre-op.”
Still, we repeated it.
And that changed everything.
ST elevation — V1 to V4.
Troponin and CK-MB both high.
Acute coronary syndrome.
We gave a loading dose, sublingual nitrate.
His BP was 150/80.
I added verapamil.
He started feeling better.
We repeated the ECG after an hour —
the ST elevation had vanished.
My colleague asked, “Why verapamil?”
I just smiled.
Because this wasn’t atherosclerosis.
This was an allergy of the heart.
That night, I met Kounis Syndrome —
an allergic storm that spasms the coronaries.
Triggered by a painkiller.
A paradox —
the drug meant to relieve pain had almost broken a heart.
In the following months, I saw two more.
One after penicillin.
One after a bee sting.
Each time, I remembered that man.
And his quiet, unforgettable line —
“Doctor… the pain has shifted to the wrong side.”
Medicine teaches you to treat what you see.
Experience teaches you to question what you don’t.
Sometimes, the clue isn’t in the test —
it’s hidden in the timeline.
In a rash. A word. A hesitation.
That’s where the diagnosis lives.
🩺 #MedTwitter #KounisSyndrome #StorytellingInMedicine #Allergy #Cardiology #Rheumatology #Immunology
#Sullysrounds #MedX #Medtwitter #Mnemonics #Medicine #History
@DrAkhilX @IhabFathiSulima@Janetbirdope #MedTwitter #RheumTwitter
@CelestinoGutirr@aditya_gan3500@nileshnolkha@nirmalregency
This is NOT the first genocide that happens under "our" watch. It is the first genocide that WE, The People, can and will stop.
Against all odds and adversities.
@otherbarak Well, just because you are looking at one healthy man, it does not by any means mean that there's no starvation in Gaza. The only way to confirm what's really happening is if the IDF allow international media inside Gaza. Which I'm sure you guys will never ever do.