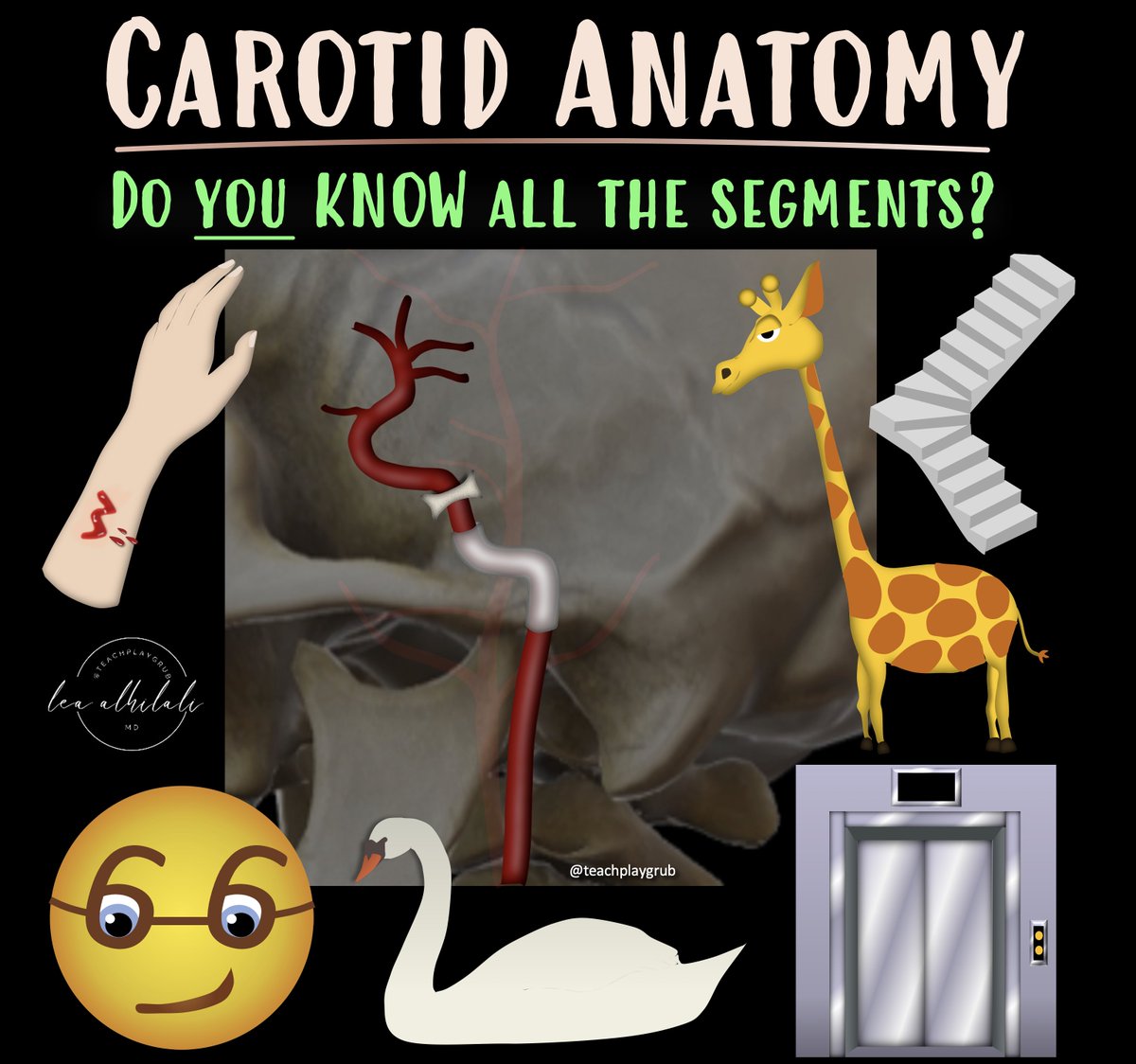
1/Time to go with the flow!
Hoping no one notices you don’t know the anatomy of internal carotid (ICA)?
Do you say “carotid siphon” & hope no one asks for more detail?
Here’s a thread to help you siphon off some information about ICA anatomy!
The 90s called & wants its carotid imaging back!
It’s been 30 years--are you still on NASCET?
Feeling vulnerable about plaque vulnerability?
This month’s @theAJNR SCANtastic has what you need to know about carotid plaque
https://t.co/5tTqrJr2mS
Carotid disease not only harms by stenosis but also by serving as a source of emboli.
We can use carotid plaque-RADS, which has been adapted for CTA to identify high-risk plaques!
Type 1 = no plaque.
--Remember bc the number 1 looks like a smooth straight vessel with no plaque!
Type 2 = plaque thickness < 3mm & no signs of vulnerability (ulceration)
--Remember this bc 2 is < 3 & the curve of the number 2 mimics a smooth, non-ulcerated plaque.
Type 3 = plaque thickness >3mm or ulceration
--Remember 3 is greater than 3! And the scooped out part of the number 3 looks like scooped out ulceration!
Type 4 = plaque hemorrhage or intraluminal thrombus
--Remember pointy part of the number 4 looks like pointy thrombus pointing into the lumen
--Remember also the number four has a hole in the middle—just like the hole blasted in a plaque by intraplaque hemorrhage!
In this month’s @theAJNR, Saba et al. found that this scoring system was highly reproducible among intermediate & experienced readers.
But like all things radiology—there was a learning curve for inexperienced readers.
So go beyond NASCET!
Hopefully, now you’ll never feel vulnerable about vulnerable carotid plaque!
Follow @theAJNR and check it out for yourself:
https://t.co/5tTqrJr2mS
If you aren’t cheating, you aren’t trying!
Are you looking at MRIs?
Feeling some confusion about the diffusion?
Feel impaired when it comes to the FLAIR?
Wish you could cheat a little?
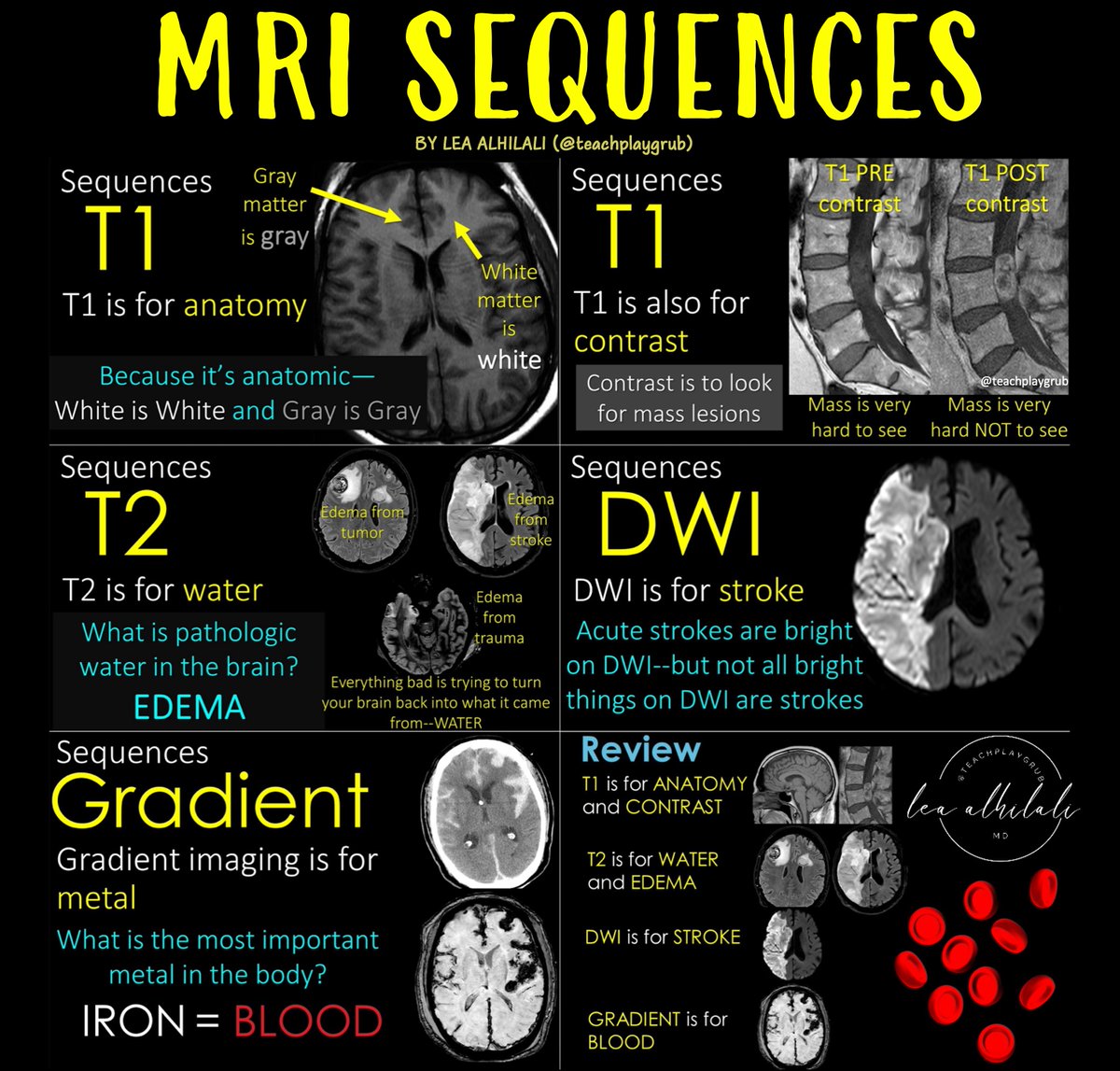
Here’s a post to help you cheat on all the sequences you NEED to know if you are looking at MRIs!
--T1: It’s for anatomy, so brain structures reflect the same color as real life. So gray matter is gray on T1 & white matter is white on T1. It’s also for contrast. Contrast material is taken up by masses making them light up & them easier to see.
--T2: It’s the water sensitive sequence. What is pathologic water in the brain? Edema! My attending once said, “Everything bad in this world is trying to turn you back into what you came from—water."
-- DWI: Diffusion detects stroke, which are bright on diffusion. But anything that makes space tight in the brain can be bright on diffusion (highly cellular masses, clotted blood, pus under pressure, etc.)
--Gradient: Gradient is sensitive to metals. And what’s the most important metal in body? Iron—bc iron is in blood. So gradient is our blood sensitive sequence
So now you know the basic MRI sequences and what they are used for! Now you get rid of all pretenses when it comes to MR sequences!
Los de la Cotorrisa pusieron a rabiar a la hdspm de @vegabiestro y a todo su séquito de js insidiosos y señoras mal cgidas JAJAJAJA qué gozada ver a esa bola de pseudoperiodistas tragando bilis porque un wey los fue a joder haciendo lo mismo que ellos hacen 😂
Need help reading spine imaging? I’ve got your back!
It’s as easy as ABC!
This post is about an easy mnemonic you can use on every single spine study you see to increase your speed & make sure you never miss a thing!
Just remember ABCD:
A = Alignment
(1) look for unstable injuries
(2) look for malalignment that causes early degenerative change
B = Bones
On CT, look for fractures
On MRI, look for marrow lesions/edema
C = Cord/Canal
On CT, look at the canal contents for large masses or collections
On MRI, look for canal narrowing & cord edema
D= Discs/Degenerative
--Normal discs should look like a kidney on it’s side on axial images, w/tiny hilum/. Loss of this hilum means there a bulge
--On sagittal images, normal discs should look like jelly donuts. If they look like pancakes instead of jelly donuts, they are degenerated
Disc nomenclature:
Bulge = gaining weight & loosening belt (annulus gets loose)
Protrusion = hernia (annulus tears & disc protrudes through)
Extrusion = disc becomes like toothpaste & squeezes around everywhere
Free Fragment = like toothpaste on the toothbrush—completely separate from the disc
Now you know how to approach spine imaging studies in a systematic way! Hopefully, now reading spine imaging won’t be such back breaking work!
Time to go with the flow!
Knowing vascular anatomy is the first step to reading any angiogram
These are the key vessels you need to know!
Then I always remember to check for pathology using the mnemonic ANGIO to remind me what to look for:
A = aneurysms, arteriovenous malformations
N = Narrowing (atherosclerotic narrowing)
G = Globules (globular or beaded appearance in vasculitis or RCVS)
I = Irregularity/dissction
O = Occlusion (large vessel occlusion for endovascular)
So now you know the anatomy & pathology to look for angiographic studies!
Remember, there are MANY numbering systems for the carotid. This is just one—so always say the name of the segment and not the number. You never know what numbering system the person reading it uses!!!
Hopefully, now you will never have to circle back on a study of the circle of Willis!!
Here’s how to make hippocampal anatomy memorable!
This video shows hippocampal anatomy that you need to stay in your hippocampus!
--Body is where you can see the spiraling line that is the Cornu Ammonis.
--Cornu Ammonis spirals into the dentate nucleus so that they look like a yin-yang.
The theme of hippocampal anatomy is the spiral—on every single hippocampal MRI, you should look for that T2 dark line of the Cornu Ammonis or SLRM, spiraling into the dentate to make a yin yang!
If this is lost, that is an early sign of MTS.
This month’s @rsnagram @Radiographics has all you need to know about epilepsy, how we image it & how we treat it!
Check it out: https://t.co/QEyDPx1zMD
So now you know the basics of hippocampal anatomy—may you never forget the hippocampal spiral!
@cookyscan1@radiographics@RadG_Editor
1/Need help reading spine imaging? I’ve got your back!
It’s as easy as ABC!
A thread about an easy mnemonic you can use on every single spine study you see to increase your speed & make sure you never miss a thing!
¿Qué dicen las guías sobre el tratamiento inicial de la DM2?
📌 Revisión de GPC de ADA, ESC, NICE, SED, @SemergenGTDM, entre otras.
✅ Consensos clave:
•Metformina: 1.ª opción.
•ECV, IC o ERC: iSGLT-2 /arGLP-1.
•Obesidad: arGLP-1 o GLP-1/GIP
🔗https://t.co/8y5YUyci7O
Me ha pasado algo surrealista comprando en Amazon este Black Friday. Llevo 10 días desesperado y no me dan ninguna solución. Recurro a contarlo aquí porque ya no sé qué más hacer. Al menos, si sirve a alguien para que no le engañen como a mí, bueno será. Abro hilo:
The @goKDIGO recommendation for ‘flozination’ in CKD. 🌟How it all began and how EMPA-KIDNEY and other trials have shaped this journey. Join us tonight at #NephJC to explore this evolution! 🩺✨
Cómo fue la vida de los niños mexicas que vivieron en Tenochtitlan y Tlatelolco durante el apogéo de la Triple Alianza en el siglo XV?
Les comparto un 🔴HILO🔴 basado en Códice Mendocino.
A los 3 años tanto niños y niñas comían media tortilla. El niño no usaba braguero (maxtlatl), solamente usaba su pequeña tilma y la niña su huipil. A esta edad los padres enseñaban a los niños como comportarse. A los 4 años el niño lleva una jícara de agua mientras que la niña se familiariza con el malacate para hilar.
A los 5 años (noten los chalchihuites, círculos verdes en la imagen) comían una tortilla su cumplían con su deberes. La educación de los varones era supervisada por los padres y la de las niñas por sus madres. El niño ya ayudaba cargando parte de la cosecha y la niña sigue bajo la supervisión de la madre.