Mental toughness and critical thinking is seeing through the greatest psyop the world has ever suffered. I’m more proud of these accomplishments than anything else:
-Speaking out against lockdowns on social and being politically active with my local government attempting to educate them.
-Not taking the mRNA and telling as many patients as I could not take the mRNA poison likely saving thousands from harm.
-Seeing patients in person with covid and having them take off their masks so they could breathe air. I saw thousands of patients this way and never got sick.
- I developed the early covid treatment protocol on my own by studying mechanism of action, pathophysiology of the disease and mechanism of repurposing medicine and nutraceuticals within the first weeks of the bioweapon reaching the US (this lecture is incredibly still on my old YouTube channel dated early June 2020).
-I treated thousands outpatient with this early treatment protocol likely saving many from developing worse illnesses and being at the mercy of the hospital vent protocols and remdesivir (which I also correctly warned about publicly on social media).
-Early advocacy for improving metabolic health and eating real foods to avoid worse covid outcomes over vaccination (much to the anger of my peers).
-I recognized wild type and vaccine injuries where my peers gaslit and I developed ways to assess and treat this condition.
-I now enjoy travel without the jab after having fully resigned myself never to travel again due to the European restrictions on unvaccinated (my beloved Western Europe where I grew up is sadly >90% jabbed).
My medical profession was weaponized to gaslight, withhold treatment, and coerce people into joining the greatest human experiment ever seen. Any one of my peers could have stood up and fought back like I did as we were all taught critical thinking in school for the very purpose of advocating for patients and questioning harmful dogma.
This resume is more important than any other accomplishment I’ve had. And it’s one you should ask your doctor for.
The primary care doctor lifestyle is tough: 2,000 patients, 20+ daily visits, endless portal messages. This burnout is driving many away from the profession. #DoctorLife#Burnout
Direct primary care removes healthcare bureaucracy for one-to-one patient interaction. This direct communication can save lives and even covers membership costs by avoiding ER visits for urgent needs like stitches. #DirectPrimaryCare#HealthcareInnovation
Grip Strength Evidence as a biomarker of health
Grip strength (HGS) is a simple, cheap, reliable biomarker of muscle function, biological aging, frailty, and longevity. It strongly predicts all-cause mortality, cardiovascular death, disability, and chronic disease risk across populations.
**Key Studies**
**PURE Study (2015, The Lancet)**
- ~140,000 adults (35–70 yrs) in 17 countries.
- Every 5 kg drop in grip strength linked to:
- 16% higher all-cause mortality (HR 1.16)
- 17% higher CV mortality
- Stronger predictor of death than systolic blood pressure. Results consistent across income levels after full adjustments.
**2017 Meta-Analysis (JAMDA)**
- Lowest vs. highest grip: 41% higher all-cause mortality (HR 1.41), 63% higher CV risk.
- Per 5 kg decrease: 16% higher all-cause, 21% higher CV mortality.
**Umbrella Review of Meta-Analyses**
Higher grip strength associated with:
- 28% lower all-cause mortality (RR 0.72)
- 16% lower CV mortality (RR 0.84)
- 24% lower disability (RR 0.76)
**Additional Findings**
- Midlife grip strength predicted 2.5× higher odds of reaching age 100.
- Low grip links to faster epigenetic aging, frailty, falls, diabetes, cognitive decline, depression, multimorbidity, and poorer quality of life.
- Reflects systemic health (muscle, bone, nutrition, inflammation, neurology).
**Notes**
Cancer mortality links are weaker. Asymmetry may add risk.
**Practical Takeaway**
Grip strength is a vital longevity sign. Improve it via resistance training + nutrition. Use dynamometer cutoffs for sarcopenia/frailty screening. Strong evidence supports tracking and boosting it for longer, healthier life.
@izzers_tennis
Some patients are surprised that we do stem cells in the US. They thought it was only available in Third World countries. It’s available in the US. It’s just more expensive and this is the reason why they cut corners in Third World countries.
Unlock deeper health insights with advanced multi-matrix testing. Dr. Shade's lab offers superior sensitivity by comparing your hair, urine, and blood levels to a wider population baseline. Go beyond basic tests. #HealthTech#LabTesting#Wellness
Everything I do (in my medical practice) is 100% cash.
I have no interest in an insurance company telling me how much I should make based on their random criteria.
If I wanna see a patient for an hour, then I’ll see a patient for an hour. I’m not going to let Insurance company tell me ‘oh we’re only gonna pay you $50 for that visit.’
We are only going to pay you for one diagnosis, regardless of how many you speak with the patient about.
I’m not going to let them say ‘hey this patient doesn’t meet criteria for an MRI so we’re not gonna cover it.’
They know nothing about the patient and simply use either AI or a low education person following a checklist to determine whether or not your lab/imaging/procedure is going to get financially covered.
American health insurance is a scam and really only necessary for catastrophic injuries
There ‘up charge’ rates are so ridiculous.
At the end of the day, they’re in the business of healthcare, they don’t care about your health.
They care about one thing: PROFIT.
You’re just the ends to their means.
You want to actually take care of your health?
Find a doctor that actually cares. Not one that ‘happens to be in my network.’
Who will spend 30-60 minutes with you extensively analyzing your labs, your hormones, your diet, your exercise regiment.
It will be the best money you’ve spent.
‘Traditional’ medicine has turned you in a ‘number.’ One of 25 to 35 numbers every day.
When you just become a number then you have to step back and take matters into your own hands.
It’s time to take your health back.
Quality of life >>>
If someone wants to do a deep dive into their health, with knowledge and experience with finding the ‘root cause’ of your medical issues (gut, mitochondrial, nutritional deficiencies, genetics etc) who is also leading the charge in both peptides and stem cells - the future of medicine - I’m happy to help.
Yes I’m taking new patients and I do telemedicine visits.
🚨 8 out of 10 fears patients have about very low LDL cholesterol are not supported by randomized clinical trial data.
Doctors hear these objections every single day in clinic.
But the 2026 Atherosclerosis review just dismantled them one by one.
I am a cardiologist.
I have patients pushing back on statins and PCSK9 inhibitors because they read something online about cholesterol being "too low."
I have this conversation more than almost any other in my practice.
Here is what the science actually says.
🔬 The review analyzed 10 of the most common fears about very low LDL:
- Brain damage
- Cancer risk
- Hemorrhagic stroke
- Hormonal disruption
- Muscle destruction
- Nerve damage
- Immune suppression
- Diabetes risk
- Fetal harm
- Adrenal dysfunction
8 of those 10 fears have no support from randomized clinical trial data.
Zero.
💓 The ESC/EAS 2025 guidelines define the current target for very high-risk patients as below 55 mg/dL.
Many patients in large trials achieved levels well below that threshold.
The cardiovascular protection was proportional at every step down.
✅ FOURIER TRIAL (evolocumab): major cardiovascular events reduced 15%, LDL driven to median 30 mg/dL with no safety signal
✅ ODYSSEY OUTCOMES (alirocumab): cardiovascular death reduced 15%, with patients reaching LDL levels below 25 mg/dL in some arms without excess harm
✅ IMPROVE-IT (ezetimibe): confirmed that lower LDL beyond statin therapy translates to lower events, even at very low achieved levels
That matters because the argument was never "how low is safe."
The argument should be "how low saves lives."
⚠️ Two concerns from the review do carry legitimate evidentiary support:
🔸 New-onset diabetes. Statins carry a real but modest risk, roughly a 10% relative increase in certain populations. That risk does not eliminate the cardiovascular benefit in high-risk patients.
🔸 Fetal safety. Statins should not be used during pregnancy. That is a real and established contraindication.
Every other fear on that list. Not supported by the data.
❌ "My cholesterol will get too low and damage my brain." Not supported by randomized trial data.
❌ "Very low LDL causes cancer." Not supported by randomized trial data.
❌ "I need cholesterol for my hormones." The body maintains hormonal synthesis even at very low circulating LDL levels. Not supported by randomized trial data.
The tools with the strongest data are unsexy, require a prescription, and require your participation.
🩺 A patient who reaches an LDL below 55 mg/dL after a heart attack and stays there can reduce their risk of a second major cardiovascular event by 15% to 25% depending on the agent used.
That is the difference between a second heart attack and a decade of life with their family.
❤️ Bottom line:
Very low LDL is not dangerous for most patients. It is protective.
This evidence comes from trials enrolling tens of thousands of patients across multiple continents.
Get your LDL measured. Know your risk category. Have an honest conversation with your cardiologist about targets.
If you are very high risk and your LDL is not below 55 mg/dL, that is the conversation you need to have today.
The question is no longer whether low LDL is safe. The question is why so many high-risk patients are still not at goal.
#Cardiology #HeartDisease #HeartHealth #CardiovascularHealth #LDLCholesterol #Statins #PCSK9Inhibitors #CholesterolMyths #PreventiveCardiology #MetabolicHealth
🚨 Your LDL can look normal and you can still have a heart attack.
That happens because LDL measures cholesterol cargo, not the number of particles attacking your arteries.
ApoB counts every single one.
I am a cardiologist and lipid specialist.
I have seen patients with an LDL of 90 mg/dL walk into my office with significant atherosclerosis already developing.
Their ApoB told the real story.
Here is what the science actually says.
🔬 What ApoB actually is:
Every atherogenic particle in your blood carries exactly one ApoB molecule.
LDL carries one. VLDL carries one. IDL carries one. Lp(a) carries one.
ApoB is the headcount of every particle that can penetrate your arterial wall and cause plaque.
LDL cholesterol measures the cargo inside those particles.
Not the particles themselves.
That distinction is everything.
💓 Why this matters clinically:
Two particles can carry the same total cholesterol load.
One particle carries a large cholesterol-rich payload. One particle carries a small payload.
Your LDL number looks identical. Your ApoB number does not.
The patient with more small dense particles has a higher particle count, a higher ApoB, and a higher risk of a heart attack.
LDL missed it entirely.
✅ AMORIS Study (apolipoprotein B): ApoB outperformed LDL cholesterol as a predictor of fatal myocardial infarction across 175,553 patients.
✅ INTERHEART Study (lipid markers): ApoB to ApoA1 ratio showed stronger association with acute MI risk than LDL in 52 countries.
✅ Emerging Risk Factors Collaboration (non-HDL and ApoB): ApoB reclassified cardiovascular risk in patients who appeared low risk by standard lipid panels.
⚠️ The guideline gap that cost patients decades:
For over 20 years the science supported ApoB as the superior marker.
Standard lipid panels kept reporting LDL because it was familiar and cheap.
The 2026 guidelines have now formally aligned with the evidence.
That is 20 years of patients receiving incomplete risk information.
That matters because plaque does not wait for guidelines to catch up.
🩺 What your number should be:
For a low risk patient, ApoB should be below 100 mg/dL.
For a high risk patient with established heart disease or diabetes, ApoB should be below 70 mg/dL.
For very high risk patients, below 60 mg/dL is the target I use in practice.
A standard lipid panel will not tell you any of this.
A patient who asks their doctor for an ApoB test today, discovers elevated particle count despite a normal LDL, and starts targeted therapy can stop plaque progression before a first event.
That is the difference between a normal stress test at 55 and a stent at 58.
❤️ Bottom line:
LDL cholesterol is not the right target. It never was.
ApoB is now supported by two decades of data and formal guideline recognition in 2026.
Ask for your ApoB at your next appointment.
Know your number.
Treat to the right target for your risk level.
A normal LDL with a high ApoB is a missed diagnosis.
Do not let that be you.
The question is no longer whether ApoB is better than LDL.
The question is why your doctor has not ordered it yet.
#Cardiology #HeartDisease #HeartHealth #CardiovascularHealth #ApoB #LDLCholesterol #Atherosclerosis #MetabolicHealth #PreventiveCardiology #LipidManagement
Former Ferrari chairman Montezemolo tears the new electric Ferrari “Luce” apart:
“I cannot say what I really think: I would harm Ferrari. We risk the destruction of a legend. So sorry. Take the Prancing Horse off. At least the Chinese won’t copy this car”
🚨 An LDL of 70 still leaves millions of patients at serious cardiovascular risk. That number felt safe for decades. But the data says otherwise.
Your doctor told you LDL under 70 was the goal. You hit it. You felt protected. You were not.
I am a cardiologist. I have spent over a decade managing lipids in high-risk patients. I have watched people hit every guideline target and still have heart attacks. That is not a coincidence. That is a ceiling problem.
Here is what the science actually says.
💓 The old LDL target of 70 mg/dL came from trials that showed benefit compared to higher numbers. But lower was never tested as a ceiling. It was tested as a floor. The question is no longer whether 70 is better than 130. The question is whether 70 is good enough to stop atherosclerosis from progressing.
It is not.
🔬 Mechanism:
Plaque does not stabilize at LDL 70. It continues to accumulate.
Residual inflammatory risk persists even when LDL appears controlled.
ApoB, not LDL alone, drives particle-level atherogenicity.
Smaller LDL particles penetrate the arterial wall even at lower total LDL concentrations.
Time-weighted LDL exposure across decades determines lifetime plaque burden.
✅ IMPROVE-IT (ezetimibe): cardiovascular events reduced 6.4% by pushing LDL below 70 in patients already on statins.
✅ FOURIER (evolocumab): major adverse cardiovascular events reduced 15% in statin-treated patients by targeting LDL below 30 mg/dL.
✅ ODYSSEY OUTCOMES (alirocumab): all-cause mortality reduced 15% in post-ACS patients with LDL driven to levels previously considered extreme.
✅ JUPITER (rosuvastatin): events reduced 44% in patients with low LDL but elevated hsCRP, proving LDL alone misses the picture.
And FOURIER changed everything. It demolished the floor argument. There is no J-curve. Lower LDL means fewer events. Full stop.
That matters because every point above your true biological LDL floor is costing someone a cardiac event they did not have to have.
⚠️ What most patients are never told:
LDL 70 is a guideline threshold, not a biological finish line.
Patients with prior MI, diabetes, or familial hypercholesterolemia carry higher residual risk at LDL 70 than guidelines historically acknowledged.
ApoB can remain elevated even when LDL appears controlled.
Lp(a) adds independent risk that LDL measurement does not capture.
🩺 Ask your cardiologist these specific numbers:
What is my ApoB?
What is my Lp(a)?
What is my hsCRP?
What is my actual 10-year ASCVD risk score?
If your doctor only checked your LDL and called it a day, you have an incomplete picture.
🔸 The tools exist to go lower safely:
High-intensity statins
Ezetimibe added to statins with zero major safety concerns
PCSK9 inhibitors for patients with established disease or familial hypercholesterolemia
Inclisiran for patients who need twice-yearly dosing instead of daily pills
Bempedoic acid for statin-intolerant patients
❌ Coenzyme Q10 will not save you.
❌ Red yeast rice will not save you.
❌ Omega-3 supplements at standard doses will not save you.
The tools with the strongest data are unsexy, free, and require your participation.
A patient who hits LDL 70 and stops there can continue accumulating plaque for 10 to 20 years while believing they are protected. A patient who pushes ApoB below 60, drives LDL to 40 to 55, and addresses inflammation with lifestyle and targeted therapy can halt progression and reduce event risk by 40% or more over the same period.
That is the difference between a preventable heart attack and a preventable life.
❤️ Bottom line:
LDL 70 is not a destination. It is a starting point that the data has already moved past.
FOURIER, ODYSSEY OUTCOMES, and IMPROVE-IT together represent over 60,000 patients proving that lower LDL saves more lives without a safety ceiling.
Know your ApoB. Know your Lp(a). Know your hsCRP. Demand a full lipid picture, not just a total LDL number. Push your care team to treat to biological targets, not just guideline minimums. Start today, because every year at a suboptimal LDL is a year of plaque you cannot take back.
The question is not whether you can go lower. The question is why you have not yet.
#Cardiology #HeartDisease #HeartHealth #CardiovascularHealth #LDL #ApoB #Lpa #Statins #PreventiveCardiology #MetabolicHealth
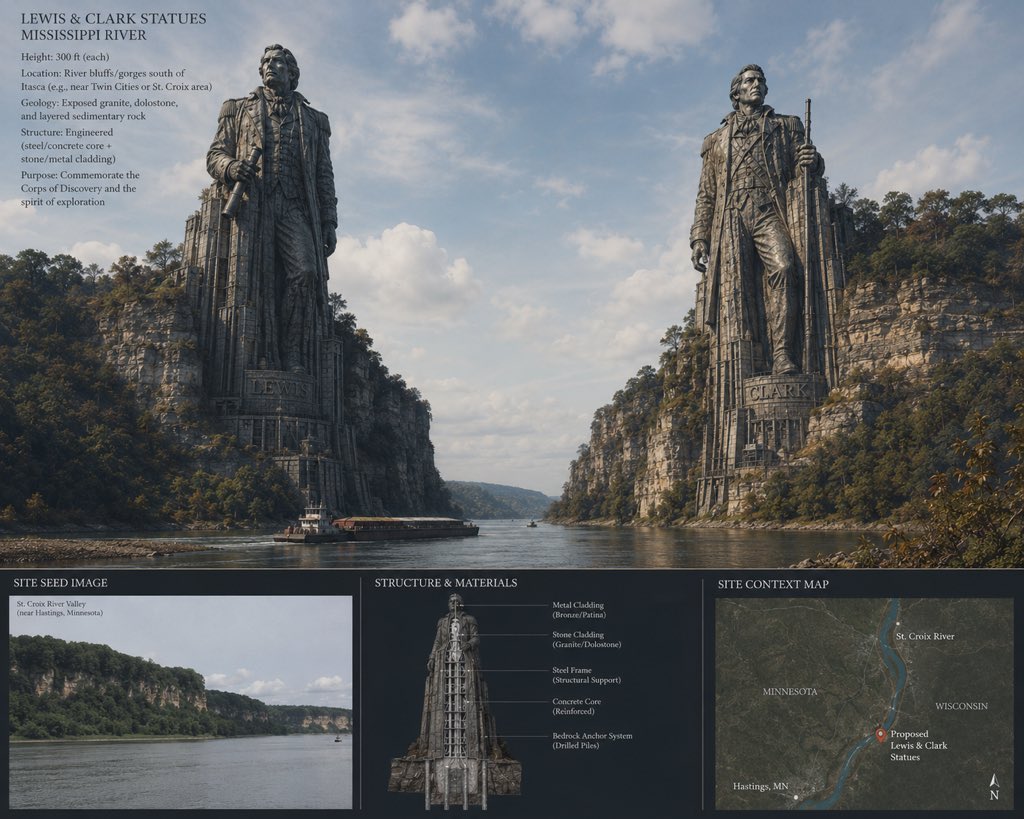
I think we need to build this.
I designed this below image, representing Lewis and Clark on the Mississippi in the style of Argonath.
At $1 Billion or more, I think it can be done.
A cardiologist is telling 1.9 million people the gut is the problem. His supplement store is the solution.
@DrJackWolfson runs NaturalHeartDoctor, a supplement line built on the premise that cholesterol is not the cause of heart disease and the real answer is gut health and natural protocols. The free ebook is the top of the funnel.
Precious.
The gut-inflammation-heart connection is a real area of research. It does not have a single cardiovascular outcomes trial showing that gut health intervention reduces heart attacks or all-cause mortality. Not one. CANTOS directly targeted inflammation with a precision biologic. 15% MACE reduction. No all-cause mortality benefit. Fatal infection signal. That is the best inflammation-first trial ever run and it did not move the mortality needle.
ApoB-containing particles accumulate in the arterial wall regardless of gut health status. @foundationofnla has published on why particle burden remains the operative variable even when metabolic markers improve.
The binary for his 1.9 million readers: evidence-based lipid management with a 30-year outcomes record, or a gut health protocol from a cardiologist whose income depends on you not taking the former.
Choose wisely my friends.
🫀 This paper is quietly dangerous. Not because it’s wrong— but because it can be misunderstood.
Let’s go straight to the core.
What the study actually shows
In 479 CCS patients undergoing CCTA:
👉 Lower LDL-C (<70 mg/dL)
was associated with
👉 MORE severe CAD and higher plaque burden
Even more interesting:
👉 These patients had
- more diabetes / pre-diabetes
- more metabolic syndrome
- worse glucose metabolism markers
And:
👉 Diabetes (OR ~6.1) and pre-diabetes remained strong independent predictors of CAD risk
The uncomfortable observation
👉 The “best treated” patients (low LDL) had the worst arteries
Before anyone panics:
This is NOT saying LDL reduction is harmful.
This is saying something much more subtle—and more important.
What is really happening?
1. Reverse causality (the elephant in the room)
Patients with:
👉 prior events
👉 higher baseline risk
👉 more aggressive treatment
→ end up with lower LDL
So:
👉 Low LDL is a marker of treated high-risk patients
Not the cause of disease.
2. Metabolic risk is the real signal
The study shows very clearly:
👉 Glucose dysregulation dominates residual risk
- Diabetes
- Pre-diabetes
- Insulin resistance
- Metabolic syndrome
→ strongly associated with plaque burden and Leiden score
This is the key shift
For years, we simplified CAD risk to:
👉 LDL = bad → lower is better
That’s still true.
But incomplete.
What this paper actually teaches
👉 You can have “perfect LDL” and still have high atherosclerotic risk
Because:
👉 Atherosclerosis ≠ cholesterol alone
👉 It is a metabolic + inflammatory + vascular disease
The imaging angle (the real gold here)
CCTA shows:
👉 more non-calcified plaques in low LDL group
👉 higher plaque burden (SIS)
👉 higher Leiden risk scores
This is exactly where imaging becomes decisive:
👉 Biology > numbers
Clinical implication (the part guidelines are still catching up with)
Treating LDL alone:
❌ does NOT eliminate risk
Because:
👉 residual risk = metabolic + inflammatory + phenotypic
My take
This paper reinforces a concept that is still underused clinically:
👉 CAD is an atheroma disease, not a cholesterol disease
The real mistake to avoid
A superficial reading would lead to:
❌ “Low LDL is associated with more disease → LDL doesn’t matter”
That would be wrong.
The correct interpretation
👉 LDL lowering works
👉 BUT it does not address the whole disease
Where this goes next
This is exactly where:
👉 advanced CCTA (plaque quantification, phenotype)
👉 PCCT (microstructure, composition)
👉 AI-QCT
will redefine risk stratification.
Bottom line
👉 LDL reduction is necessary
👉 but absolutely not sufficient
And if you only track LDL:
👉 you are managing a number
👉 not the disease
I didn’t really catch that they are now proclaiming apo B as the one to watch. There were a few reviewers who voted to make it so but they ended up supporting LDL again as the main metric to track. I agree apo B is way better especially since patients don’t seem to always understand thay fasting labs does not mean you can add cream to your coffee.