❓ "But they're too drowsy to assess."
I hear this regularly. A patient is lying quietly, eyes closed, not responding to questions. How can we screen for delirium if they won't engage?
✅ 𝐇𝐞𝐫𝐞'𝐬 𝐭𝐡𝐞 𝐜𝐥𝐢𝐧𝐢𝐜𝐚𝐥 𝐩𝐞𝐚𝐫𝐥: 𝐝𝐫𝐨𝐰𝐬𝐢𝐧𝐞𝐬𝐬 𝐈𝐒 𝐭𝐡𝐞 𝐚𝐬𝐬𝐞𝐬𝐬𝐦𝐞𝐧𝐭.
A patient who is drowsy or unrousable has altered consciousness - which is itself a key feature of delirium. You don't need them to answer orientation questions to recognise something is wrong.
The 4AT was designed with this in mind. Item 1 assesses alertness first. A patient who is clearly abnormally sleepy, or agitated, scores 4 points immediately - meeting the threshold for possible delirium before you even ask about the year or the months backwards.
𝑾𝒉𝒂𝒕 𝒕𝒐 𝒅𝒐 𝒘𝒊𝒕𝒉 𝒕𝒉𝒆 𝒅𝒓𝒐𝒘𝒔𝒚 𝒑𝒂𝒕𝒊𝒆𝒏𝒕:
Check their level of arousal. Are they sleepy but rousable? Only rousable to physical stimulus? Unrousable?
Consider this altered consciousness as clinical information. In most cases, the patient will fulfil criteria for delirium when assessed.
➡️ The sleepy patient isn't unsuitable for assessment. The sleepiness is a critical clinical sign.
What's your approach when the patient is too drowsy to complete cognitive testing?
She survived the admission.
But what happens after discharge?
Too often: fragmented care, medication errors & caregiver stress.
Malaysia needs better transitional care for older persons.
Join us at #MCGM2026 for the launch of MSGM’s position statement.
https://t.co/w60YIptxec
Ageing in place is only possible when we manage:
🧠 Cognitive decline
🚶 Recurrent falls
💪 Frailty & sarcopenia
Join us at the MCGM symposium
Managing Geriatric Syndromes in Supporting Ageing in Place
Practical. Community-focused. Immediately applicable.
https://t.co/IjGHJ87umG
More than 1 in 3 older inpatients in this study were dehydrated.
Dehydrated patients: 13% higher odds of falling (OR 1.13, P=.002).
↳ Dehydration is cheap to fix - but easy to miss.
💧💧💧💧💧💧💧💧
⇉ Do you check fluid status on every ward round?
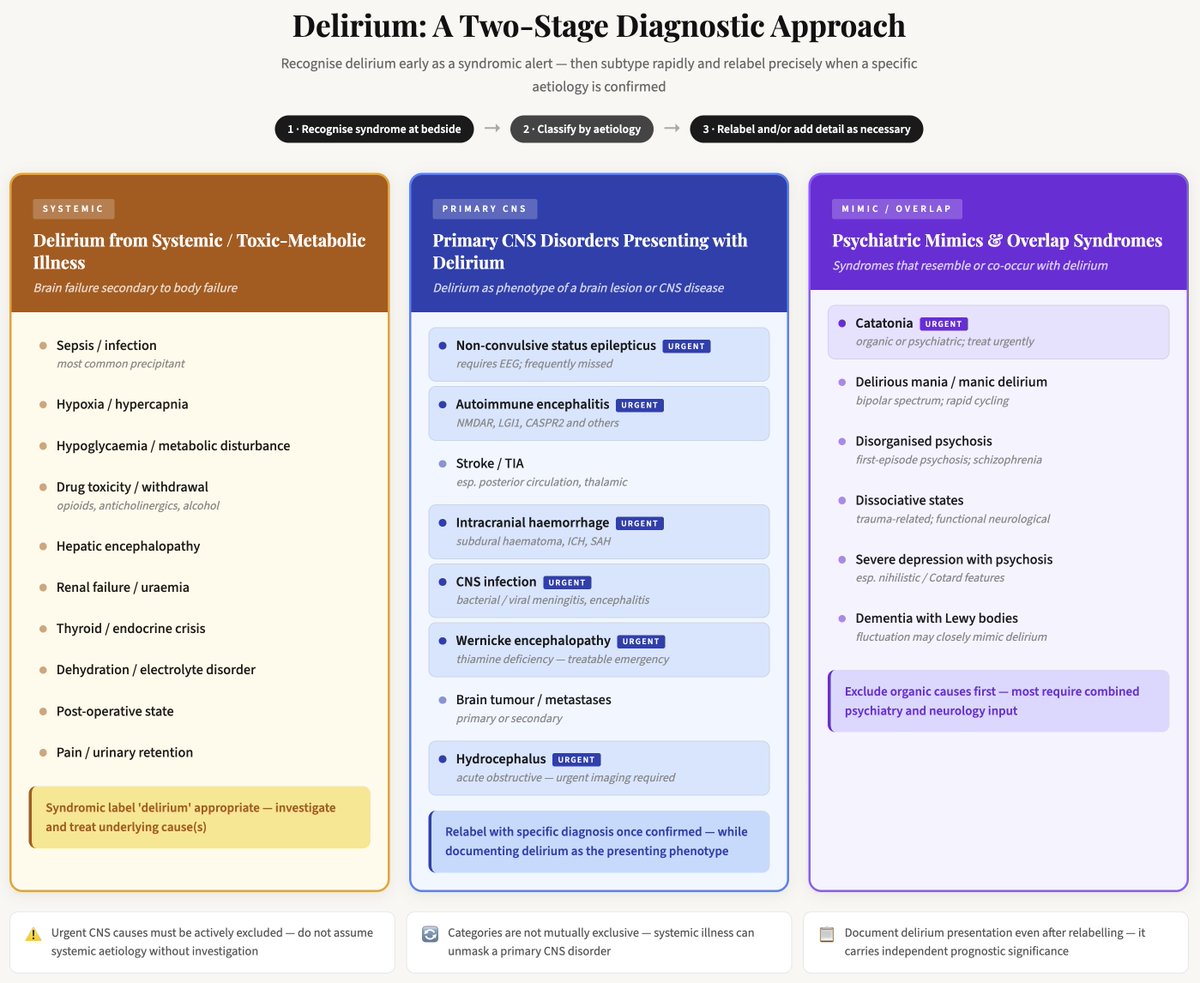
Most delirium is caused by acute triggers originating outside the brain.
But there are some primary brain causes, and there are also some psychiatric mimics.
This diagram shows this. The first thing is to make the diagnosis of delirium, but then to carefully consider systemic and non-systemic causes, as well as the admittedly rarer psychiatric mimics.
#neurology #psychiatry #WDAD2026
Our official Photography Competition is NOW OPEN. Show us your best shot depicting "Ageing in Place" in Malaysia for a chance to be featured at #MCGM2026.
📸 Submit: https://t.co/g35HYs4Axr
📌 Malaysian Congress of Geriatric Medicine 2026
🗓 9–11 July 2026 | 📍 KLCC
#MCGM2026
Alzheimer’s disease is not equivalent to dementia. The new revised criteria for diagnosis and staging using biomarkers are discussed in this amazing podcast! @GreenJournal https://t.co/2G6gyV1BJr
Ageing in place starts in the community — not the hospital.
This Hari Warga Emas activity at Klinik Kesihatan Kepala Batas & PAWE Kepala Batas reflects the real-world practice behind our theme:
Ageing in Place – Continuity, Community & Care.
#MCGM2026#AgeingInPlace
✨ First time at MCGM!
Trade Visitors are welcome to our annual exhibition. Connect, explore eldercare innovations & discover ageing care trends.
✔ Complimentary registration (subject to approval)
🔗 Register now: https://t.co/1Cgo4xDeXW
❓ "But they're too drowsy to assess."
I hear this regularly. A patient is lying quietly, eyes closed, not responding to questions. How can we screen for delirium if they won't engage?
✅ 𝐇𝐞𝐫𝐞'𝐬 𝐭𝐡𝐞 𝐜𝐥𝐢𝐧𝐢𝐜𝐚𝐥 𝐩𝐞𝐚𝐫𝐥: 𝐝𝐫𝐨𝐰𝐬𝐢𝐧𝐞𝐬𝐬 𝐈𝐒 𝐭𝐡𝐞 𝐚𝐬𝐬𝐞𝐬𝐬𝐦𝐞𝐧𝐭.
A patient who is drowsy or unrousable has altered consciousness - which is itself a key feature of delirium. You don't need them to answer orientation questions to recognise something is wrong.
The 4AT was designed with this in mind. Item 1 assesses alertness first. A patient who is clearly abnormally sleepy, or agitated, scores 4 points immediately - meeting the threshold for possible delirium before you even ask about the year or the months backwards.
𝑾𝒉𝒂𝒕 𝒕𝒐 𝒅𝒐 𝒘𝒊𝒕𝒉 𝒕𝒉𝒆 𝒅𝒓𝒐𝒘𝒔𝒚 𝒑𝒂𝒕𝒊𝒆𝒏𝒕:
Check their level of arousal. Are they sleepy but rousable? Only rousable to physical stimulus? Unrousable?
Consider this altered consciousness as clinical information. In most cases, the patient will fulfil criteria for delirium when assessed.
➡️ The sleepy patient isn't unsuitable for assessment. The sleepiness is a critical clinical sign.
What's your approach when the patient is too drowsy to complete cognitive testing?
Nutritional Management Guidelines for Sarcopenia and Frailty 2025.
The Japanese Society of Clinical Nutrition and the Japanese Association on Sarcopenia and Frailty developed this guideline.
I hope many people read and make use of it. It's open access.
https://t.co/HGO0WwgDi1
This 2005 study by Andrew, Freter & Rockwood was one of the first to show that when doctors didn't recognise delirium, outcomes were significantly worse.
68% of patients had poor outcomes at 6 months. But the most striking finding: poor recognition by the treating team was associated with 18x higher odds of death or functional decline.
Twenty years on, under-recognition remains the single most fixable problem in delirium care.
Are we any better at it now?
#delirium #geriatrics
🧠 𝐃𝐢𝐝 𝐘𝐨𝐮 𝐊𝐧𝐨𝐰? 𝐀 𝐁𝐫𝐢𝐞𝐟 𝐇𝐢𝐬𝐭𝐨𝐫𝐲 𝐨𝐟 𝐃𝐞𝐥𝐢𝐫𝐢𝐮𝐦
For most families, delirium remains an unfamiliar term, at least in relation to health. But the symptoms of delirium - sudden confusion, agitation or extreme sleepiness - have been described for thousands of years.
Around 2,400 years ago, the Greek physician Hippocrates wrote about people experiencing abrupt confusion, especially during fevers. He called this "phrenitis". He described a mixture of symptoms, including restlessness, losing the ability to think clearly, being upset, and behaving in unusual ways.
Hippocrates also wrote about a related state which he called "lethargus," where people became withdrawn and sleepy. Importantly, he noted patients could move between these two states, from agitation to drowsiness.
The word "delirium" itself comes from the Latin "delirare," meaning "to leave the furrow". It's a useful image: a mind suddenly veering off track. A Roman physician named Celsus, working in the first century AD, was the first to use "delirium" in medical writing.
Since these ancient times, sudden changes in mental functioning triggered by medical illnesses were commonly noted in medical and historical texts. For example, Procopius noted that plague victims sometimes showed agitation and paranoia, while others fell into a prolonged sleep.
By the 1800s, doctors had started recording that delirium involved a kind of mental "clouding," meaning difficulties in concentrating and thinking.
A significant step forward came in the 1940s when scientists began measuring brain activity through EEGs (brain wave tests), confirming that delirium involved measurable changes in how the brain worked.
𝐓𝐨𝐝𝐚𝐲, 𝐡𝐞𝐚𝐥𝐭𝐡𝐜𝐚𝐫𝐞 𝐩𝐫𝐨𝐟𝐞𝐬𝐬𝐢𝐨𝐧𝐚𝐥𝐬 𝐮𝐬𝐞 𝐚𝐠𝐫𝐞𝐞𝐝 𝐜𝐡𝐞𝐜𝐤𝐥𝐢𝐬𝐭𝐬 𝐨𝐟 𝐟𝐞𝐚𝐭𝐮𝐫𝐞𝐬 𝐭𝐨 𝐢𝐝𝐞𝐧𝐭𝐢𝐟𝐲 𝐝𝐞𝐥𝐢𝐫𝐢𝐮𝐦.
Yet the essential features Hippocrates first described, sudden confusion, disrupted sleep, and symptoms that come and go, remain remarkably unchanged after thousands of years.
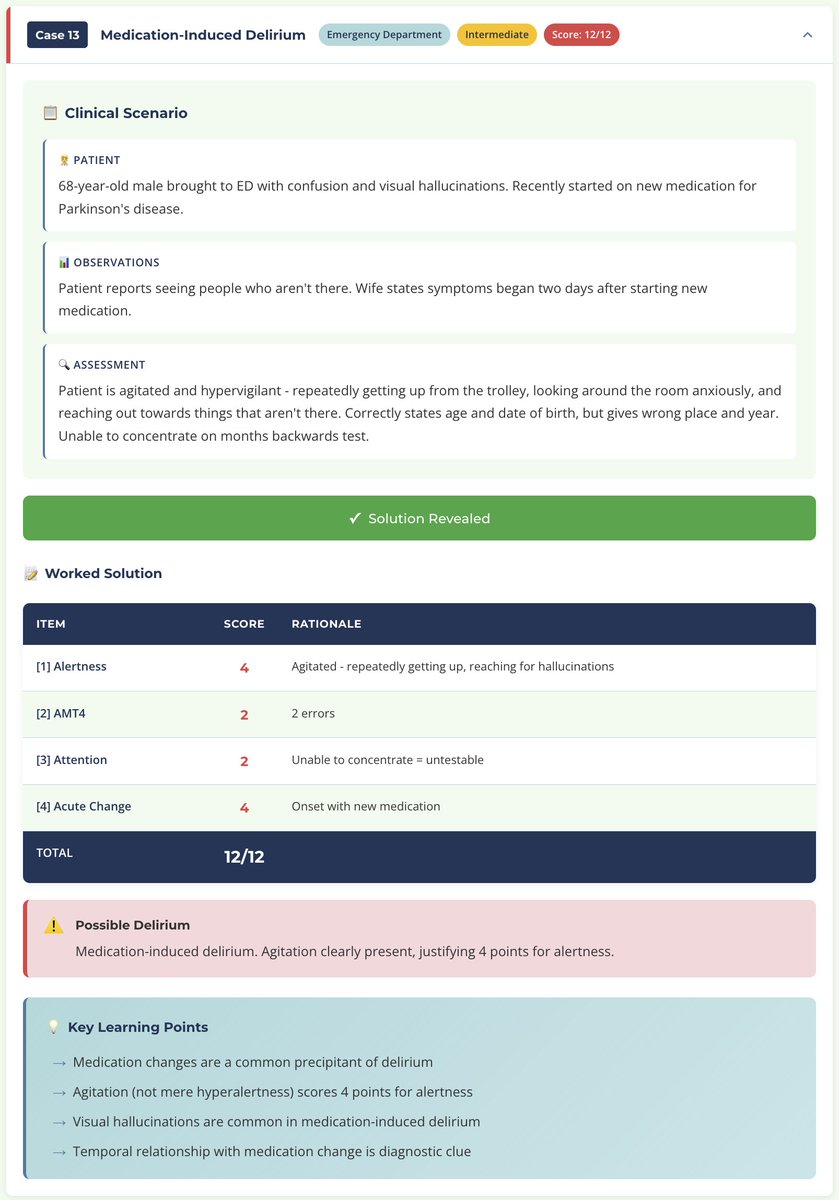
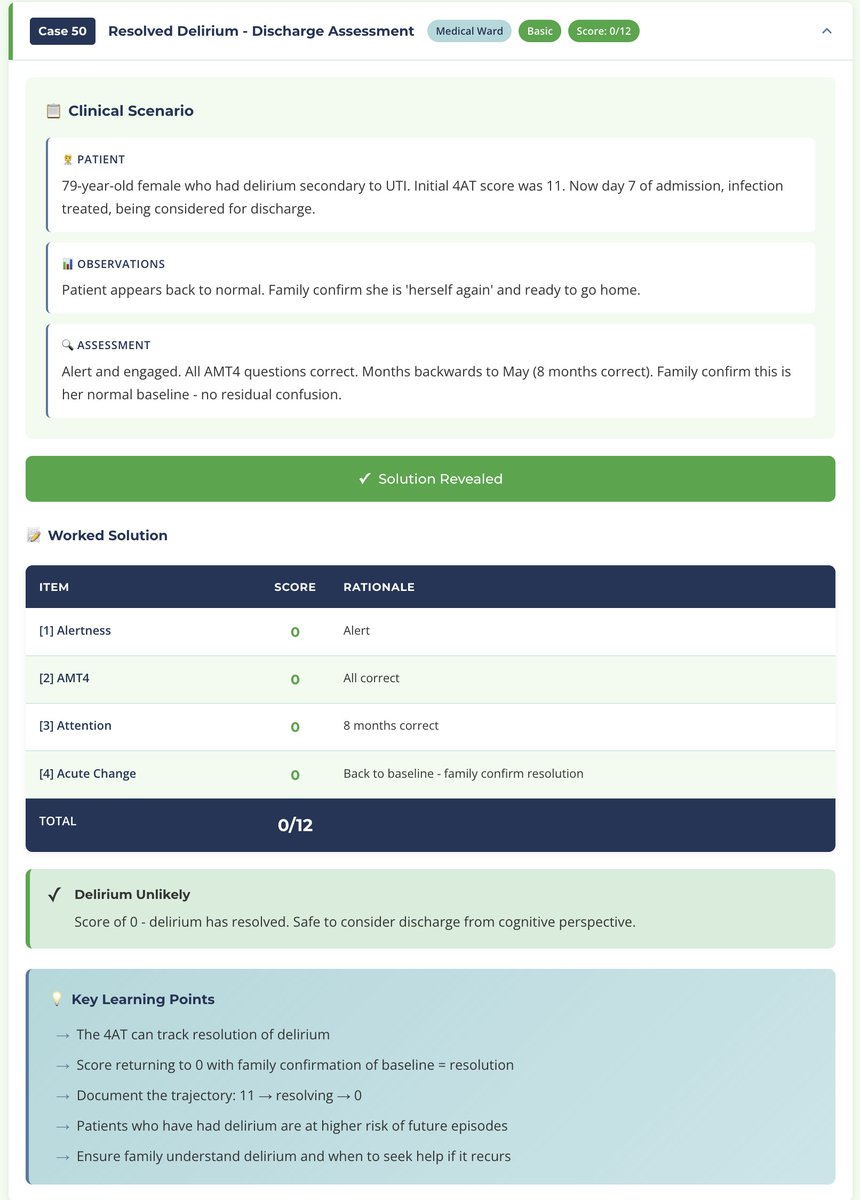
⭐ New delirium resource: 50 free clinical cases to practice 4AT #delirium scoring
12 healthcare settings. 3 difficulty levels. Read the case, note your score, then click 'Show Worked Solution'.
No login. No ads. Just learning.
Please RT & share with colleagues!
Link 👇