Neonatologist. Researcher. Passionate about neonatal resuscitation, optimization of oxygen use, quality improvement and innovation. Opinions are my own.
If you missed it, the latest @AAPneonatal Journal Club is now up on youtube - https://t.co/riEcQZpCzm!
Dr. Budh provided an excellent review of TORPIDO 30/60, with Dr. Ju-Lee Oei and @KapadiaNeo providing great insights. #neotwitter@NeoTECaN@vjain_md@mattie_wolf
Sharing our commentary in @Ped_Research with @gargparvesh2011@crmartin90 & Srini Bolisetty
on IV lipids in neonates.
Do not blindly follow trends
Base it on physiology, duration of need, risk factors.
First Do No Trend!
https://t.co/74IFxiB1hT
@NeoConsortium@AAPneonatal
If you teach neonatal resuscitation, congratulations. You save lives. The data says so. Very proud of Dr. Neveln, a mentee of mine @BCMNeonatal. A lot of work to write a @CochraneNeonate review. @AAPneonatal@Ilcor_org https://t.co/tZIuqk3ztR
Would we still be doing cord milking in extremely preterm infants if PREMOD2 did not allow for waiver of antenatal consent? Have a look at Dr. Barrington's take on our study of waiver vs no waiver eligibility? https://t.co/UtpOep02Ti
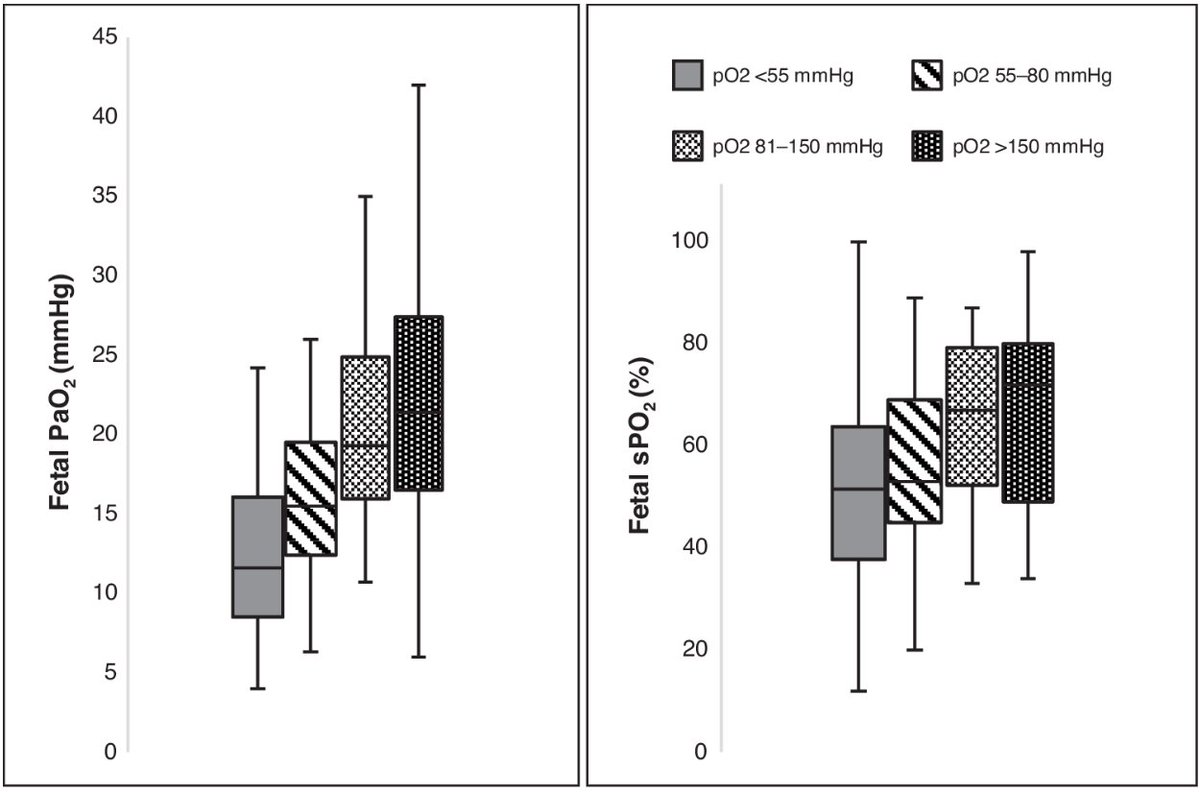
Amazing buffering capacity of the placenta - impact of maternal hypoxemia and hyperoxemia on fetal oxygenation by Drs. Michelle Lim and Nithi Fernandes @pedresearch https://t.co/I5Ganbsmxv
Attend our workshop at #APLUSConference at #UTSW if you want to know more about "Confirmation of less invasive surfactant administration catheter placement with capnography" @LoriBautistaMD@vkakkilaya@KapadiaNeo
https://t.co/FydkXYT6Cd
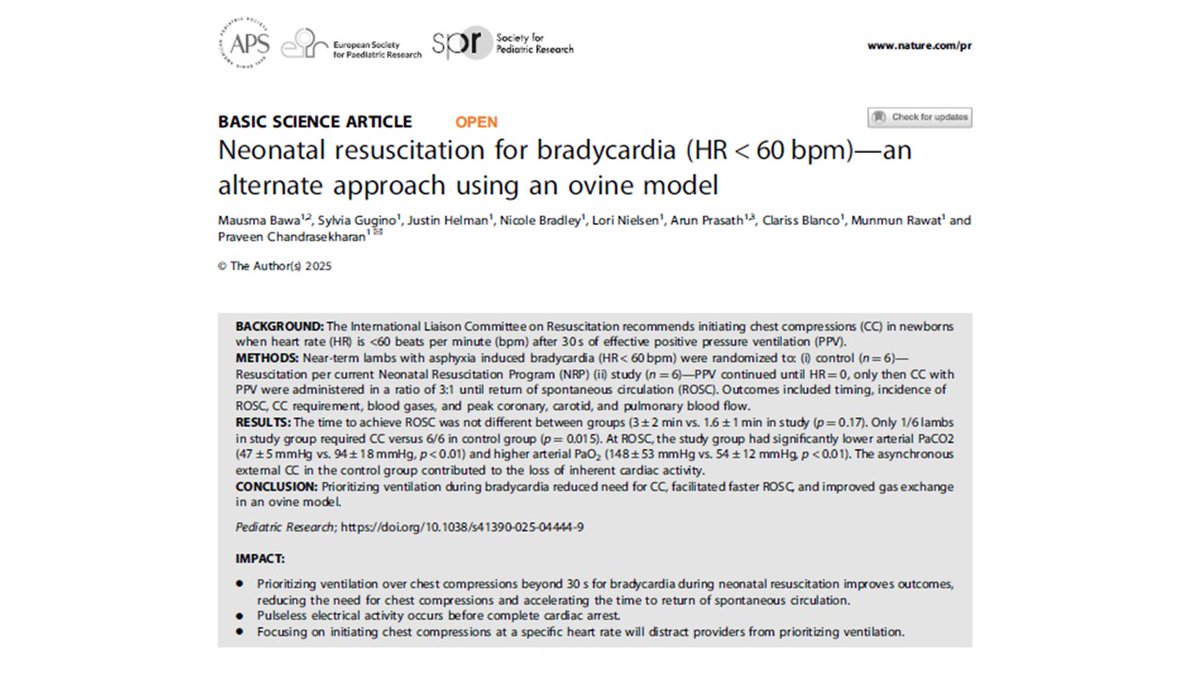
https://t.co/R5MCLn7KEn Neonatal resuscitation for bradycardia (HR < 60 bpm)—an alternate approach using an ovine model @MausmaBawa @ Sgugino @ Jhelman @ Nbradley @ LNielsen @gsarunprasath@clablancomd@munmun_rawat@neosatyan@NeoResus@AAPneonatal@AmerAcadPeds@Ped_Research@SPR@EAPSCongress - Our recent novel ovine study on neonatal resuscitation found that prioritizing ventilation beyond 30 seconds for bradycardia improved outcomes compared to current NRP guidelines. Only 1/6 lambs in the ventilation-first group required chest compressions versus 6/6 controls (p=0.015). Ventilation-first animals also demonstrated superior gas exchange, with lower PaCO₂ and higher PaO₂ at return of spontaneous circulation (ROSC). Importantly, premature chest compressions suppressed intrinsic cardiac activity. These data suggest ventilation should remain the primary intervention during bradycardia, supporting a shift away from compressions at an arbitrary heart rate threshold and toward evidence-based refinements in resuscitation practice.
Don’t forget to register for the upcoming #APLUSConference at #UTSW on Nov. 14. Register today to join this immersive one-day event on advancing noninvasive premature lung and brain protection. General registration closes on Nov. 10. Learn more: https://t.co/a4WtjTo8ZV
Have you registered for the Aplus conference yet? Hang out with us as we learn all about what's new in the field of respiratory support in extremely preterm infants. We will talk about SALSA, LISA, iNO, best practices for tiny babies, and my favorite delivery room resuscitation. @AAPneonatal@vkakkilaya@natetexsun@neosatyan
Registration for the APLUS Conference at #UTSW is now open. Join us for this one-day event on the latest advancements in noninvasive premature lung and brain protection and earn CME credits. Learn more: https://t.co/a4WtjTo8ZV
@Parkland@childrens#APLUSConference#Neonatology