Save the Date! May 21-24th 2025, Mayo Neuro and Intensive Care CPD at the Ritz Carlton Orlando, FL 🌴 🌞
“Time is Brain” for a number of neurologic emergencies including 🧠🩸“CODE ICH”
🔗 https://t.co/l45ayNX2kW
@neurocritical@enlscourse 5/24/2025
https://t.co/H6RWi5KBNE
Are you a physician, advanced practice provider, nurse, technician, or other health professional interested in #neurovascular#ultrasound or #transcranial#Doppler? The ASN offers an excellent program for credentialing in #neurosonology. Find out more at https://t.co/p7mkQGqnQg
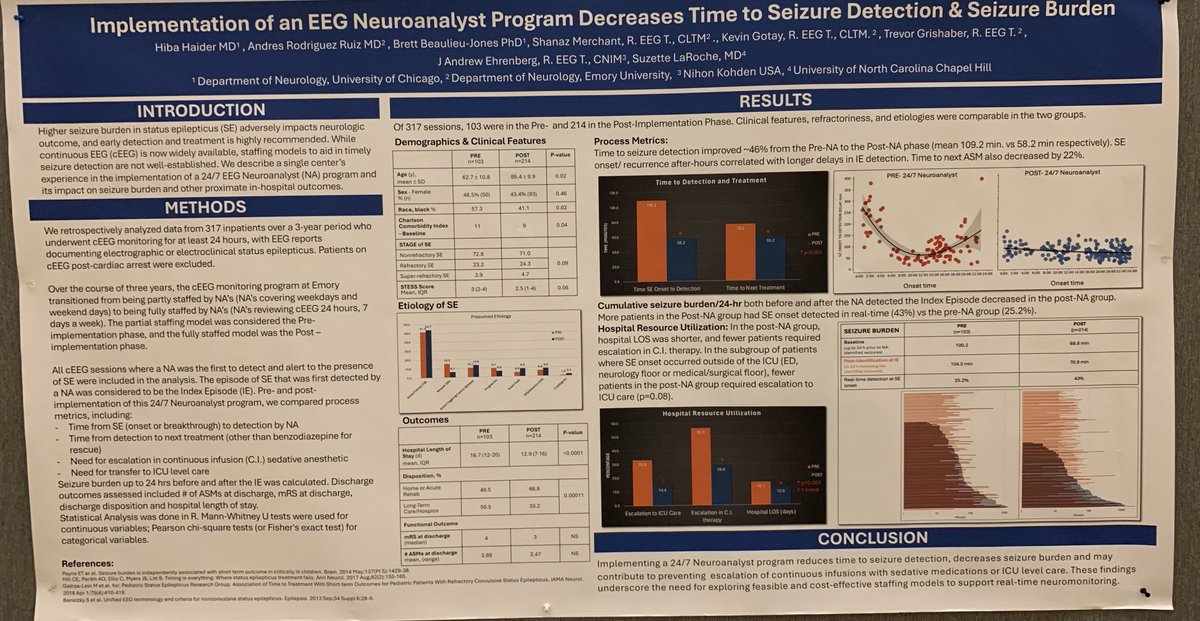
#acns2024 best alarm system remains human eyes, but is it cost efficient? NA-CLTM program towards 24/7/365 monitoring for immediate detection of seizures to be reported to the EEGer MD.
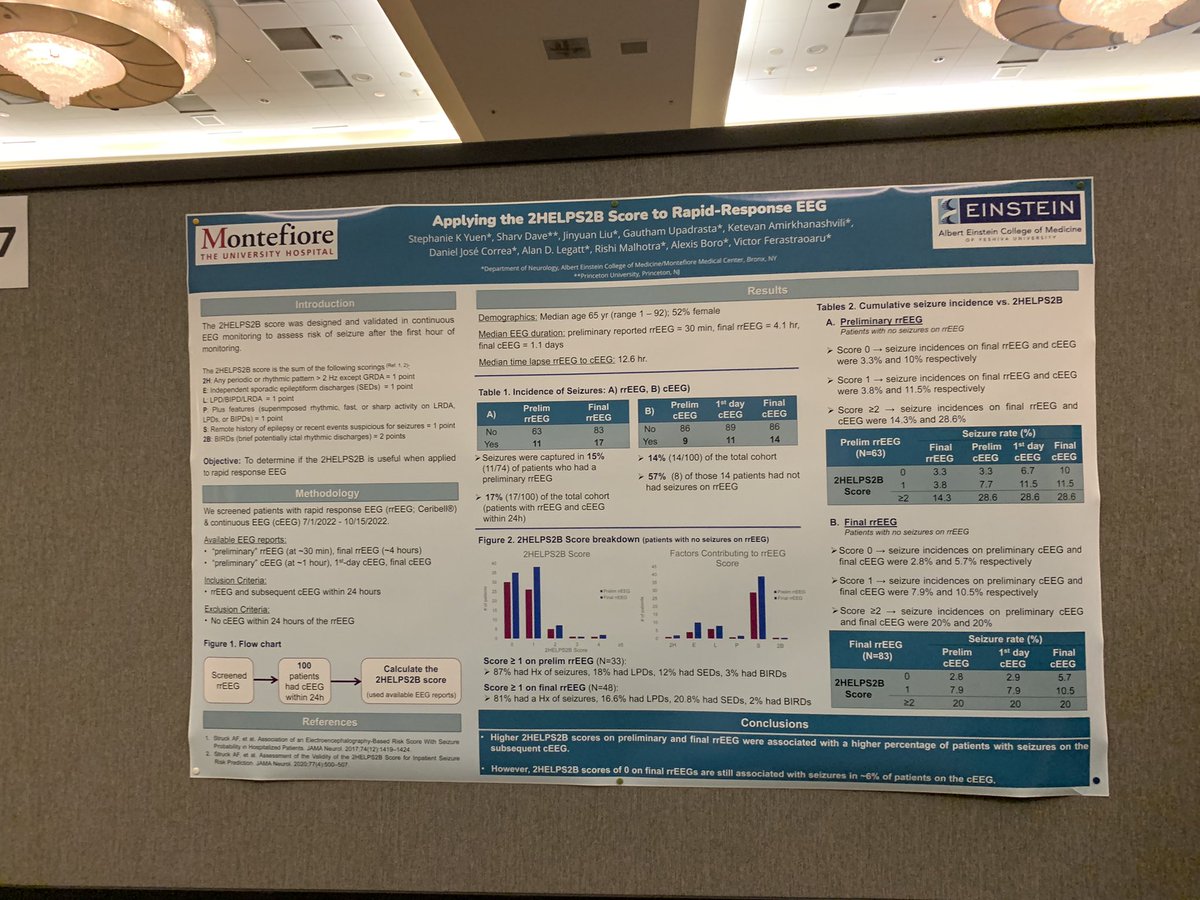
#ACNS2024 My favourite poster, verifying validity of 2HELPS2B on first 30min of POCEEG: Good triaging tool as it replicates gradation along score, but imperfect screen with 6% FNR.
#ACNS2024 red orange band definition as narrow vs broad for spike composition of the PRA, flame shape, laterality, distinguishing artifacts, great qEEG DSA talk by Brandon Westover!
ASN is launching an open access online journal that will focus on clinical applications of neuroimaging. We are looking for a social media editor, please complete & submit this form to apply: https://t.co/k87GxXz8cu
Freezing from undisclosed Parkinson, sure, gait has some features, stuporous look can match, but he seems very much unaware and not memorizing, so focal temporal seizures still more likely than PD. Interrogating his recollection of pre per post sxs is key. https://t.co/0HKozzop9j
Exactly. Consciousness alteration disorders are diverse with each domain being specific. #postconcussivedisorder with brain fog, cognitive difficulties, lightheadedness DO NOT present as blank stares. #nonconvulsiveseizures do. https://t.co/Rkf1EoV9mg
US Capitol top doc who cleared McConnell is lying. Any neurologist can tell these events weren’t “lightheadedness” by def, but blank stares which can suggest nonconvulsive seizures. Post concussion sd also not giving you blank stares but fog https://t.co/Od3d2HjHPK via @bpolitics
Grateful for the leadership of @neurollama leading us through this Delphi process. These “Practice Standards for the Use of Multimodality Neuromonitoring” now out in @CritCareMed enable advocacy for personnel, technology, reporting, education, & analytics https://t.co/ax9ogzUfBz
What a great #ISTH2023 — and a huge thank you to @AnticoagPharmD for taking over our Twitter account and keeping everyone updated on the latest and greatest #thrombosis news!
When was the last time you visited the Neuroanesthesia Classroom? This online roadmap for residents rotating through #neuroanesthesia links keywords to PBLDs, quizzes, & topic-specific peer-reviewed articles. #FOAMed#neuroscience https://t.co/OT9bARiu2l
@salia_farrokh @tigernole13 @senelson13 Not sure I like this: MDZ too short acting c/t LRZ but gradation is great. MINDS not best c/t Cushman. Using VPA PHB once only, as “adjunct”, is misleading, better as core standing w/ LRZ prn. Dexmed and prop drips great but intensive. Last step MDZ drip too short acting c/t PHB.
@katereillymd@stephanamayer Exactly, this is why I push for using what ACF DOAC GLs and ACEP GLs recommend: 2,000 flat dose for DOAC reversal, reserving 25-50IU/kg per weight and INR to WAICH and 50IU/kg solely to hemophiliacs. Costs saved on Kcentra by this strategy can be reinvested towards Andexanet!
@Nicole_Davis026@AlexReynoldsMD@stephanamayer True, ideally fast access to Kcentra in the comparative arm. Im just bitter about arguments made solely based on pricing. With this logic, we would never have immunoRx in cancer as all these Abs are very expensive. No LEV as PHT more cost effective. No MRI as CT sufficient.