@northwoods1980 L clavicle osteoid osteoma would be my first guess. I think I can discern a nodus within the inferior cortex. However this is only a guess without an MRI
Long nail.
Looks pathological - if the patient has cancer history I would CT first as it could change management (long life expectancy & pathological fx may be better managed with PF EPR).
Assess for stiffness/OA/fixed flexion in the contralateral hip before setting up for a nail. If FFD then set up the fx table with some hip flexion. It's impossible to get the fx fragments to meet if the proximal fragment is fixed flexed and the distal extended.
@medflutter_@DrFraneNicholas@IMNailR@orthotraumamd Personally, I’d have preferred 3 proximal screws for a fracture above the isthmus, but I don’t think you did anything wrong. T&O is humbling like that. Sometimes you miss a detail and the patient does well, sometimes you do everything right and they suffer.
Returning soon! The UK's oldest FRCS course, initiated by Apley many years ago, is making a comeback. Sponsored pricing, restricted availability. Gratitude to our sponsors Acumed and our committed faculty. Date: 19.04.2026
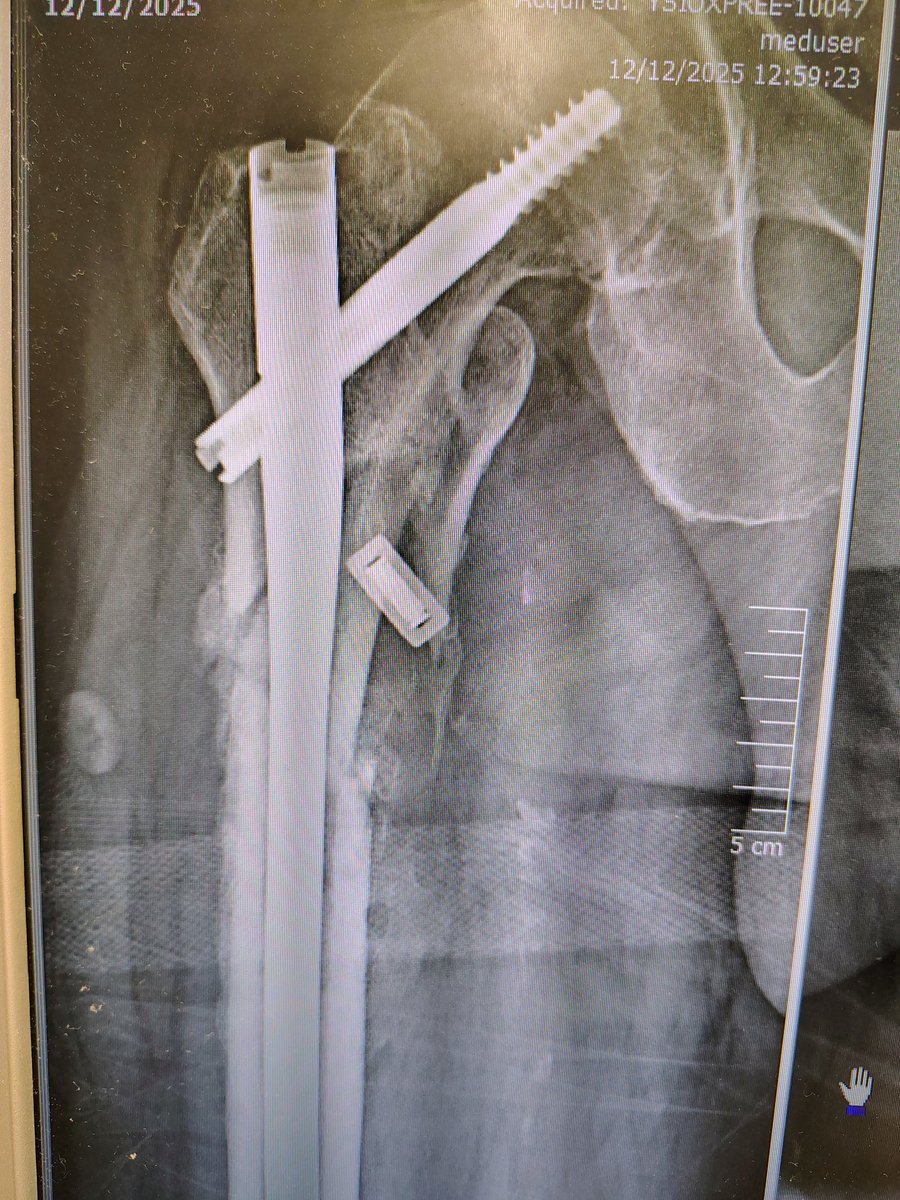
@InvictaOrtho Looks like we are winning. Lag screws have loosened as expected but metalwork intact & patient walking without aids. Still watching this one
Difficult medial malleolar fractures: salvage options
72 year old f&w lady pulled by the dog sustaining this fracture. Closed but with moderate skin tethering medially just above the medial malleolar fragments. Rudimentarily reduced in ED and operated next morning.
#orthotwitter
Thank you for this post. Have long thought elbow braces are not fit for purpose. Backslab for 1-2 weeks post injury and bulky bandaging for the first days postop is what I rely on. And then early active ROM exercises supine with arm vertical and forearm above torso, effectively using the forearm weight to maintain ghe elbow in joint
Distal locking failure
75yo comorbid gentleman, broke the distal locking screws of his Gamma2. Initially had a length unstable butterfly subtrochanteric fixed 5 months ago. Bloods negative, no signs of infection. New onset mild knee symptoms.
#orthotwitter
Intraop cultures came back negative 🙏🏻. The patient is recovering, 8 weeks down the line still has some pain but can now WB.
Would you have done something different?
We ended up doing this. Removed the lateral half of the screws and pushed the rest out using the screwdriver & II. Then inserted the bolts. Wanted to protect the knee so I inserted another advanced locker distally. The idea was they the first resistance would be the regular bolt, then the nail would migrate proximally to be held by the advanced locker at the end of the oblique hole and the distalmost screw.