INSTEAD OF WATCHING AN HOUR OF NETFLIX TONIGHT.
This 60-minute Cambridge lecture by Demis Hassabis will teach you more about the future of AI than most people will learn in the next 5 years.
Bookmark it and give it an hour, no matter what.
🔥 #EuroPCR 2026 Major Late-Breaking Trials: Long-term mortality following PCI with DES versus CABG for left main disease
An individual participant data meta-analysis of the SYNTAX, PRECOMBAT, NOBLE and EXCEL trials presented by Brian Bergmark showed no significant difference in all-cause mortality between DES PCI and CABG over 10-year follow-up in patients with left main coronary artery disease suitable for revascularisation.
Read the press release here: https://t.co/IWwgQBtbbU
@NievesGonzalo1@CuissetDr@nicolasdumonte1
#LeftMain #PCI #CABG #CoronaryArteryDisease #InterventionalCardiology #ClinicalTrials
4 A.M. STEMI call.
45-year-old male with acute anterior STEMI activated through the STEMI pathway.
Coronary angiography showed complete thrombotic occlusion of the LAD. Initial ballooning restored flow, and a drug-eluting stent was deployed successfully… or so we thought.
Seconds later came one of the true nightmares in interventional cardiology:
The stent was physically delivered. Deployment was confirmed.
But fluoroscopy showed… no stent in the lesion.
The LAD still looked unstented.
Immediate full fluoroscopic search of the patient’s body was performed. No lost stent was seen anywhere.
The table? Negative.
The sheath? Negative.
The guiding system inside the body? Negative.
Unfortunately, stent boost was unavailable at that moment, and IVUS was not accessible.
Multiple vigorous flushes of the guiding catheter failed to reveal the missing stent. At that point, the concern escalated dramatically — embolized stent? Lost in the system? Somewhere unseen?
Decision was made to retrieve the entire system and physically inspect everything outside the patient.
Still nothing.
Finally, as a last attempt, the guiding catheter was carefully cut in small external segments.
And there it was.
The entire undeployed stent was trapped inside the OUTSIDE portion of the guiding catheter — beyond the fluoroscopy field — firmly stuck despite repeated flushing attempts.
The relief in the cath lab at that moment was indescribable.
A new stent was then successfully deployed with excellent final angiographic result.
Lessons from the night:
• Never trust assumptions in the cath lab
• Lost stents can hide in unexpected places
• Systematic troubleshooting saves lives — and saves operators from panic
• Sometimes the solution is not high-tech… but persistence and careful thinking
Interventional cardiology continues to humble us.
#Cardiology #InterventionalCardiology #STEMI #PCI #CathLab #CoronaryIntervention #LAD #CardioTwitter #MedTwitter #STEMIPathway
#EuroPCR
💥 LM Perforation : a rare but catastrophic complication
Prevention Is Better ❗️
But When It Happens :
🚨Recognise it immediately
🚨The team must be there
🚨Remember to have covered stents in the lab
This is the first study to demonstrate the added value of #IVUS imaging on top of physiology-guided PCI with #PPG.
The impact appears greatest in focal disease, where imaging can further optimize PCI.
@crfheart@PCRonline
I would say that the KISS trial @JACCJournals not only proved that you do not need to do routine SB intervention (commonly kissing), rather I would say the most significant change is proving the concept of POT-side-POT (done in 57% of SB interventions and seems to be more favorable than kissing).
I have been recently doing POT-side-POT instead of kissing when I need SBI and that study proved it can be better!
Congrats to the authors and @sbrugaletta for an insightful editorial!
https://t.co/H3m2dHoufQ
#cardioX
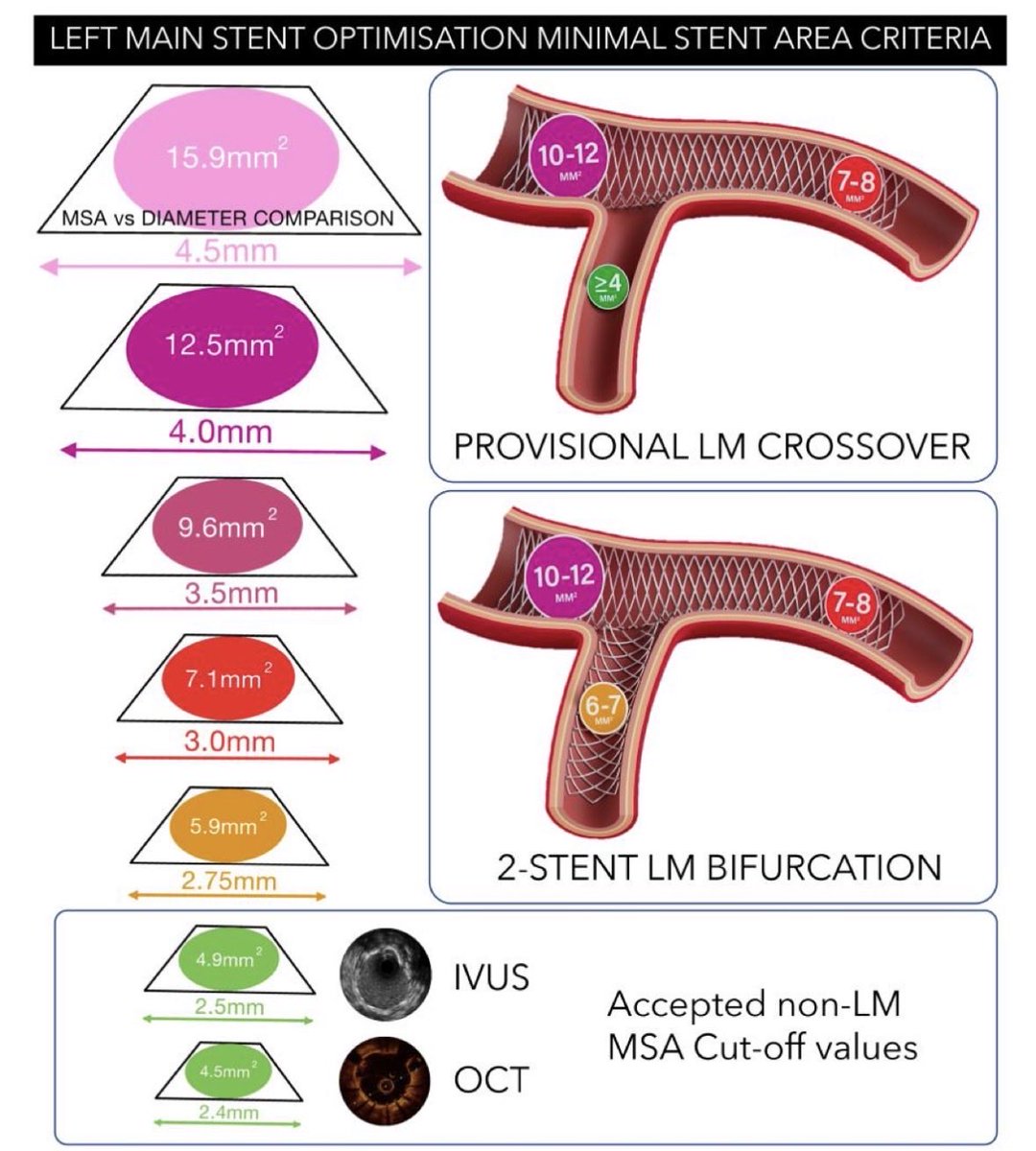
After 2 years of work, the 🇪🇺 consensus on #IVUS#OCT use in #LM#PCI is now published in #EHJ. Great international collaboration coordinated by #EBC and #EAPCI !!!
It includes fantastic practical images that can be hung on the walls of all cath labs…
https://t.co/2TbBTIoMxu
Burr entrapment, one of the most feared complications in rotational atherectomy. Multiple bailouts, choice driven by operator experience. Algorithms help organize the toolbox, especially for less experienced operators. My usual path: step (2) vasodilator + gentle pull (solves most), then (5) wire + balloon next to the burr or (6) knuckle wire for the resistant ones. With step (3), skipping rope, a newer iterative technique, I'll probably start following this more logical sequence.
#CHIP #Rotablator #RA #atherectomy #entrapment
In the DKCRUSH VIII trial comparing IVUS vs angiography for complex bifurcation lesions treated with 2-stent DK crush technique, benefits of IVUS-guided PCI at 1 year was achieved largely through achievement of IVUS-defined optimization targets https://t.co/AzsA7JXKtz
Welcome to the “skipping rope technique” for managing burr entrapment during rotational atherectomy, based on sequential counterclockwise rotational force is applied to the drive shaft, generating alternative torque dynamics https://t.co/sz8tj6y5my @ccijournal
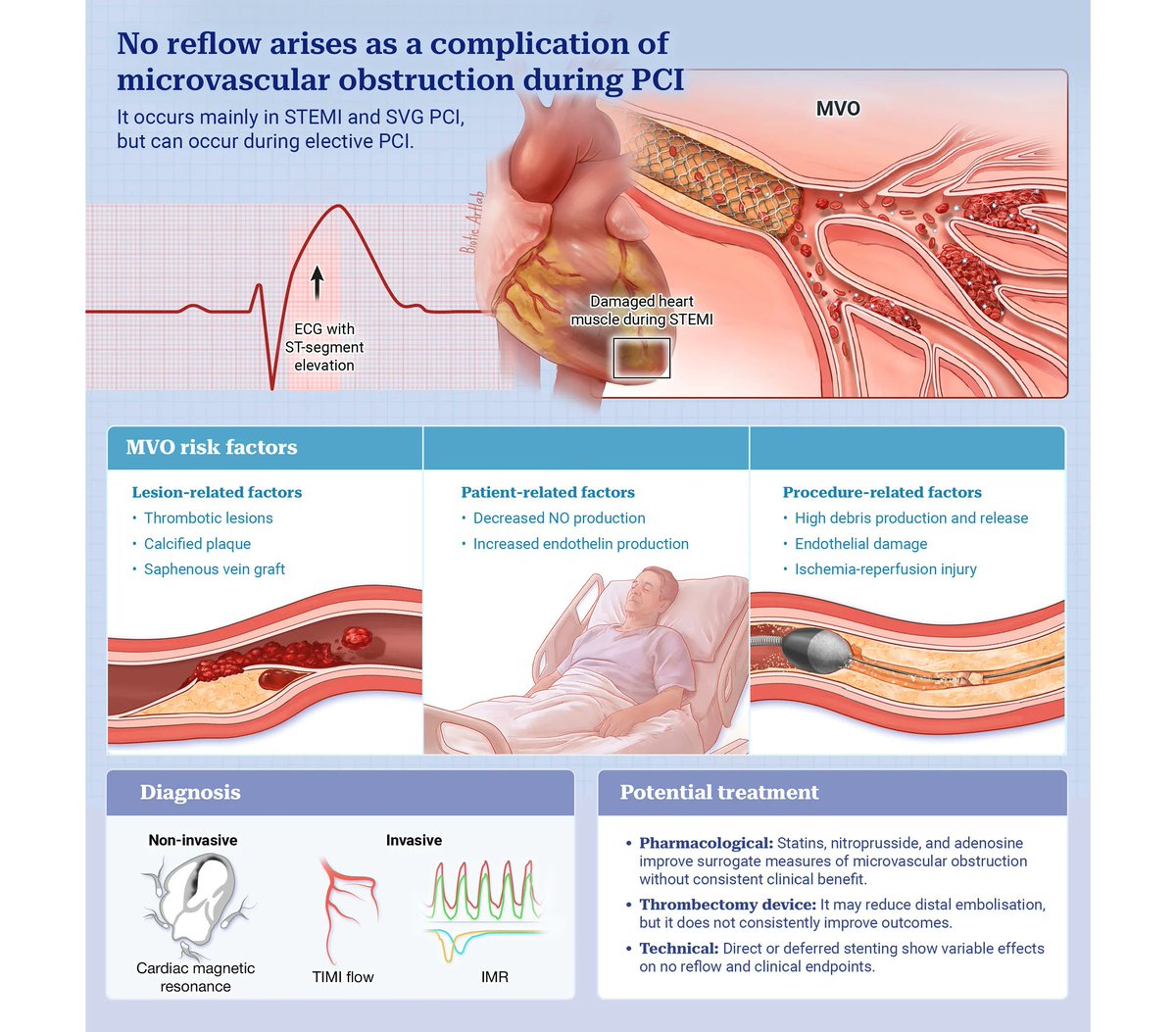
This state-of-the-art review provides a comprehensive overview of the pathophysiological mechanisms underlying the no-reflow/slow-flow phenomenon, covering invasive and non-invasive diagnostic tools, pharmacological and interventional treatment strategies, and the key clinical gaps that still need to be addressed in the field. https://t.co/glYW3u2X2z
A comprehensive expert review of NSTE-ACS, examining contemporary approaches to diagnosis, risk assessment, and early management, with practical insights into biomarkers, invasive strategies, and revascularisation pathways to support evidence-based clinical decision-making.
#Cardiology #NSTEMI #NSTEACS
https://t.co/7yy1BuOf7Y
@thiele_holger@gabrielsteg@VijayKunadian