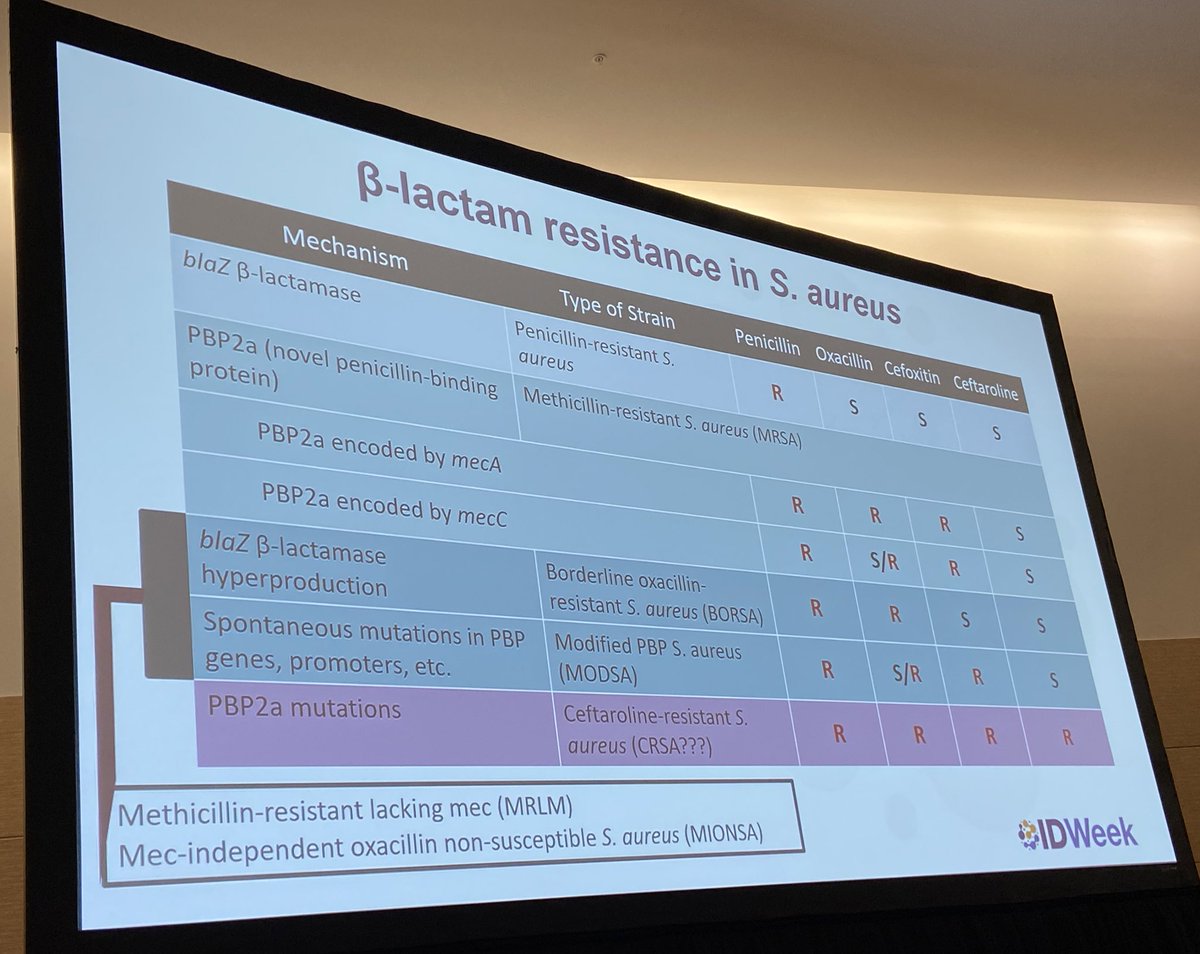
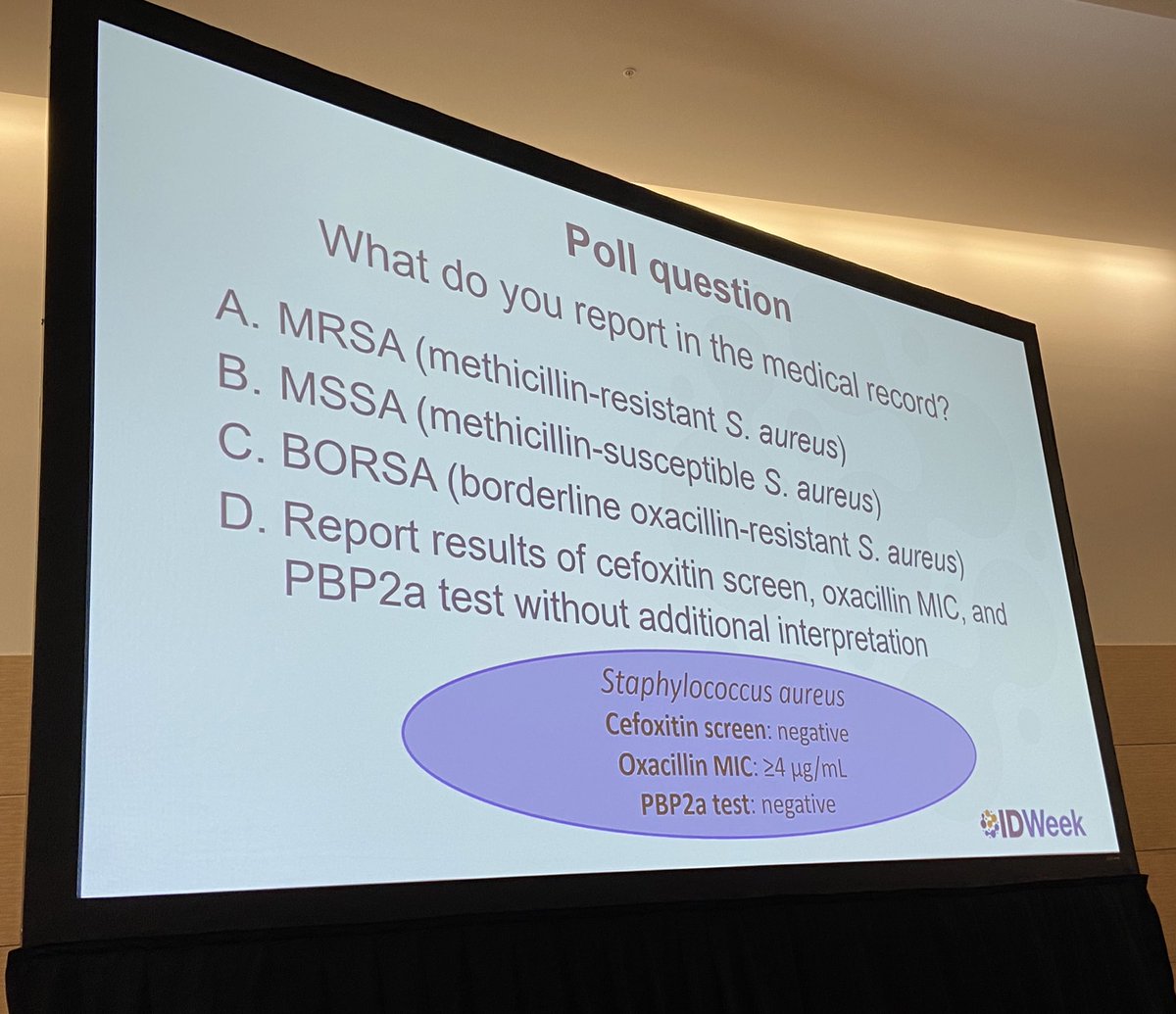
Great debate of what to do with mecA/PBP2A negative, oxacillin-resistant Staph aureus Cx results
A: Expert panel rec’s report & treat as MRSA, given highly elevated oxa MIC as opposed to BORSA that traditionally has MIC of 2 or less. Likely explained by blaZ #IDWeek2023
Think you know already know everything about beta-lactam resistance in Staphylococcus aureus? Think twice! In my commentary in #AACJournal I describe the hidden side of oxacillin resistance @ASMicrobiology https://t.co/LxJtD0gaBt
Kyle A. Hess, PharmD, BCPS - "All-In on Insulin? Use of High-Dose Insulin Euglycemic Therapy in Calcium Channel Blocker Overdose". Pharmacology CE available for pharmacists, physicians, physician assistants, and nurse practitioners. #TwitteRx@MayoMedEd
https://t.co/npRnH5YJiW
Publication Alert
Description of a case of S. aureus bloodstream infection and infective endocarditis with discordance between mecA/mecC genotypic results and phenotypic susceptibility testing. @omarabusaleh15@Stevens_AK
https://t.co/kV61fxVpa1
#IDTwitter will like this case, invoking conversations of BORSA/MODSA and the like.
What to do when genotypic and phenotypic testing don't align in Staph aureus?
Hot-off-the-press #AACJournal. Challenging Clinical Case on a patient with S. aureus endocarditis and discrepant mecA/mecC PCR. A rea therapeutic conundrum! @ASMicrobiology@asm_tmc
https://t.co/aavFhVl98U
One day @MayoClinicINFD Twitterless Dan DeSimone and I had a pt w/ persistent MSSA bacteremia on cefazolin and had an ox MIC of 2… we said “right right… the cefazolin shouldn’t be inferior to an ASP… we know the data… but what about the high ox MIC?”
https://t.co/MbES347rcz
🆕️⚡️⚡️#JCM@JClinMicro
Retrospective Evaluation of the Association of Oxacillin MIC on Acute Treatment Outcomes with Cefazolin and Antistaphylococcal Penicillins in MSSA Bacteremia #IDTwitter
https://t.co/bz3VEu5YWP
My PGY-1 research project just got published! Thankful for my amazing research mentors @Stevens_AK and @kjkpharm as well as all of @MayoClinicINFD! https://t.co/KjJPXlcN2F
Kyle A. Hess, PharmD @KyleHessPharmD - "Early Multimodal Vasopressors in Septic Shock: When is it Time for Full-Court Press(ors)?". Pharmacology CE available for pharmacists, physicians, physician assistants, and nurse practitioners. #TwitteRx@MayoMedEd
https://t.co/WGQQ2ZjHKo
@iamcrsmith@accpemedprn Here are a couple of additional studies you could take a look at if you are interested in the topic! Who knows how practice might change in the future: https://t.co/XDilkG0EHd, https://t.co/YgUwKDibrT
@iamcrsmith@accpemedprn I agree though, I have many doubts due to limitations of this trial (n = 40 in DOAC group, 0.6 mg/kg alteplase not used in US, no power calculation, retrospective design). I am definitely not ready to recommend lytics in my DOAC patients with AIS
Dr. Kyle Hess, EM PGY2 resident at Mayo Clinic will present on "Intravenous Thrombolysis with Alteplase at 0.6 mg/kg in Patients with Ischemic Stroke Taking DOAC" published this year in J Am Heart Assoc.
@GilbertPharmD Mayo Clinic will be recruiting for a Peds PGY2 this year with the amazing RPD @laurmargzpharmd! I’m an EM PGY2 but am happy to answer any questions about Mayo in general and have experience with many of our incredible Peds Preceptors!
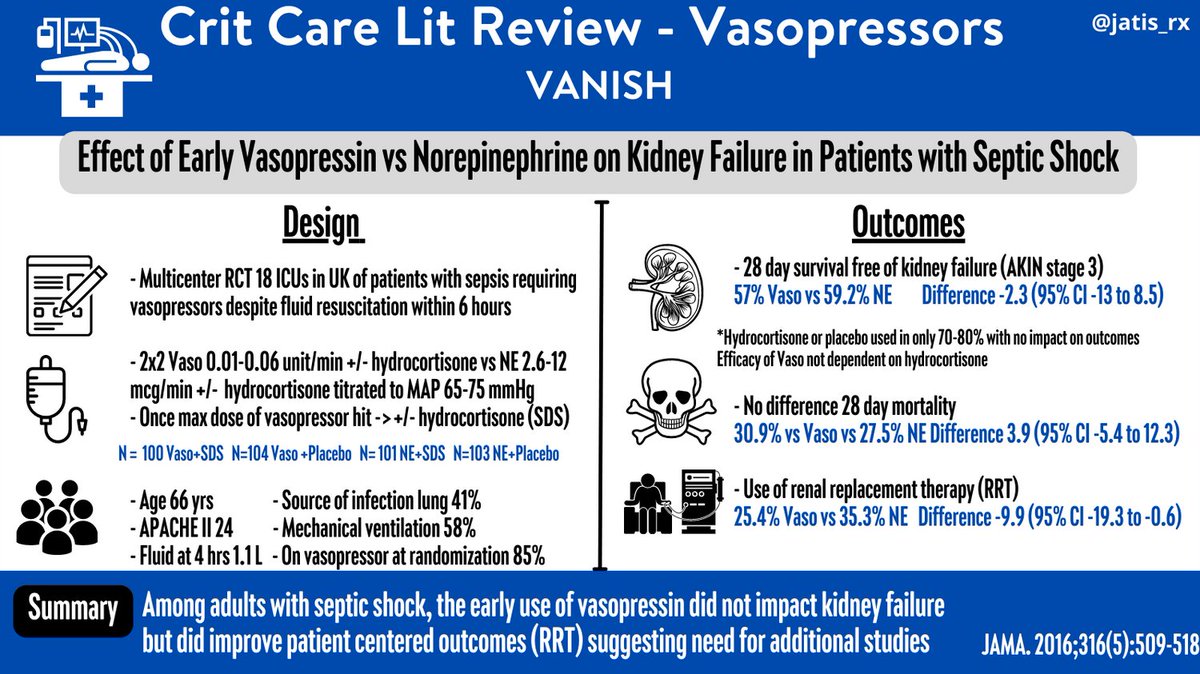
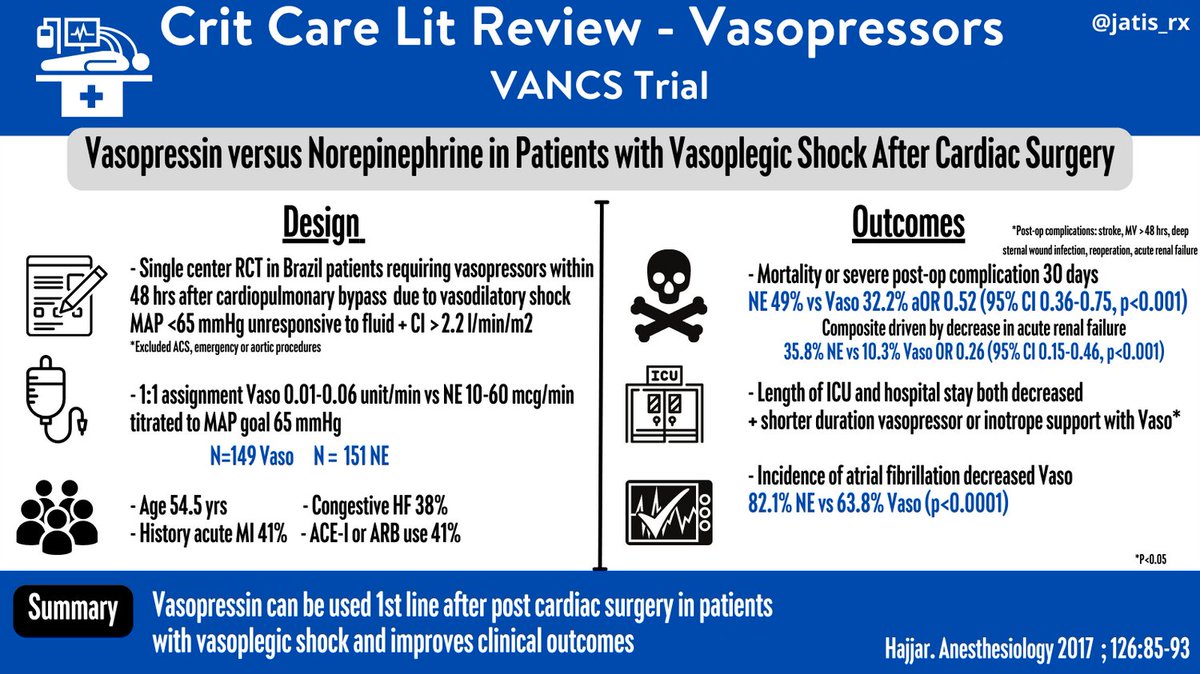
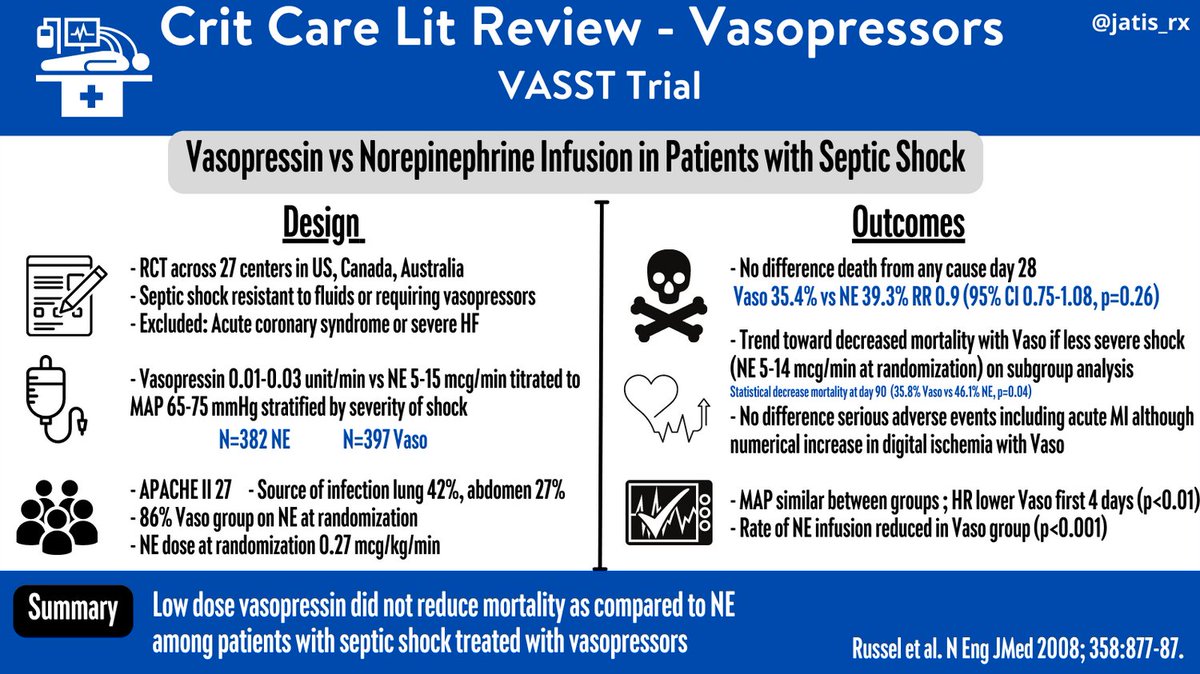
Crit Care Lit Review 📒 Vasopressin 💉
VASST: Adding vaso ⬇️catecholamine dose and may reduce mortality for those with lower NE dose (<15 mcg/min) in septic shock
VANISH: Adding vaso early to NE may ⬇️ need for RRT
VANCS: Vaso ⬇️acute renal failure in vasoplegic shock #PharmICU
I got to celebrate finishing my Grand Rounds on early multimodal vasopressors with a Squeeze Squad pin from @CuriousBoxwood! Thank you @pwierusz, @cassinetobacter, @AM_EM_PharmD, and Francis Manuel for all of your help in preparing for my presentation!