"Patient-reported Outcomes in Clinical Trials of Inflammatory Bowel Disease: A Systematic Review and Meta-analysis - Clinical Gastroenterology and Hepatology"
The study, published in @AGA_CGH was led by dr.Hanžel. We invite you to read the article: https://t.co/UuzZmeiCUj
Honored to host Dr. Ivo Boskoski, who visited us and demonstrated Gastric Mucosal Ablation (GMA) and Endoscopic Sleeve Gastroplasty (ESG) during a live case session. An excellent opportunity to learn from one of the leading experts in bariatric endoscopy.
@GI_UMCLJ@ukclj
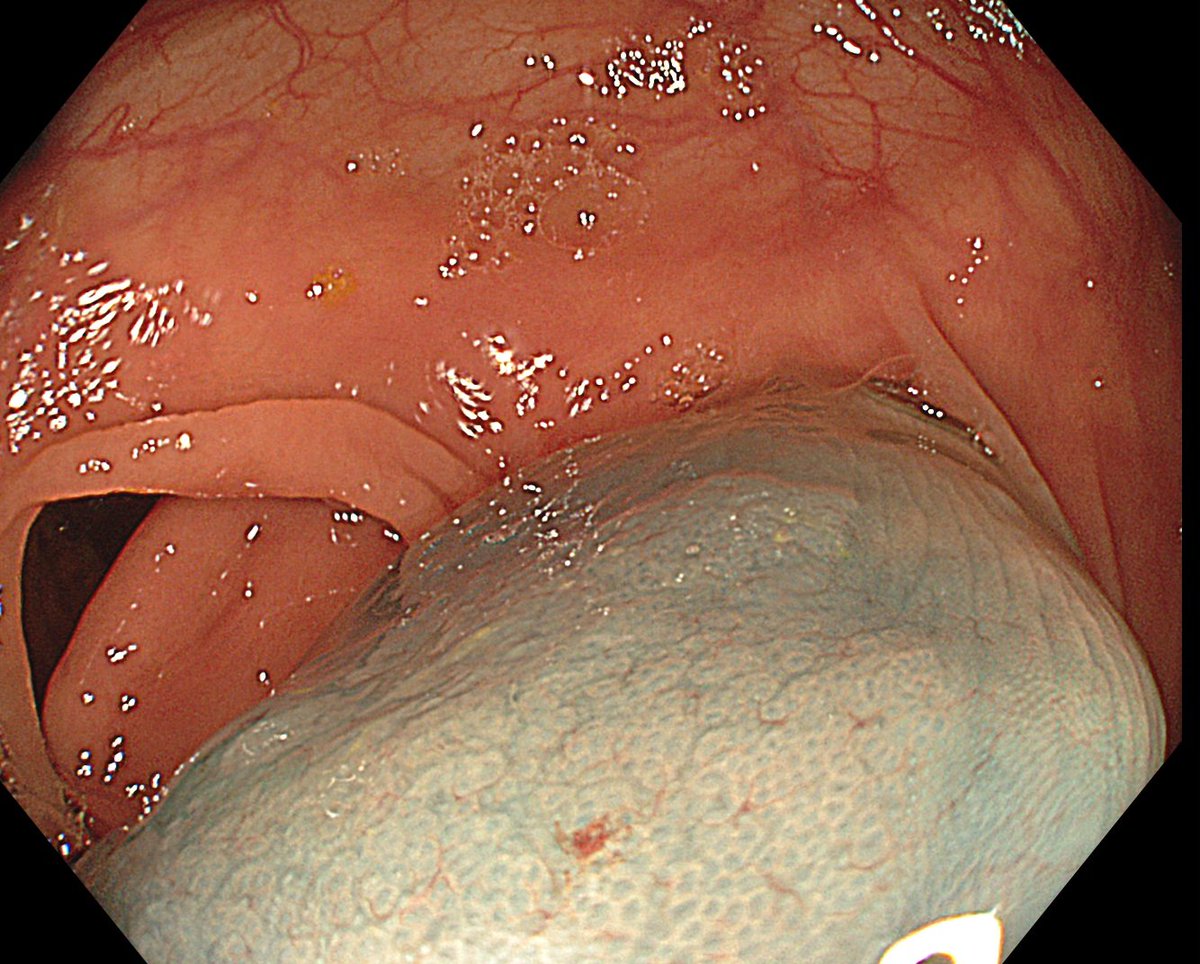
64F admitted in hemorrhagic shock. History notable for heavy NSAID use (6–8 tablets/day). After infusion/transfusion, she became stable enough for urgent EGD without intubation. CT showed no signs of perforation.
Ulcer shown below.
What would be your next step in management?
10min ERCP case in a 34 yrs-old female pt. (choledocholithiasis). 2 pancreatic duct wire passages. Pancreatic stent, sphincterotomy, stone removed.
18hrs later severe abd pain (pancreatitis). CRP 21. CT:few air bubbles around the duodenum.
Do you rescope and stent bile duct?
We have recruited 54 patients for the
Prospective Randomized Controlled Trial Evaluating Adenoma Recurrence after Endoscopic Mucosal Resection with Margin Marking or Post-Resection Treatment with Snare Tip Soft Coagulation (ERADICATE)
trial).
Went for cold pEMR.
The patient returned (12h) to the emergency unit with abdominal pain (pancreatitis).
This was periampullary lesion.
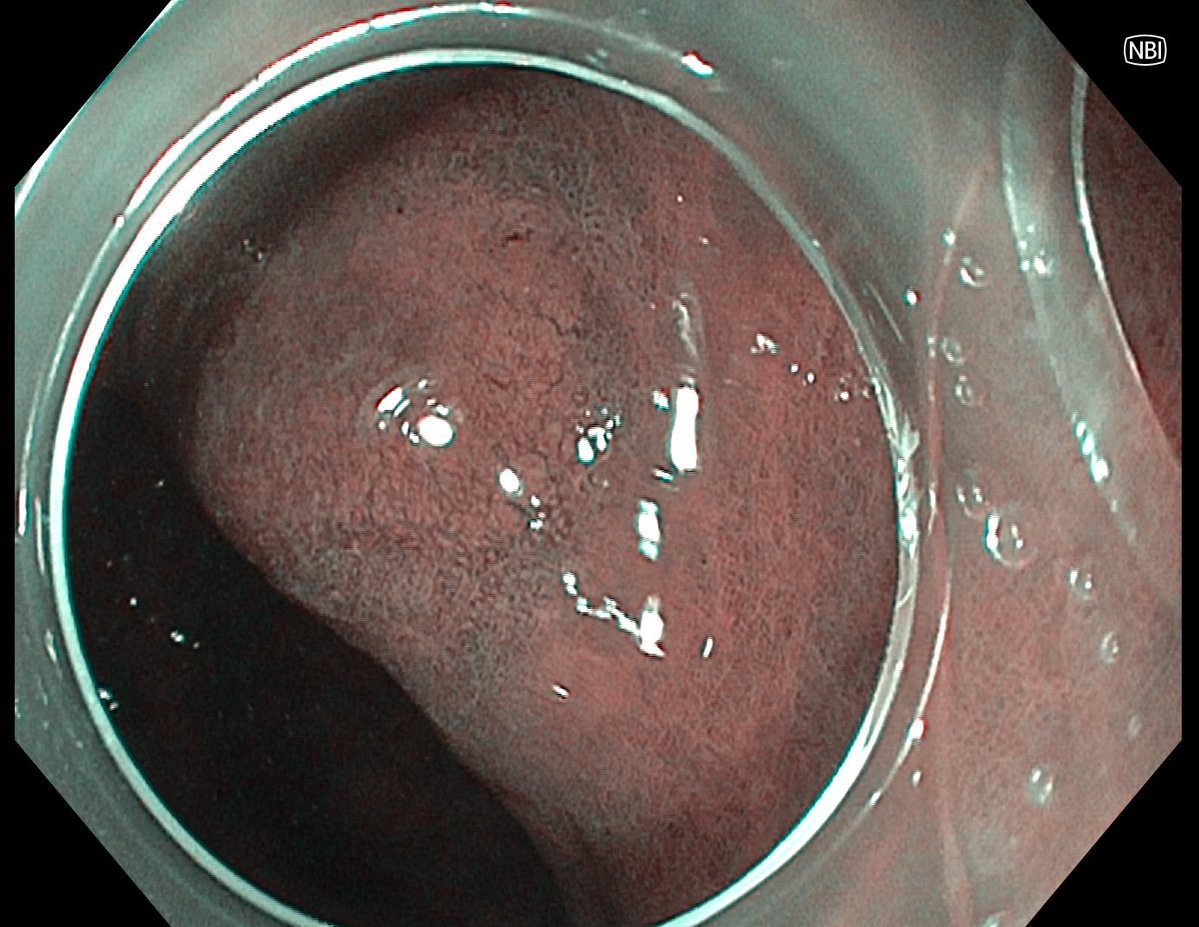
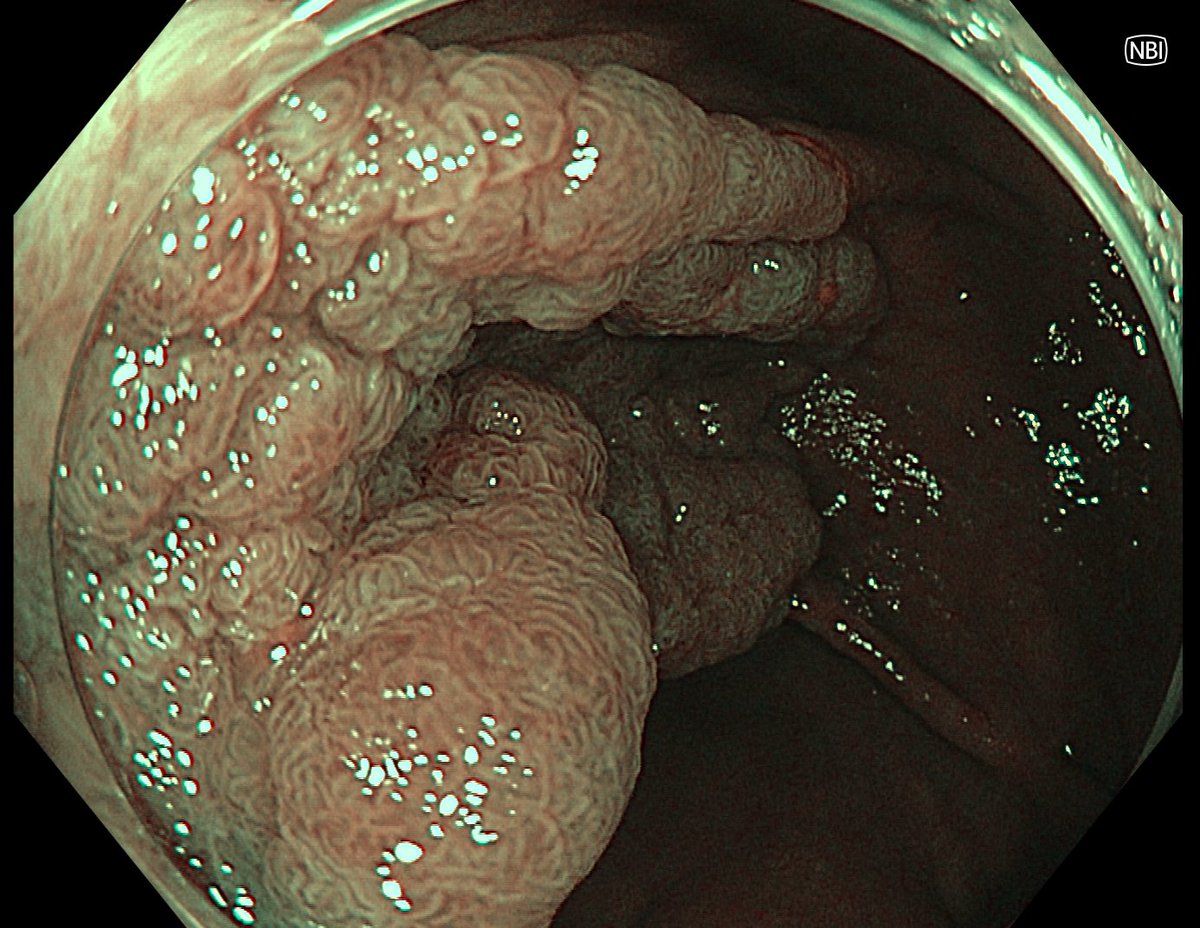
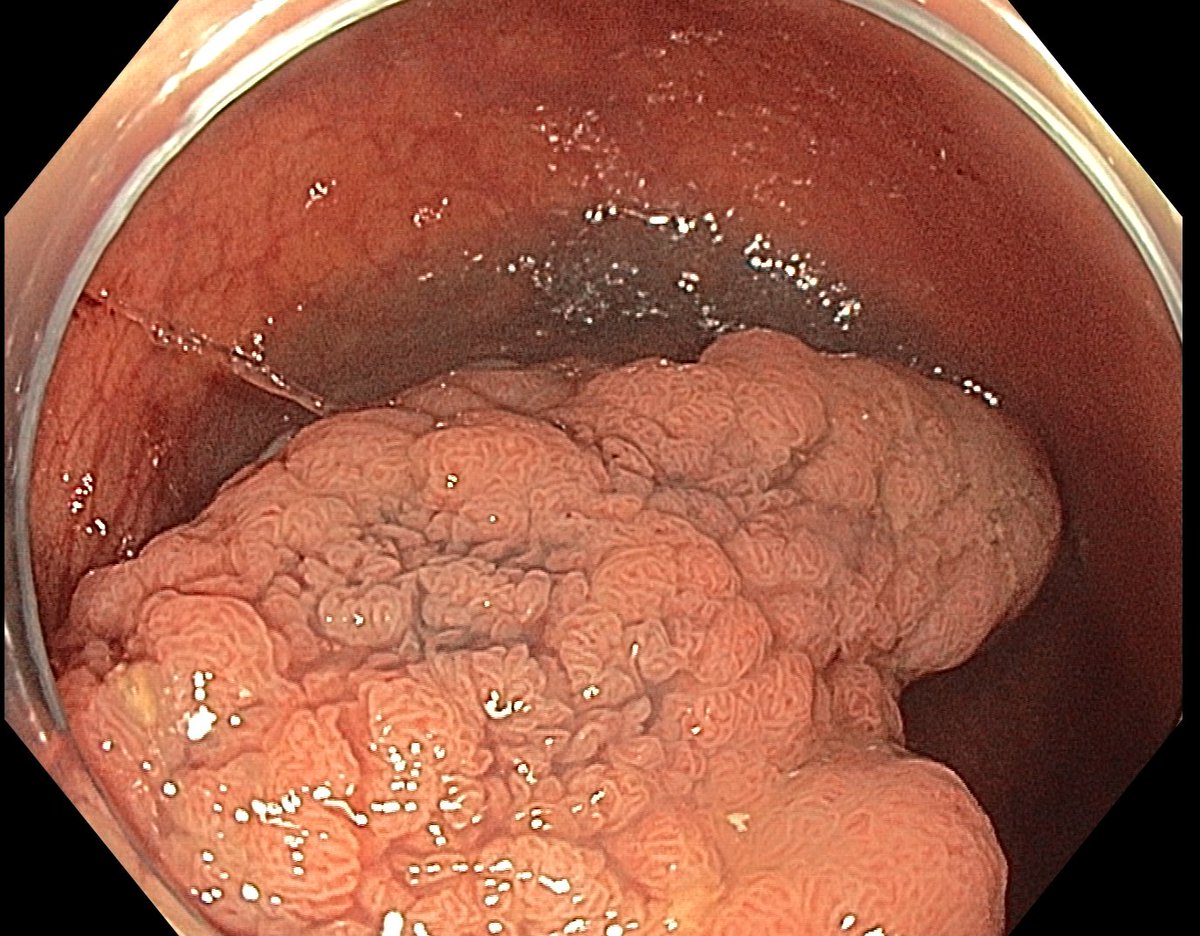
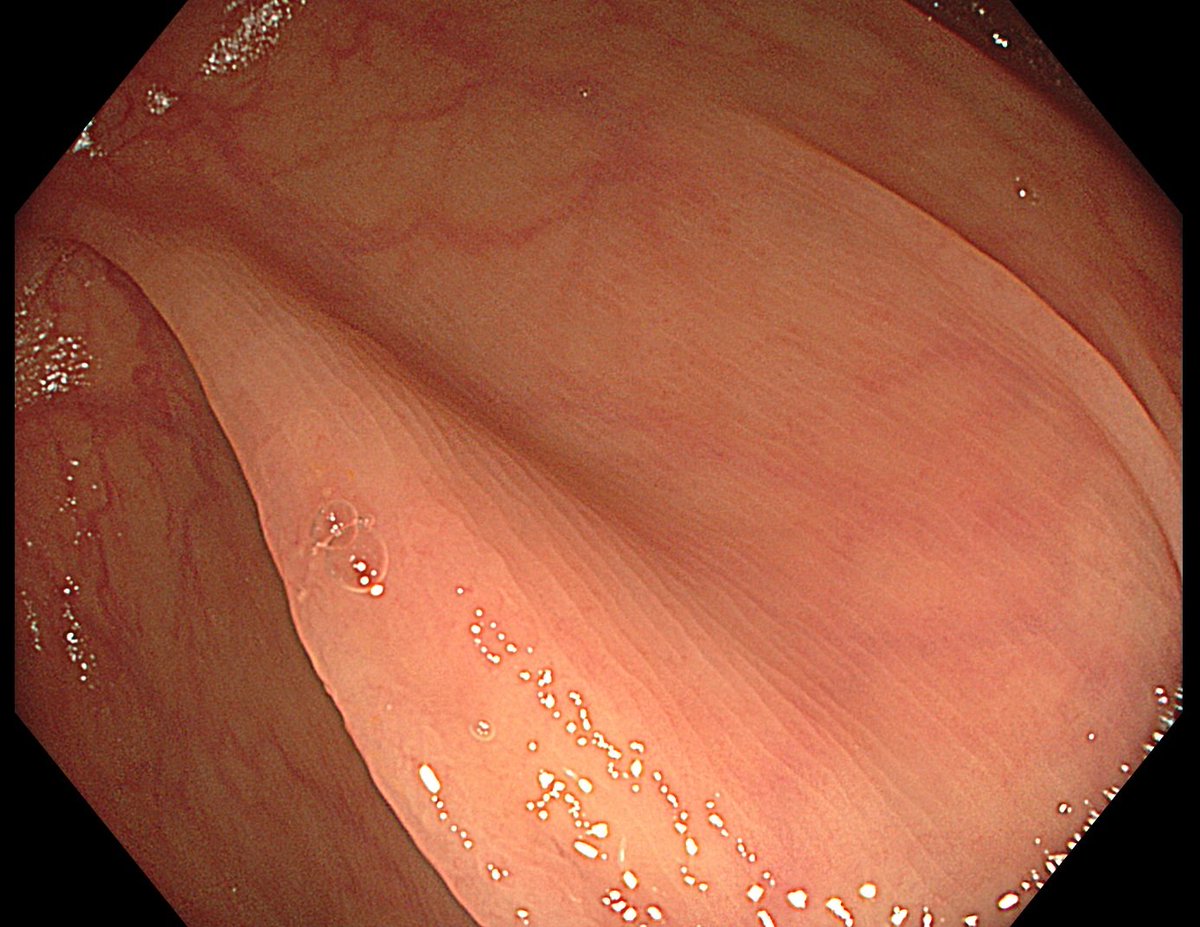
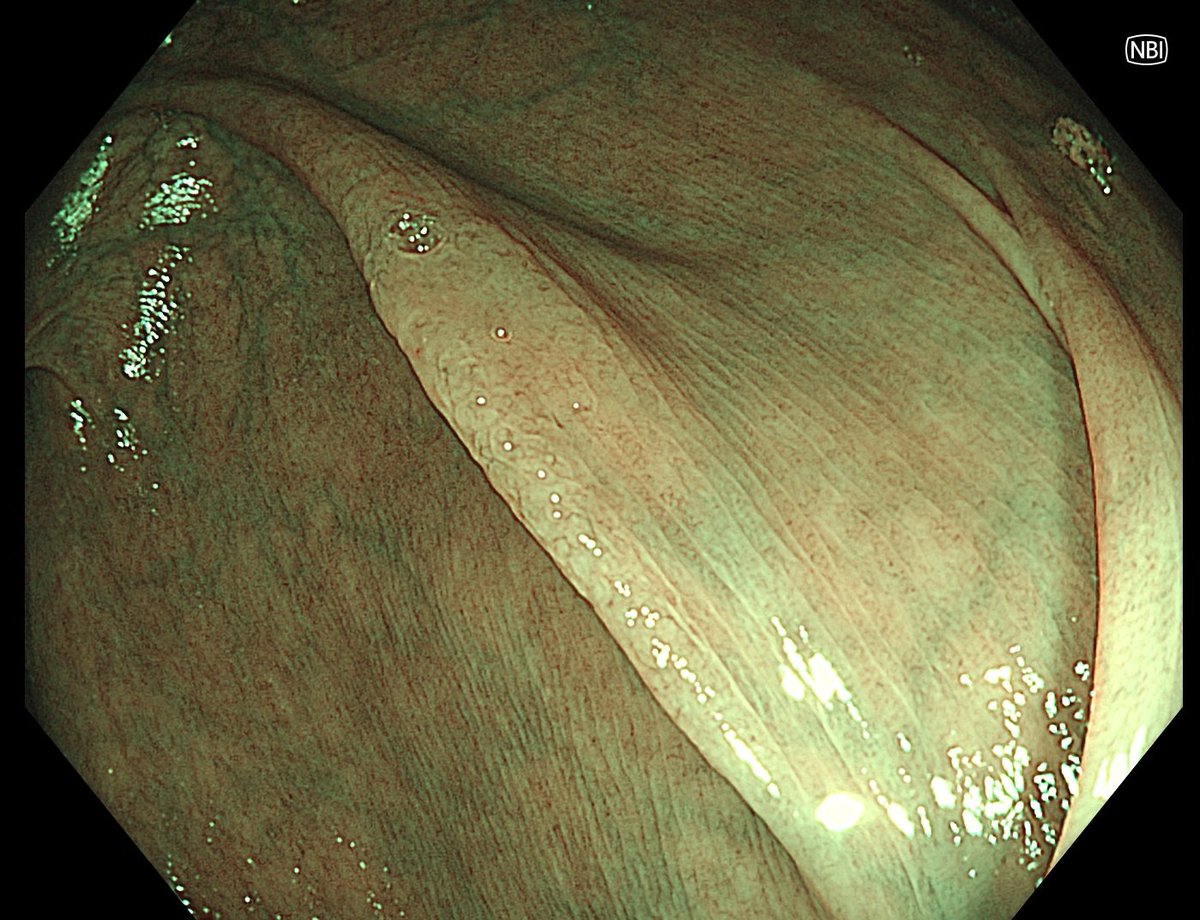
Basics: when dealing with polyps in this region, always confirm that the papilla is intact.
Images were obtained using prograde optics with a distal cap attachment.
Location: descending duodenum, approaching the horizontal (third) portion.
How would you remove this lesion? Any additional comments?
How would you remove this lesion?
20th patient recruited at @GI_UMCLJ@ukclj for a prospective cohort study: Cold Snare Endoscopic Mucosal Resection of Duodenal Adenomas >= 10mm.
@GavricAle@BilalMohammadMD
🚨 Advanced Endoscopy – Academic Opportunity at Baylor College of Medicine 🚨
We are excited to recruit two academically driven Advanced Endoscopists to support the expansion and restructuring of our Advanced Therapeutic Endoscopy program.
This is a unique opportunity to join a high-performing academic group and contribute to shaping the future of advanced endoscopy.
📍 Positions Available:
• One Advanced Endoscopist at Baylor St. Luke’s Medical Center / Woodlands campus
• One Advanced Endoscopist at Ben Taub Hospital
🎯 Who We Are Looking For:
• Recent graduates or early-career faculty (Assistant/Associate Professor)
• Strong foundation in EUS and ERCP
• Academic mindset with a track record or clear trajectory in research and publication
• Interest in becoming a future leader in academic gastroenterology
• Additional expertise or interest in bariatric or third space endoscopy is welcomed but not required
🔬 What We Offer:
A highly productive, innovation-driven academic environment:
• Dedicated Advanced Endoscopy practice (70–80%)
• State-of-the-art endoscopy unit (10 rooms)
• Robust research infrastructure:
– 4 full-time research assistants supporting IRB, study design, and grant preparation
• Strong clinical trials portfolio:
– 12+ ongoing trials
– 25+ completed clinical trials
• Proven academic productivity:
– Our team publishes 10–15 peer-reviewed publications annually
– Our team secures 3–4 grants annually
• Active presence at national and international meetings, including DDW
• Structured mentorship in advanced procedures and academic career development
• Dedicated training in grant writing, with opportunities to serve as PI on your own clinical trials
🌟 Why This Opportunity Stands Out:
• Baylor College of Medicine Gastroenterology is among the premier programs in the U.S., with a long-standing history of academic excellence and leadership
• Located within the Texas Medical Center, one of the largest and most innovative medical ecosystems globally
• Direct exposure to cutting-edge endoscopic innovation, with many novel technologies and procedures developed and trialed within our group
• Opportunities to collaborate with leading advanced endoscopists across institutions within the Texas Medical Center
• Active participation in the Texas Interventional Endoscopy Group (TXIEG | https://t.co/Uya4OHS1TV)
– Collaborative teaching platform for fellows, physicians, nurses, and technicians
– Involvement in premier hands-on workshops and advanced endoscopy courses
– Engagement in a broad, multidisciplinary network of advanced endoscopists across the region
📩 For inquiries or to refer candidates, please email me at:
[email protected]
"Twitter Endoscopy: A Mini Atlas of Gastric Dysplasia"
Here I share some of the dysplastic lesions referred for endoscopic resection at @GI_UMCLJ
1. Antrum, low grade dysplasia. Removed via ESD. Specimen 43x32mm / dysplasia 20x13mm. R0
Patient no.49 was recruited at @GI_UMCLJ@ukclj for ERADICATE trial.
The lesion was randomised to the margin marking before hpEMR.
@GavricAle@DennisYangMD
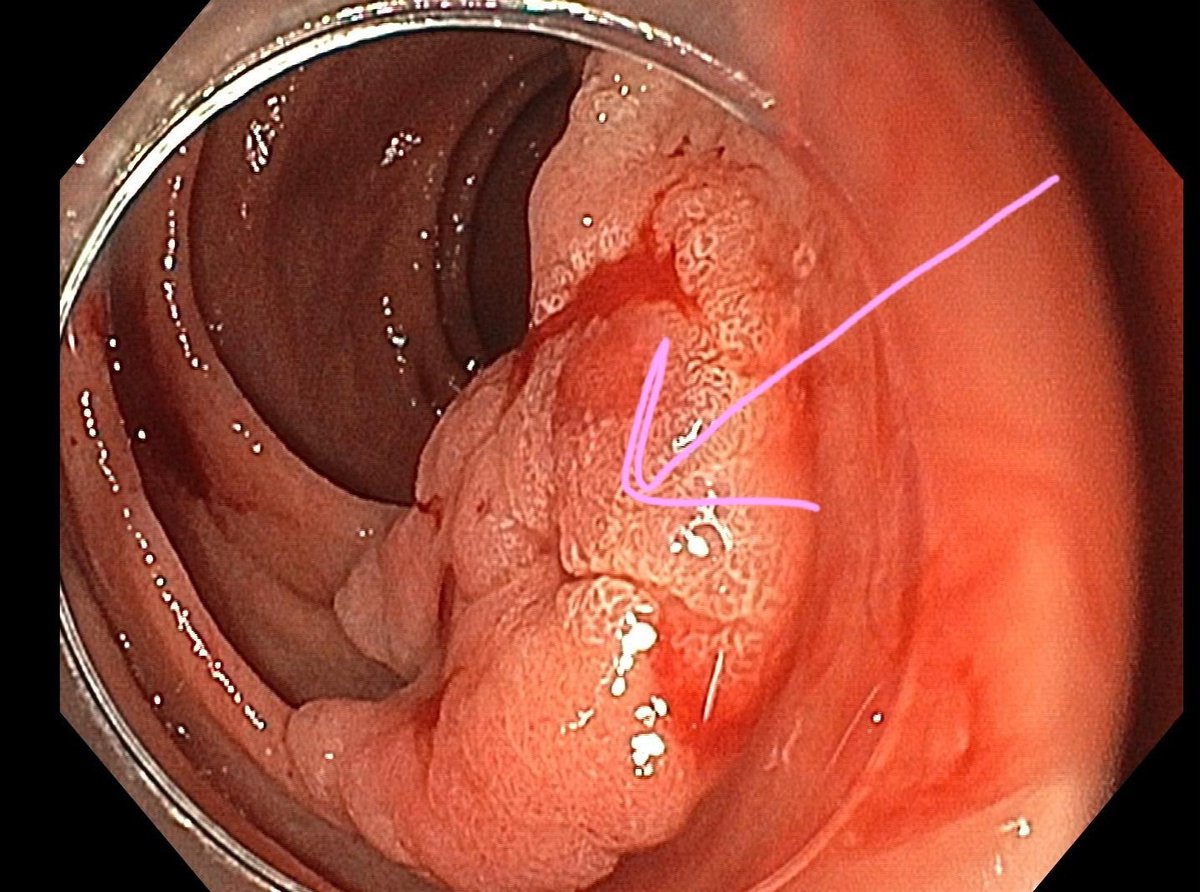
How to examine papilla with a distal cap-fitted gastroscope.
https://t.co/n0v4M60sIS
How do you examine papilla in patients with polyposis syndromes? Duodenoscope or gastroscope with a distal attachment cap?