@ElMonoGran42994 All current oral drugs for UC are absorbed systemically then distributed to other tissues including colon. Strict intestinal topical drug will have a hard time penetrate the mucosa & maintain a sustained PD.
$ADIL Unlike other AhR agonist, Indirubin has a polypharmacology where low concentration functions as AhR agonist then at a slightly higher concentration it becomes GSK3b inhibitor. Good luck.
@BiotechObserver@BenWil46805 Based on what I've heard these days, most institutions are laser focusing on safety signals in part 2. Ofc, safety is critical, but ultimately it's a risk reward compared to the current options e.g. Jaks.
@FidelisAurelius Moderately bullish. The readout is significantly overdue. The most likely outcome is Roche's Inavolisib failed to beat Aplelisib in a more powered trial. Probably already priced in, but it will be a readthrough to other PI3Ka-selective inhibitors in 2L ABC.
@BenWil46805 In ph2b study, 1/3 of those who didn't respond to 8-week obefazimod eventually achieved clinical *remission* if treated longer. The part 2 of ph3 has a similar nonresponder population. If data is good it will give doc much confidence obe is just a bit slower than biologics/Jaks.
$COGT ASCO data suggests Bezuclastinib + Sunitinib combo not only covered the exon 17/18 escape mutations (13mo vs 2mo), but also helped hit exon 11 harder. Note ~1/2 of GIST is KIT exon 11-*only* mutation.
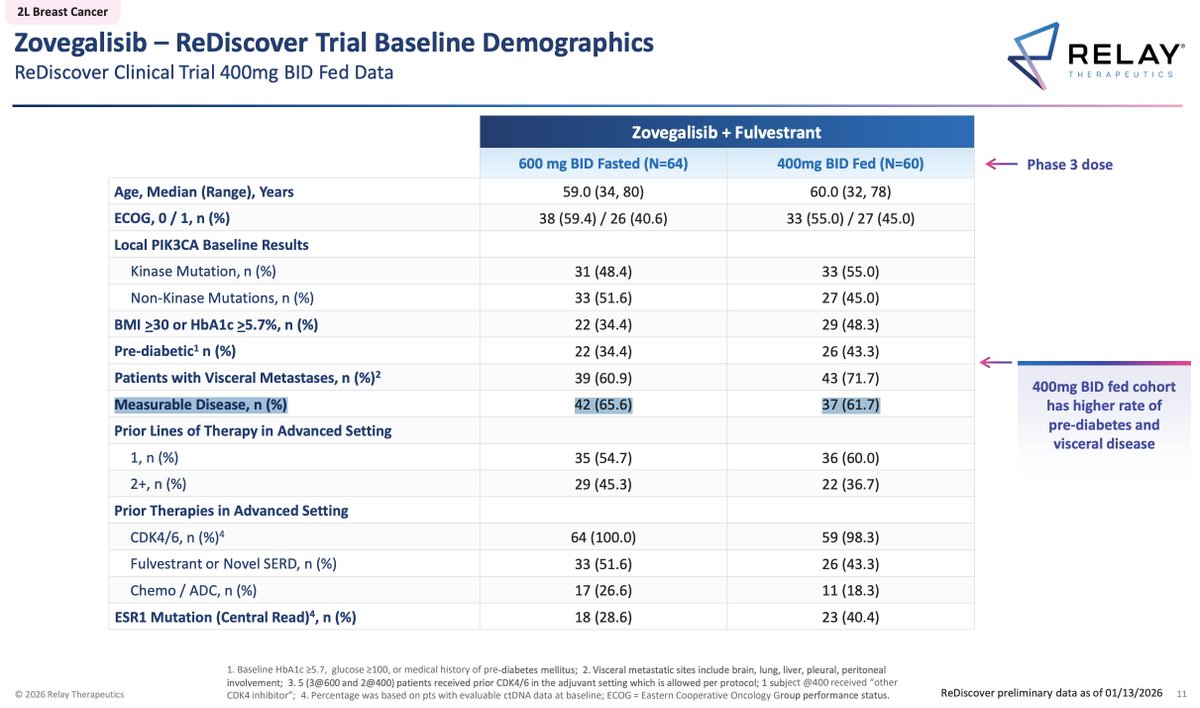
$RLAY Zovegalisib + Fulvestrant won't reproduce the 11mo PFS in phase 3. They included 40% bone-only disease in phase 1b which significantly inflated the performance.