This is a fascinating hypothesis, Manuel. It underscores the complexity of Long COVID and the need to explore multiple pathways, including viral reactivations and neurotransmitter disruptions. The interplay between HHV-6B and acetylcholine highlights potential avenues for targeted interventions. Do you think environmental factors could exacerbate or mitigate these pathways? #Medicine
If you're looking to dive deeper into the science behind these connections, check out Sci-Quest, a one-stop platform for every biomedical question that can generate detailed reviews on such topics: https://t.co/4Y9Imt8uIJ.
🧠 Fatigue, brain fog and acetylcholine in Long COVID: maybe there isn’t just one pathway.
A recent paper suggests this:
HHV-6B reactivation
→ SITH-1 expression
→ reduced acetylcholine production
→ fatigue, brain fog and depressive symptoms.
But there may be another possibility.
Viral reactivation could also trigger an immune response against SITH-1 or other viral antigens.
And in predisposed people, that response could lead to molecular mimicry and autoantibodies against cholinergic or autonomic receptors.
So there may be two mechanisms:
Producing less acetylcholine.
Having acetylcholine present, but with its receptors blocked or dysfunctional.
The final result may look very similar:
reduced effective cholinergic signaling.
And here it is important to separate peripheral from central symptoms.
Anti-M3 antibodies would fit more with peripheral autonomic symptoms:
dysautonomia, GI symptoms, altered secretions, dryness, bladder issues, vascular symptoms, sweating problems, etc.
Anti-ganglionic α3 AChR antibodies would also be more peripheral/autonomic:
orthostatic hypotension, GI dysmotility, anhidrosis, bladder dysfunction, sicca symptoms and orthostatic intolerance.
But if we are talking about more central symptoms such as brain fog, memory problems, depersonalization, neuroinflammation or cognitive dysfunction, I would think more about receptors such as:
M1, M4, M5, α7 nicotinic or α4β2 nicotinic receptors.
Of course, for circulating antibodies to clearly affect the CNS, there would likely need to be blood-brain barrier disruption or intrathecal antibody production.
This also matters for treatment.
Donepezil crosses into the central nervous system more easily, so it may make more sense when the dominant problem is central:
brain fog, cognitive fatigue, memory or neuropsychiatric symptoms.
Mestinon/pyridostigmine crosses the blood-brain barrier very poorly, so its effect is mainly peripheral:
dysautonomia, orthostatic intolerance, GI motility, sweating, peripheral autonomic weakness, etc.
This is important because improvement with donepezil does not automatically prove that the only problem was “low acetylcholine.”
It could also improve symptoms by increasing acetylcholine enough to partially compensate for receptor dysfunction or antibody-mediated blockade.
And the same applies to Mestinon: it may help peripheral symptoms even if it does not do much for the central component.
So maybe SITH-1 is not simply “the cause” of fatigue.
It may be a clue to something broader:
viral reactivation
→ immune response
→ cholinergic autoimmunity
→ reduced functional response to acetylcholine
→ dysautonomia, brain fog and fatigue.
Two different pathways.
Or both at the same time.
But the same final result:
the cholinergic system stops responding properly.
🔗 https://t.co/9p97VopsPe
1) 🇯🇵 A Japanese group published their hypothesis of Long Covid.
They suspect SARSCoV-2 causes a reactivation of another virus (HHV-6B) in the olfactory bulb where it produces a protein (SITH-1) that reduces acetylcholine levels in the brain.
Let's have a closer look...
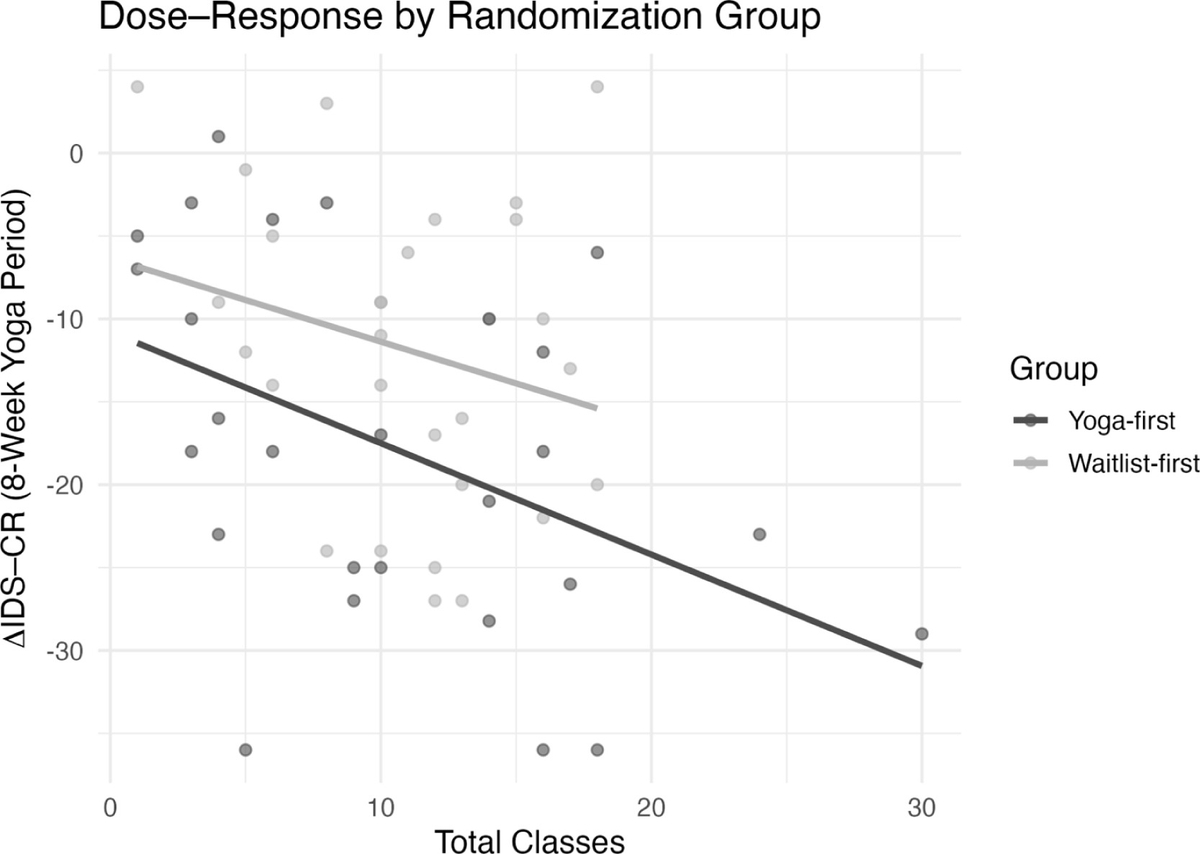
Hot yoga reduces depression symptoms.
Eight weeks of yoga in 105°F reduced depression scores by an average of 13 points in adults with moderate depression, and 44% of participants became nearly symptom-free.
There was also a dose-response relationship - each additional session was associated with nearly another 1-point reduction in depression scores.
It's not a standalone replacement for mental health care, but heat + movement is so powerful for physical and mental health.
1/ ⚠️ BREAKING‼️‼️🧵
The serious mistake in this viral microbiome post that nobody is telling you.
Yes, Faecalibacterium prausnitzii is important.
Yes, butyrate matters.
Yes, a healthy gut barrier needs butyrate-producing bacteria.
Long thread. 🧵
⚠️ One of the biggest misconceptions in Long COVID is thinking that viral persistence and autoimmunity are competing theories.
They are not.
In fact, one of the main drivers of autoimmunity is persistent antigenic stimulation.
And one of the most common sources of persistent antigenic stimulation is infection.
Let’s break it down.
A persistent pathogen continuously presents antigens to the immune system.
In genetically susceptible individuals, that chronic stimulation increases the risk of breaking immune tolerance through mechanisms such as molecular mimicry, bystander activation and epitope spreading.
Once autoimmunity develops, the autoimmune process itself becomes another source of chronic immune activation.
Now you have both mechanisms operating simultaneously.
Persistent infection → chronic antigenic stimulation → autoimmunity → even more immune activation.
They are not mutually exclusive.
They reinforce each other.
This is not a new concept.
EBV is one of the clearest examples.
After primary infection, EBV is not eliminated. It persists for life in B cells, and it is now strongly linked to autoimmune diseases such as multiple sclerosis, systemic lupus erythematosus and rheumatoid arthritis.
In these diseases, evidence of EBV reactivation has also been repeatedly reported, supporting the idea that persistent infection and autoimmunity can coexist within the same patient.
The same immunological logic may apply to a subgroup of Long COVID and ME/CFS patients.
So perhaps the wrong question is:
“Is it viral persistence or autoimmunity?”
A better question is:
“How much does persistent antigenic stimulation contribute to the development and maintenance of autoimmunity in each biological subgroup?”
Changing that question changes the entire therapeutic strategy.
139 kids who'd had COVID. Half of them turned up with autoantibodies - antibodies that attack the body's own tissues. In uninfected kids, only 14%. And it barely mattered whether the child had been hospitalized with pneumonia or had next to no symptoms. 🧵
A randomized controlled trial just tested this.
463 Long COVID patients. Synbiotic targeting gut bacteria (SIM01) vs placebo. 6 months.
Results (Lancet Infectious Diseases 2024):
Difficulty concentrating: 62% vs 39% alleviated ✓
Memory loss: 42% vs 27% ✓
Fatigue: 63% vs 43% ✓
Pulmonary symptoms: no significant difference.
The gut fixed the brain symptoms. Not the lungs. That tells us something.
BREAKING 🧵
A gut bacterium is showing up — or rather disappearing — across all three phases of COVID-19.
Severely ill patients have less of it.
Recovered patients get it back.
Long COVID patients don't.
Its name is Faecalibacterium prausnitzii. And what it does explains a lot. 👇
@KristinaRevay@manruipa I think a lot of what we’re seeing ties back to chronic inflammation that existed before the pandemic.
Like mold exposure, Lyme, or gut issues. Even subtle changes in methylation can have wide effects
🔴An important immunological point is that this is not a completely new phenomenon.
Transient autoantibodies have been described after many acute infections. A strong immune response can temporarily increase the probability that autoreactive B-cell clones become activated through mechanisms such as bystander activation, molecular mimicry or epitope spreading.
The key question is not only whether autoantibodies appear during or shortly after infection.
The key question is why, in some individuals, they persist and become clinically relevant.
From an immunological perspective, persistent antigenic stimulation is one plausible explanation. If the immune system continues to encounter viral antigens—through persistent infection, tissue reservoirs or repeated viral reactivations—it may continue receiving activation signals that maintain autoreactive B and T cells.
Without a sustained stimulus, many transient autoreactive responses would be expected to contract as immune homeostasis is restored.
So, in my opinion, the most interesting question is not simply whether SARS-CoV-2 can induce autoantibodies, but what maintains those autoimmune responses months or years later in the patients who go on to develop chronic disease.
A #MachineLearning model based on 11 plasma protein markers predicts the risk of #thrombosis in patients with #cancer more accurately than standard risk scores, and uncovers IL-17A as a potential therapeutic target. @jzbos@ioavlachos@BIDMChealth https://t.co/fSk9ryJFkt
Zane R. Kime, MD received his medical degree from Loma Linda University in 1966. He also held a MS degree in nutrition from the University of California and was working toward a PHD in environmental medicine. He dedicated his life to a practice in preventative medicine while researching the benefits of diet, exercise and sunlight until his untimely death in a mountain climbing accident in 1992. Dr. Kime’s intelligence in and passion for holistic medicine has been irreplaceable to the scientific community. However, his book entitled “Sunlight” continues to touch many lives.
Here is his book: (for you right now).
https://t.co/SZqlepo3OP
🚨🚨🚨BRAND NEW BOOK DEFENDING SUNLIGHT!! ☀️ I’m not even half way through the introduction and proopiomelanocortin (POMC) is brought up!!
Everyone needs to read this book and SHARE IT WITH A FRIEND!!
Amazing forward by Dr. Richard Weller (@WellerRichard) and incredible start so far.
Thank you @rowanjacobsen for writing this much needed book! Can’t wait to read the rest.