Rebound pain after peripheral nerve block
Pre-emptive opioids were not shown to offer meaningful benefit and, based on current evidence, appear to be the least effective among the drugs evaluated.
@SinghNP_23#anaesthesia#regionalanaesthesia#regionalanesthesia#MedTwitter
https://t.co/409AiHrTtd
Sub 60 🥳
Setelah analisa, kelemahan saya di aerobik base dan otot kaki kanan (post acl surgery) dan kekuatan vo2max + form lari udh bisa high speed. Target pelan2 tercapai, dan fokus latihan zona 2 dan strength training dibanyakin. Onto the next target
first 15 km, I ran with a bit of knee pain and sometimes had to contract and release my quadriceps. It’s at least improved since yesterday. Keep going ltr
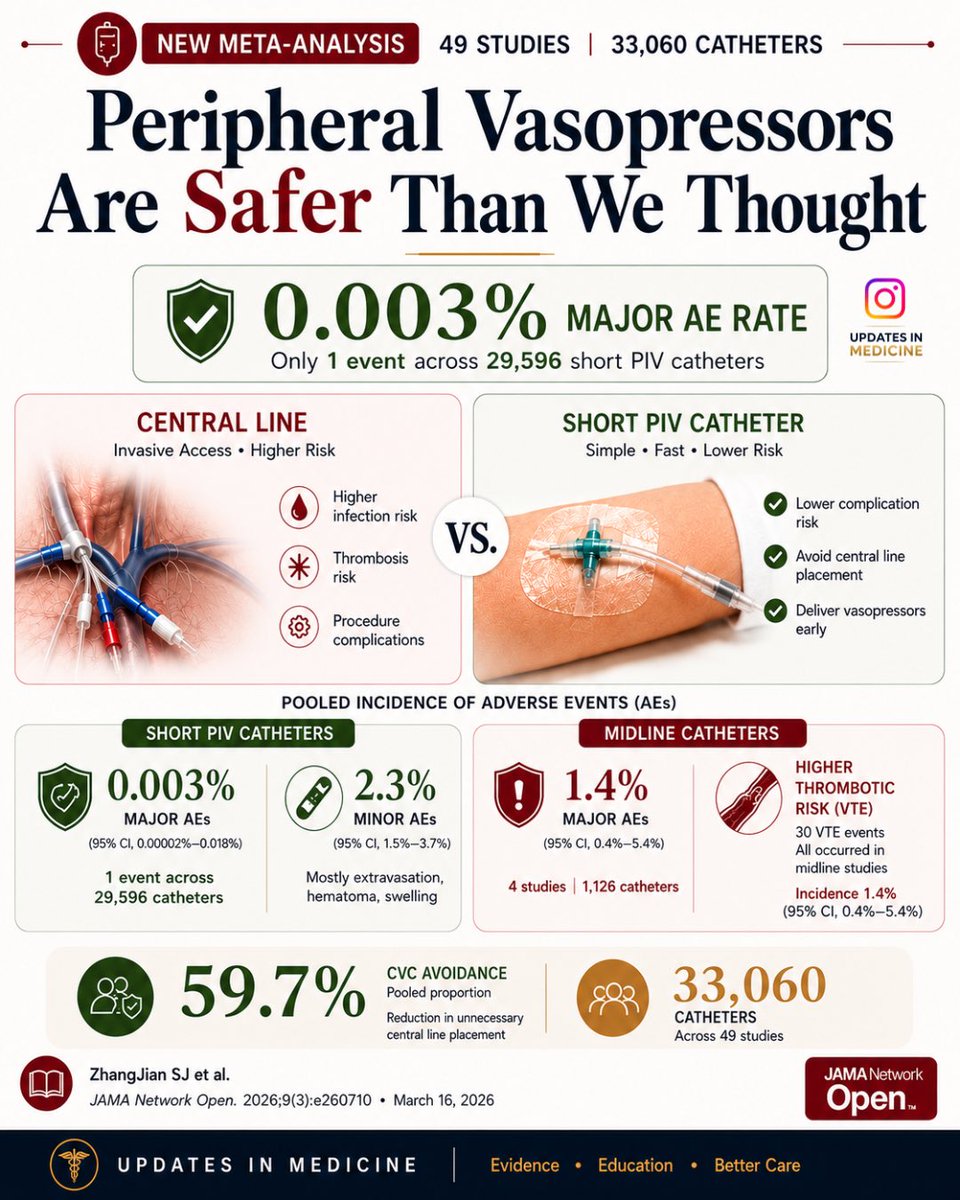
Peripheral vasopressors may be safer than we thought — only 1 major adverse event across 29,596 short PIV catheters in this meta-analysis of 49 studies.
🫁 Lung Ultrasound 2.0, From Art to Science
The new international consensus on lung ultrasound marks a clear transition:
👉 From qualitative interpretation
➡️ To standardized, reproducible, and quantitative medicine
⚠️ What is truly NEW in this update
🔴 1. Standardization is now mandatory, not optional
LUS is highly operator- and machine-dependent
👉 The same patient can generate different findings depending on settings
New recommendation:
• Always report probe, frequency, MI, depth, protocol
• Move toward reproducible imaging frameworks
🧠 2. B-lines are no longer “simple artifacts”
They are:
• Frequency-dependent
• Physically complex
• Linked to lung microstructure
👉 Counting B-lines is semi-quantitative at best
➡️ Future: quantitative ultrasound spectroscopy
🤖 3. AI enters LUS, but with caution
AI is emerging in:
• Image segmentation
• Severity scoring
• Pattern recognition
BUT:
👉 Strong warning against overinterpretation and poor methodology
Key requirement:
• Proper dataset splitting
• Standardized acquisition
• Clinical validation
⚙️ 4. Multidisciplinary shift
This is not just a clinical update
👉 Engineers + physicists are now part of the consensus
Why?
• Ultrasound physics matters
• Signal processing matters
• Image formation matters
➡️ LUS is now a true bioengineering field
📊 5. From subjective to objective metrics
Major gap identified:
• Pleural line abnormalities
• Subpleural consolidations
• Artifact interpretation
👉 Need for:
• Measurable parameters (mm, not “small/large”)
• Quantitative imaging endpoints
🛑 6. Safety is finally addressed
New concern:
👉 Potential pulmonary capillary hemorrhage (animal data)
Recommendation:
• Apply ALARA principle
• Monitor Mechanical Index (MI)
• Limit exposure time
➡️ LUS is safe, but not risk-free
📚 7. Education becomes a core pillar
Clear statement:
👉 LUS must be formally taught and standardized
Including:
• Medical curriculum integration
• Structured training
• Remote mentoring
🎯 Take-home message
Lung ultrasound is evolving from:
❌ Operator-dependent bedside tool
✅ Standardized, physics-driven, AI-supported diagnostic modality
⚖️ My reflection
We are entering a phase where:
👉 Understanding how ultrasound interacts with lung tissue
is as important as interpreting the image itself
This is where critical care, cardiology, and engineering finally meet
📖 Libertario D et al J Ultrasound Med 2023
doi:10.1002/jum.16088
#LungUltrasound #CriticalCare #POCUS #MedicalAI #ICU #Ultrasound #PrecisionMedicine #ACVC