Having back pain and a history of malignancy is not automatically a red flag.
Pay attention. Ask important questions. Elaborate.
What type of cancer? What is the current status of care? What is the temporal nature of the pain? What is their general health like? How are they sleeping? Any weight loss? Is it explainable? Over what time frame? Any fevers? Any other systemic symptoms?
A history of malignancy should raise your index of suspicion, not switch off your clinical reasoning.
We shouldn't be escalating, acting defensively, or automatically imaging based on a piece of information on paper alone. Don't let your brain fall out.
Testing ankle inversion & eversion for suspected L4, L5 radiculopathy, fibular (peroneal) mononeuropathy etc is finickety at the best of times.
Particularly when trying to perform it in sitting & trying to grade it.
Here’s a simple way to remember:
Push opposite, support same:
➡️ Eversion → push outside, support inside
⬅️ Inversion → push inside, support outside
Here’s me testing anke inversion in supine, simple set-up, with a bit of physical prompting to help guide the movement.
For those like me heading into work for a day of MSK triage, remember this. Most of what you will see is non specific, variable, and hard to slap a diagnostic label on. Your scan results will often be equivocal and you will not be able to provide certainty to your patients based purely on a pathoanatomical model. And you know what? That is ok.
It is real life, real people, real complexity. Not everything is knowable and your patients are not from a textbook. If it does not fit, do not try to make it fit. Be honest, communicate, and manage expectations. Do not feel you must always meet or exceed them.
You are human too and we do not have this stuff figured out. Not by a long shot.
Have a great day. Breathe. Drink coffee ☕
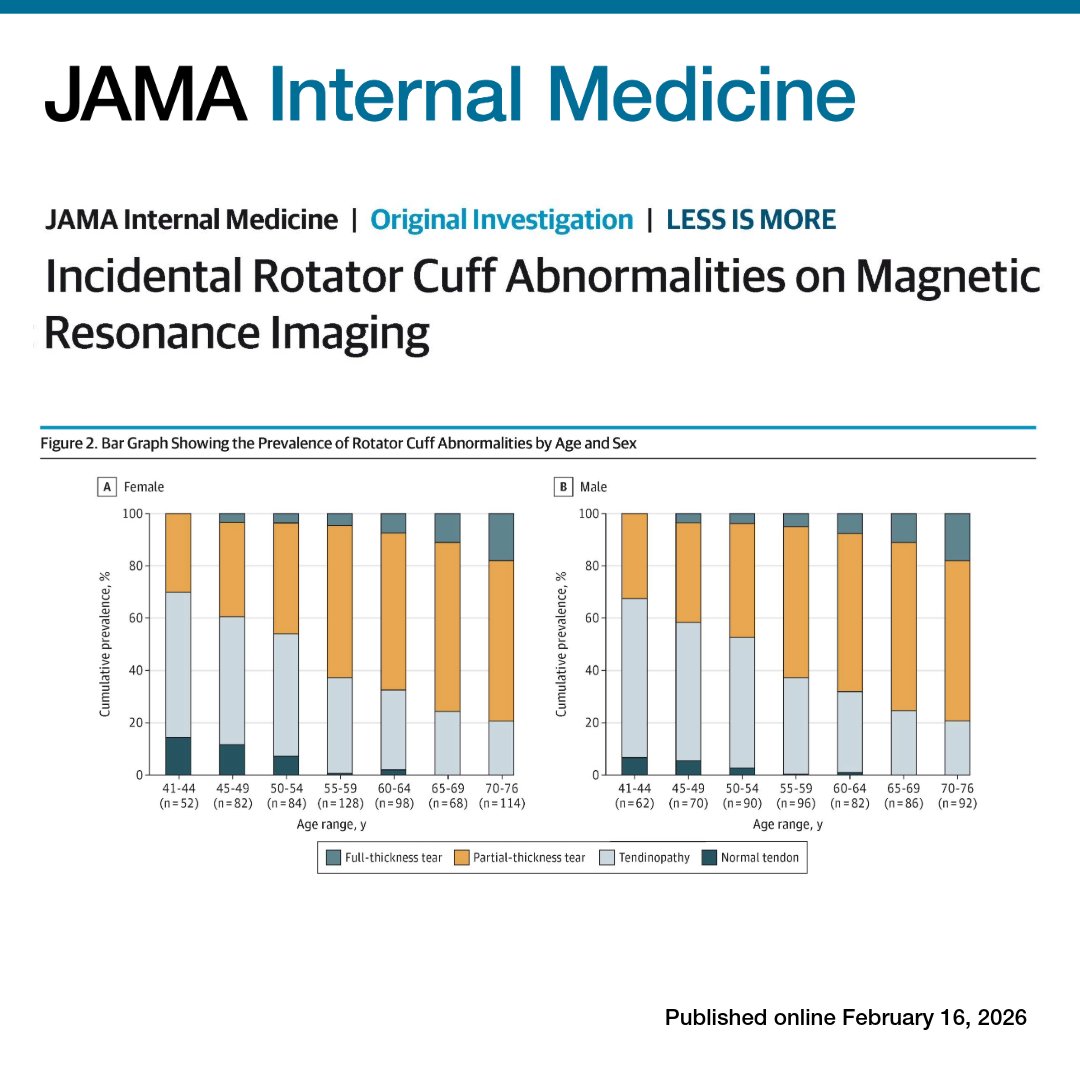
From @JAMAInternalMed: #RotatorCuff abnormalities on #MRI were found in 99% of adults aged 41 to 76, including 96% of asymptomatic shoulders, indicating most findings are age-related rather than disease.
https://t.co/f33KbhzT4z
WHO
People over 18 in UK who received treatment for Achilles pain in the last 12 months
Or
Healthcare professionals providing treatment with Achilles tendinopthy
https://t.co/Sz0aTfiuqr
#achillestendinopathy#tendonpain#healthcareprofessionals
Just published 🔥
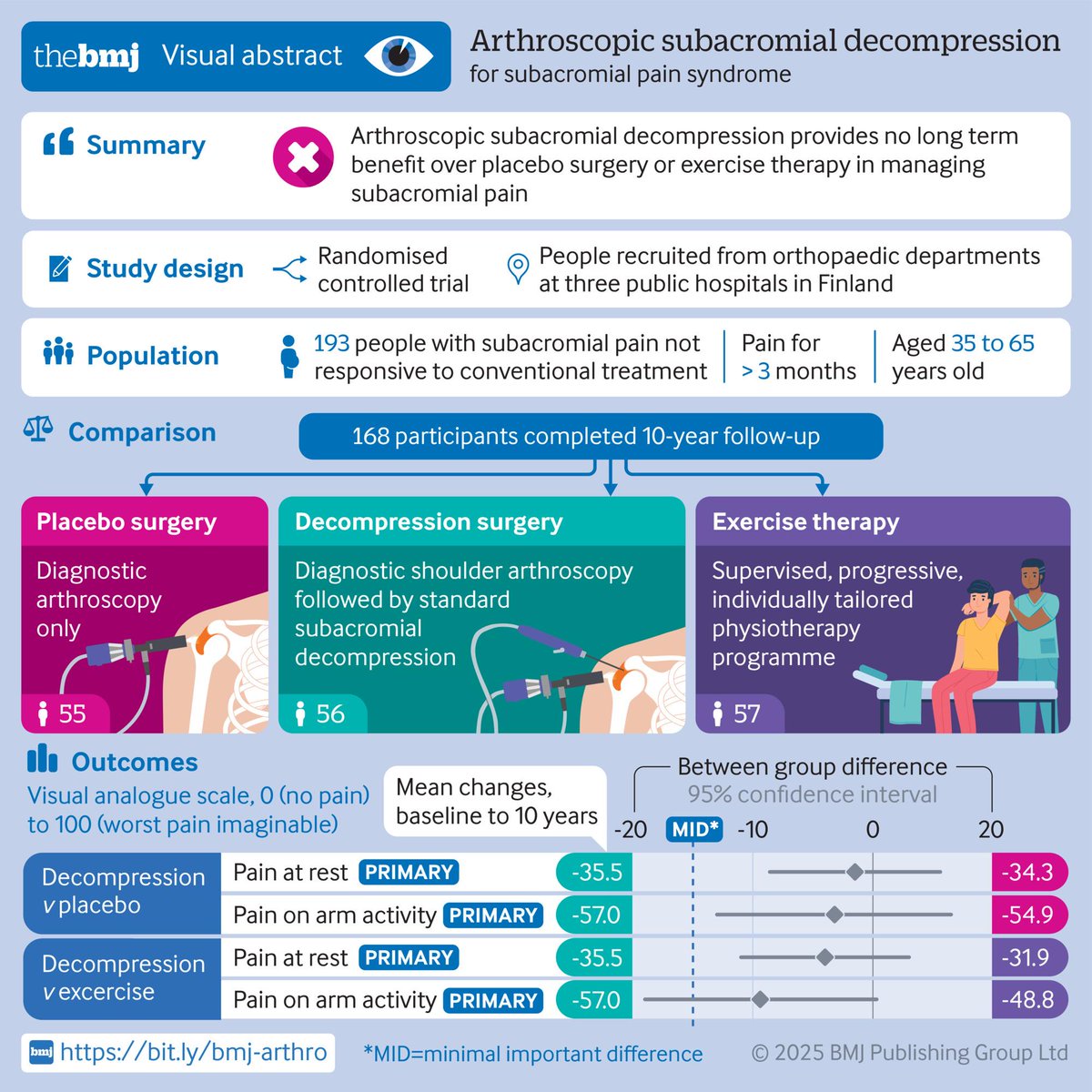
Arthroscopic subacromial decompression versus placebo surgery for subacromial pain syndrome: 10 year follow-up of the FIMPACT randomised, placebo surgery controlled trial
https://t.co/D3C9Z9niBW
You walk into two different clinics.
Clinic A is bright and organized. You’re greeted like a human. Someone actually asks what matters to you, listens without rushing, explains what they find, and gives you a say in the plan.
Clinic B is cluttered. Barely any eye contact. A quick checklist “assessment,” then a generic printout with no explanation.
Same person, same body. Different experience. Which one leads to better outcomes?
We obsess over the specifics: isometrics vs. isotonic, isolation vs. compound, peak vs. rate. These can matter, but there’s another layer shaping results: non-specific effects. Expectations. Trust. Collaboration. The way the room looks. The story around the intervention. These factors can’t replace good programming, but they can amplify it or undermine it.
High expectations tend to boost short-term outcomes. A strong therapeutic alliance improves pain and function, even when the “machine” is off. And the ritual of care, the environment, sequence, and meaning, change how a person’s brain and body respond.
None of this is fluff. It’s part of doing the basics well. The best plans combine sound methods and the human side of care.
Curious: which “non-specific” factor have you felt most in your own training or rehab: expectations, alliance, or ritual?
There is still time to apply for this fabulous clinical/research split role with our fab @C0raHealth team in the North West
Please get in touch if you have any questions!
Advanced MSK Clinician” career opportunity by @C0raHealth with an embedded (shoulder/Upper Limb) PhD scholarship in partnership with @LiverpoolHopeUK 👇🏼
Closing date: 09 September
@AndrewVCuff
https://t.co/GukRUCxELe.
What a day at @ShoulderDocUK#shoulderstudyday
Picked up some gems from @ChrisLittlew00d on research brilliantly demonstrated with the live research study 🧐
Advanced MSK Clinician” career opportunity by @C0raHealth with an embedded (shoulder/Upper Limb) PhD scholarship in partnership with @LiverpoolHopeUK 👇🏼
Closing date: 09 September
@AndrewVCuff
https://t.co/GukRUCxELe.
https://t.co/Rrzx0VKsH9 dear Twitterati please give generously to my dear friend who is facing her biggest challenge yet. Despite horrific injuries her spirit and humour are undimmed. Let’s get her home 💕
1/
#Patellofemoralpain rehab = chasing quads.
And long-term PFJ patients?
They're ninjas at avoiding quad load—even during 'quad' exercises.
Never underestimate the body's ability to adapt away from load.
🧵👇 Here's how I manage it clinically: