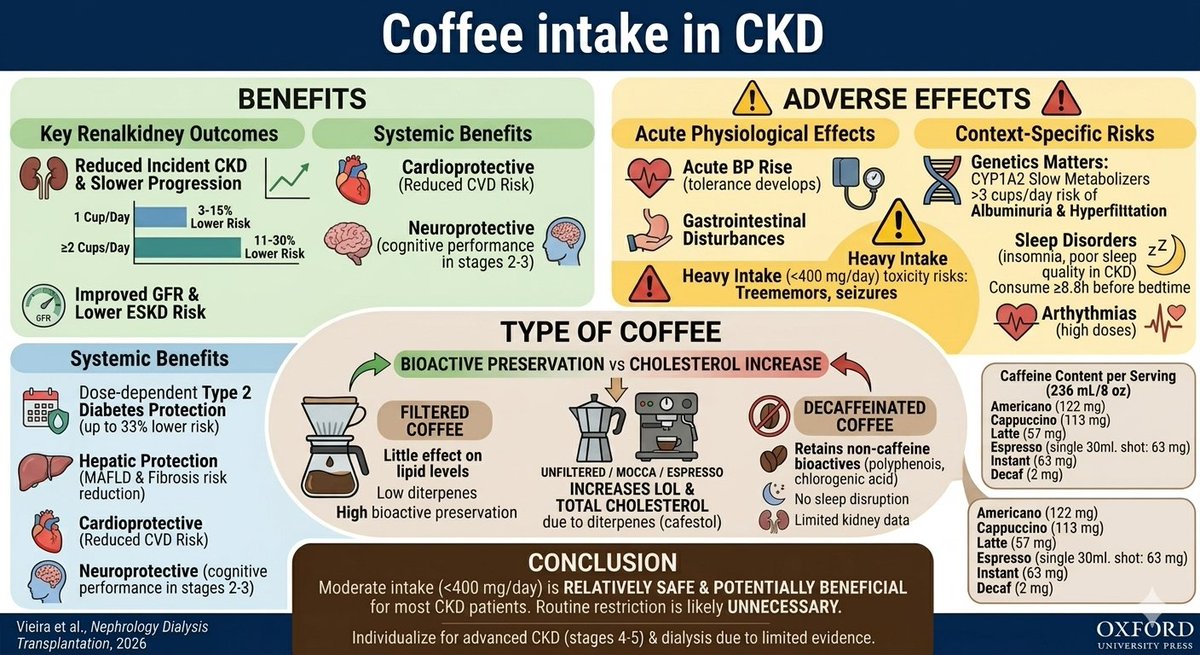
Now open access in @NDTsocial
Coffee consumption and chronic kidney disease
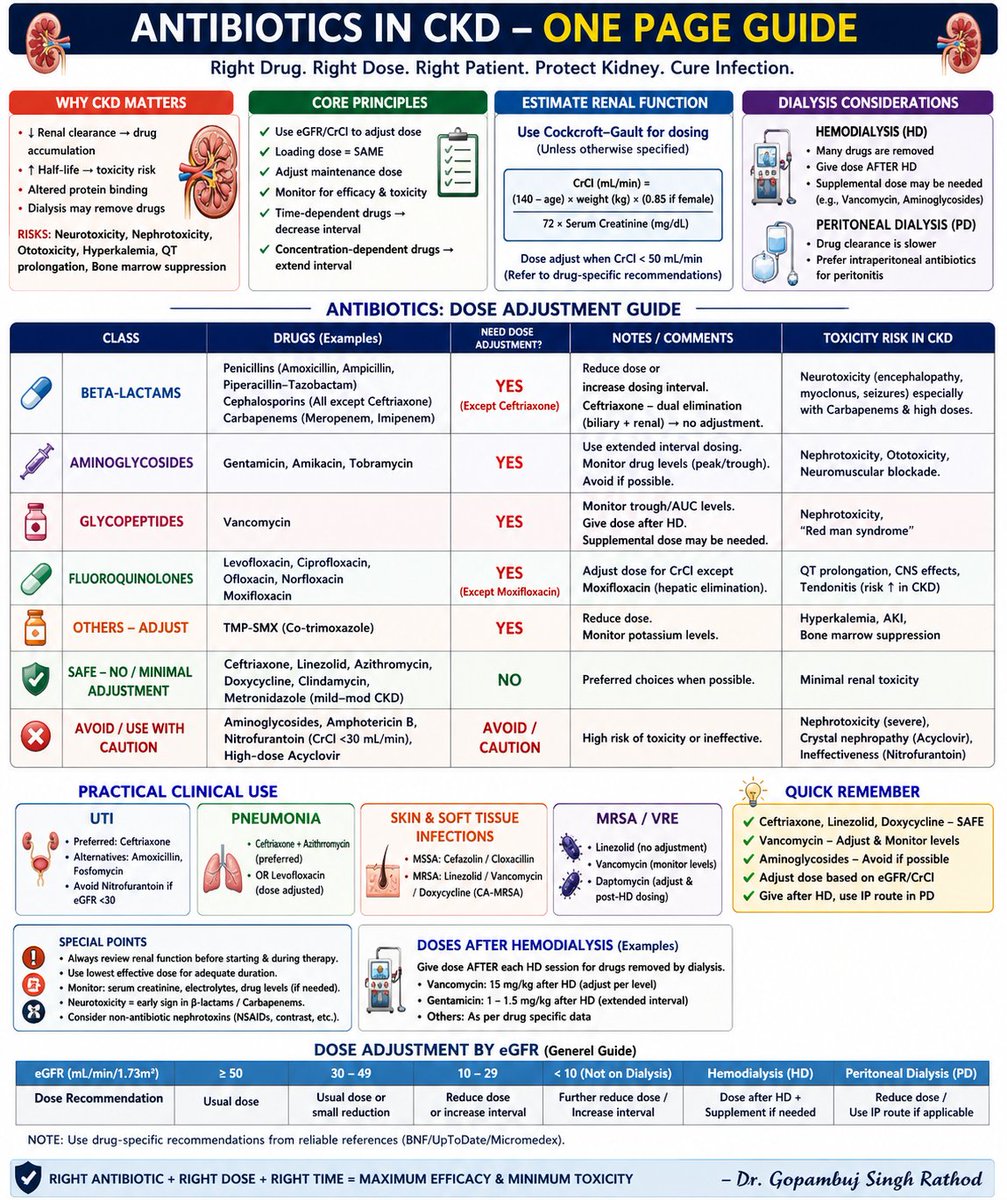
🧐Current evidence suggests that moderate caffeine intake is probably safe in CKD and may be potentially beneficial.
▶️https://t.co/UksqIYFlWK
People often ask that if they are doing good after starting dialysis , why they should go for transplant ?
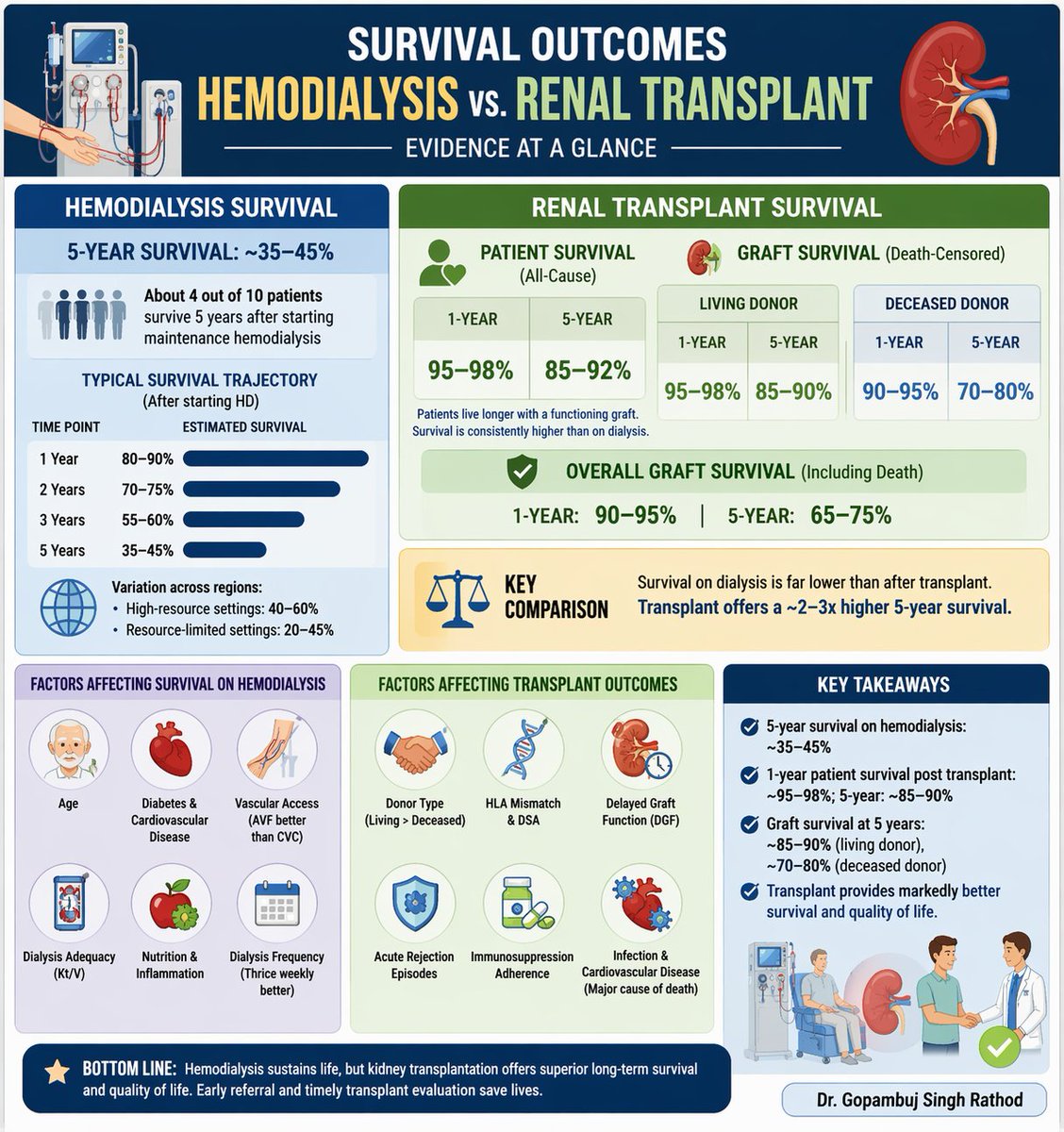
💉 Here's a Survival Reality Check between HD and Transplant-
📊 5-year survival on hemodialysis: ~35–45%
👉 Only ~4 out of 10 patients make it to 5 years
🧬 Kidney Transplant changes the story:
✅ 1-year patient survival: 95–98%
✅ 5-year patient survival: 85–90%
✅ Graft survival at 5 years:
• Living donor: ~85–90%
• Deceased donor: ~70–80%
⚖️ The difference is clear:
Transplant offers ~2–3× better long-term survival than dialysis
❤️ Beyond survival:
✔ Better quality of life
✔ Freedom from dialysis
✔ Improved cardiovascular outcomes
📌 Bottom line:
Dialysis sustains life…
👉 Transplant restores it
#GSR #BuddingNephros
#Nephrology #KidneyTransplant #Dialysis #CKD #MedEd #NephTwitter
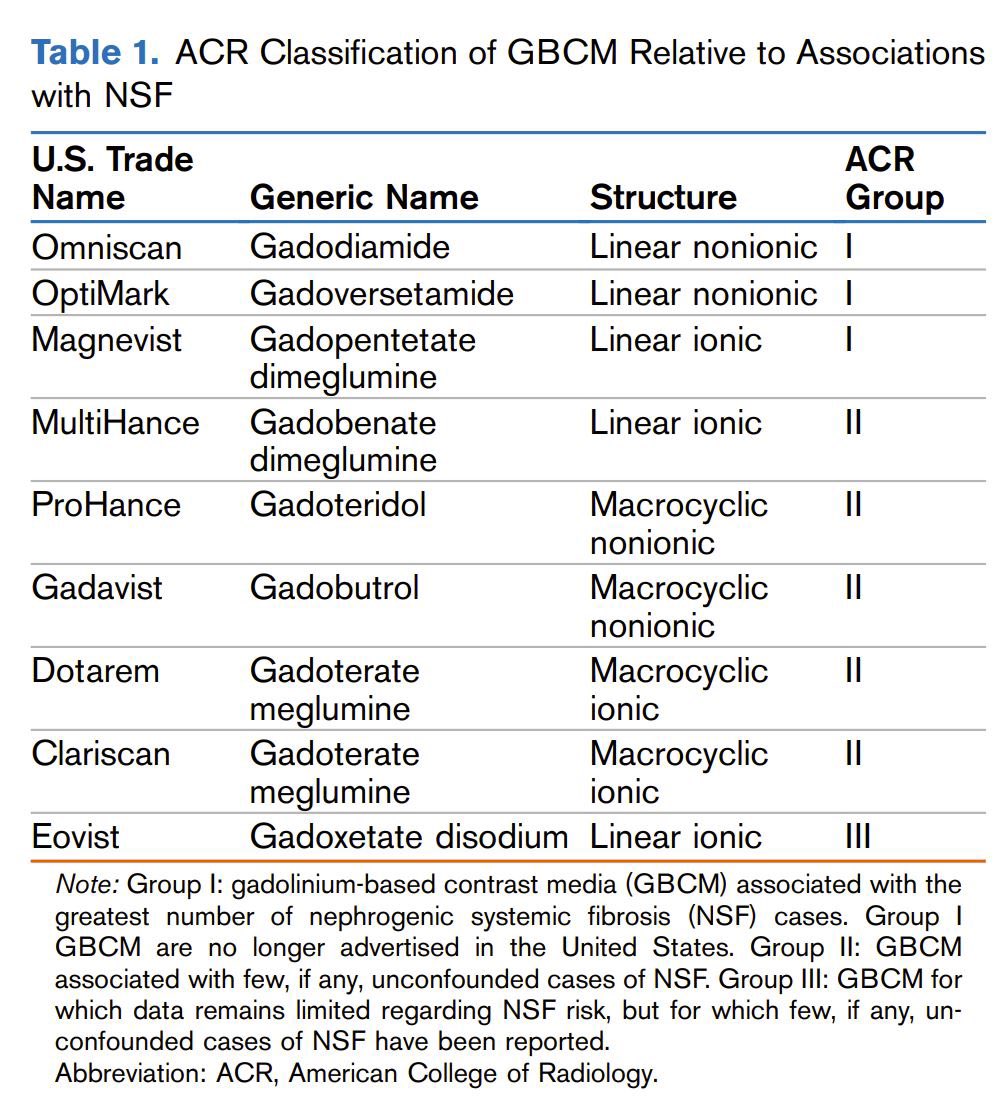
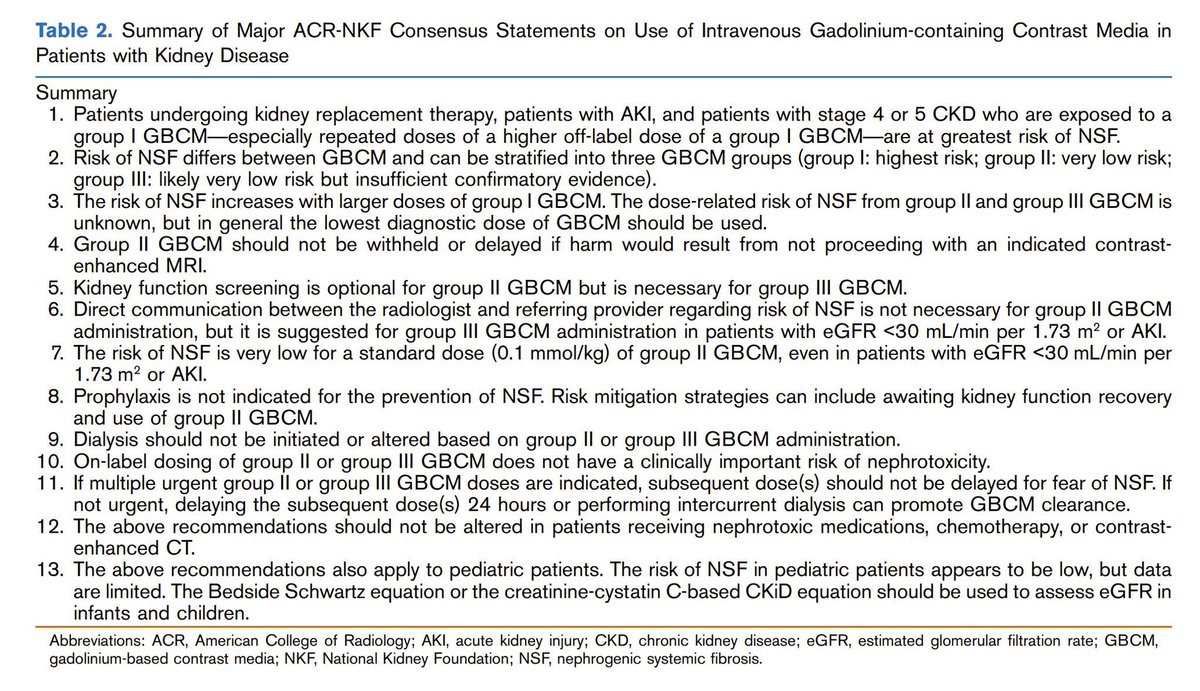
Update on gadolinium and CKD/ ESKD ca. 2021 from @NephRodby@MPerazella#Nephpearls
Risk of nephrogenic systemic fibrosis is low w/ group II gadolinium-based contrast media GBCM, so potential harms of delaying/ withholding group II GBCM for MRI in a patient w/ AKI or eGFR < 30 is likely to outweigh risk in most situations
👉 https://t.co/lFUicEy5sg
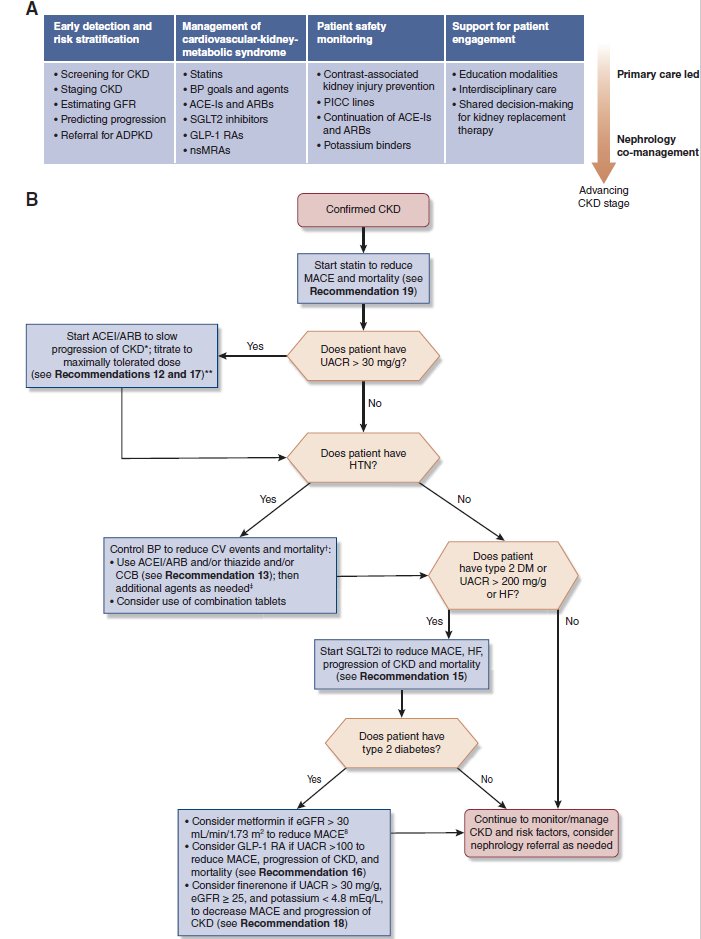
The dramatic expansion in CKD therapeutics to prevent progression of kidney disease and reduce cardiovascular events calls for thoughtful implementation. The 2025 guidelines synthesize new evidence for Primary Care Management of CKD in this #ASNCJASN#perspective https://t.co/6yj0GWECfy
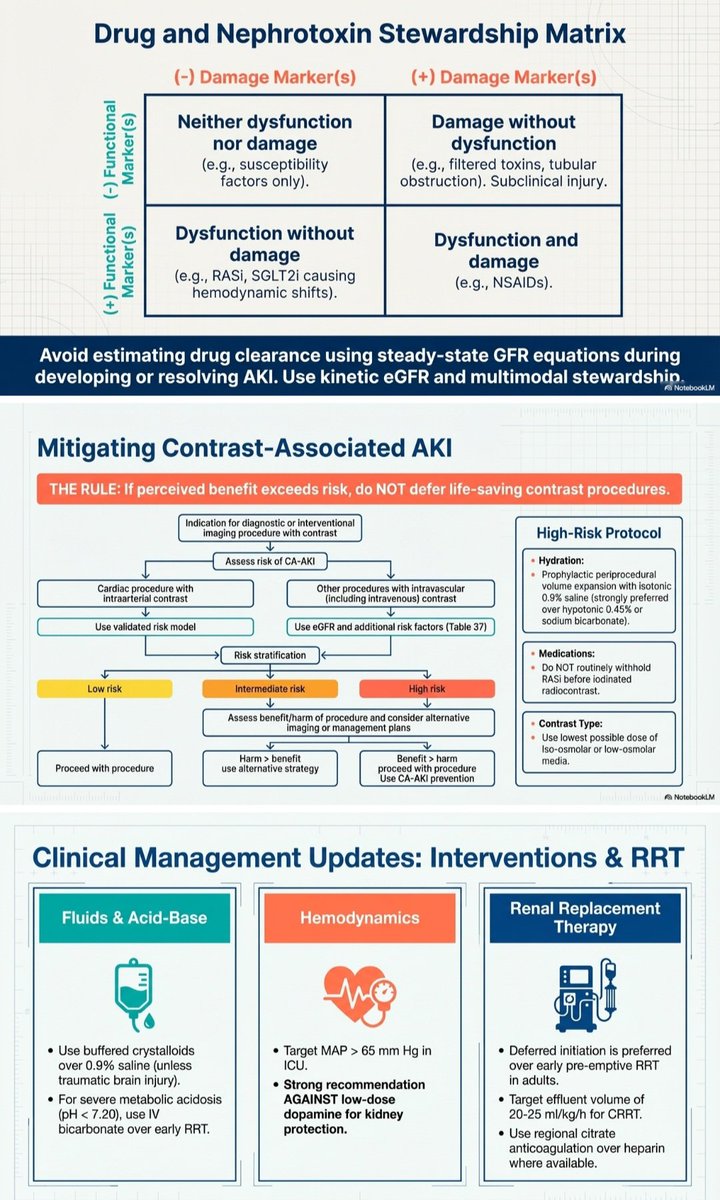
🩻Contrast-induced AKI:
one of the biggest myths still shaping clinical decisions
For decades we were taught:
👉 “Contrast damages the kidneys”
👉 “Avoid CT with contrast in CKD”
👉 “Hydrate, protect, delay imaging if needed”
But what if… most of this is wrong?🤔
->The uncomfortable reality
Modern evidence shows:
👉 Low-osmolar contrast rarely causes true nephrotoxicity
👉 Even in CKD, AKI, and ICU patients
👉 The risk is often overestimated—or nonexistent
So where did the fear come from?
📍 1950s high-osmolar contrast (actually toxic)
📍 Poorly controlled observational studies
📍 “Creatinine rise = contrast injury” assumption
👉 Correlation became causation
👉 And the dogma stayed
⚠️What recent data tells us
✔ No difference in AKI rates with vs without contrast
✔ No benefit from bicarbonate, NAC, or aggressive hydration
✔ Even ICU and AKI patients show no worsening outcomes
->Translation to real life
👉 The patient was going to develop AKI anyway...Not because of contrast!!
->The real problem: “Renalism”
👉 Avoiding necessary imaging
👉 Delaying diagnosis
👉 Choosing inferior tests
And that leads to:
❌ Missed PE
❌ Delayed sepsis source control
❌ Worse outcomes
->Clinical mindset shift
Instead of asking:
👉 “Will contrast harm the kidneys?”
We should ask:
👉 “Will NOT doing the scan harm the patient?”
->Who still deserves caution?
✔ eGFR <30
✔ Severe hemodynamic instability
✔ Multiple nephrotoxins
Even then:
👉 Optimize volume
👉 Minimize dose
👉 Don’t delay critical imaging
🤓Bottom line
✔ Contrast nephrotoxicity exists… but is rare
✔ The fear is bigger than the risk
✔ The harm of NOT imaging is often greater
In critical care
👉 We don’t treat creatinine
👉 We treat patients
And sometimes…
👉 The most dangerous thing is NOT the contrast
👉 It’s hesitation.
📃Reference
Florens N, Demiselle J.
Kidney360 7: 445–449, 2026. doi: https://t.co/CWzi7WC9Wx
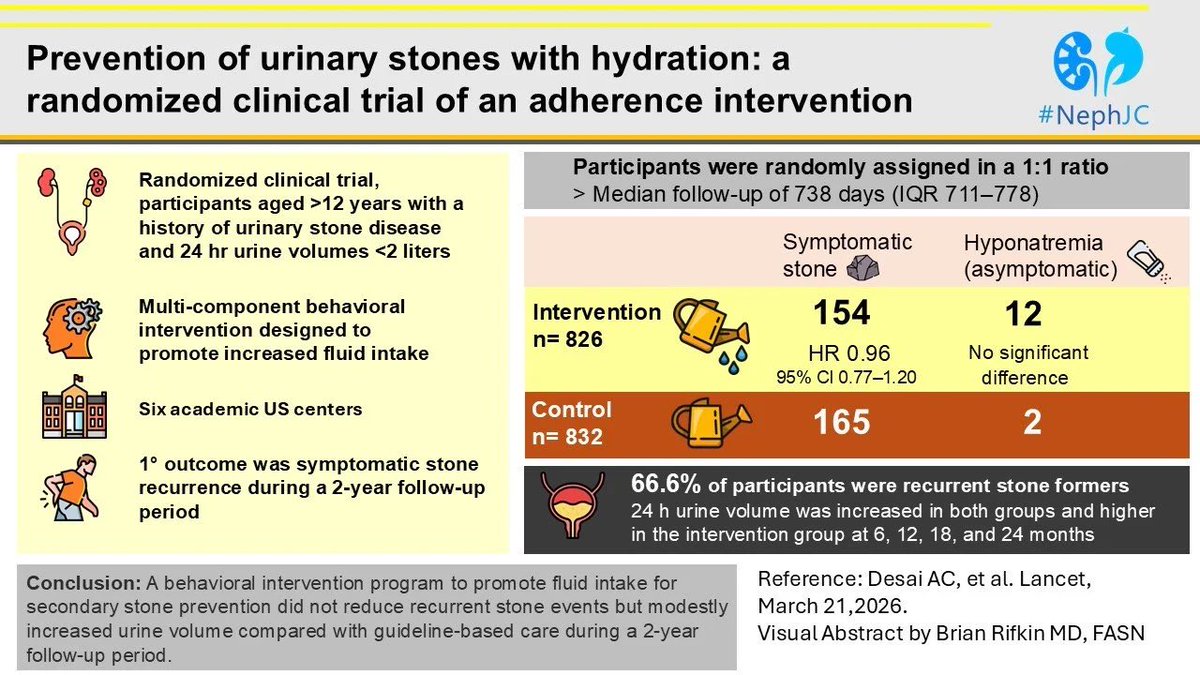
Prevention of Urinary Stones with Hydration - PUSH Trial
1. Didn't work
2. Tough to get pts to drink more water.
The PUSH Trial in Lancet - https://t.co/z3FeZofyKs
A nice synopsis of the trial here - https://t.co/UsgpNWNeCh