If insurance companies can deny care and call it "medically unnecessary", why aren't they required to have malpractice insurance doe when they get it wrong and someone gets sicker or tragically dies ?
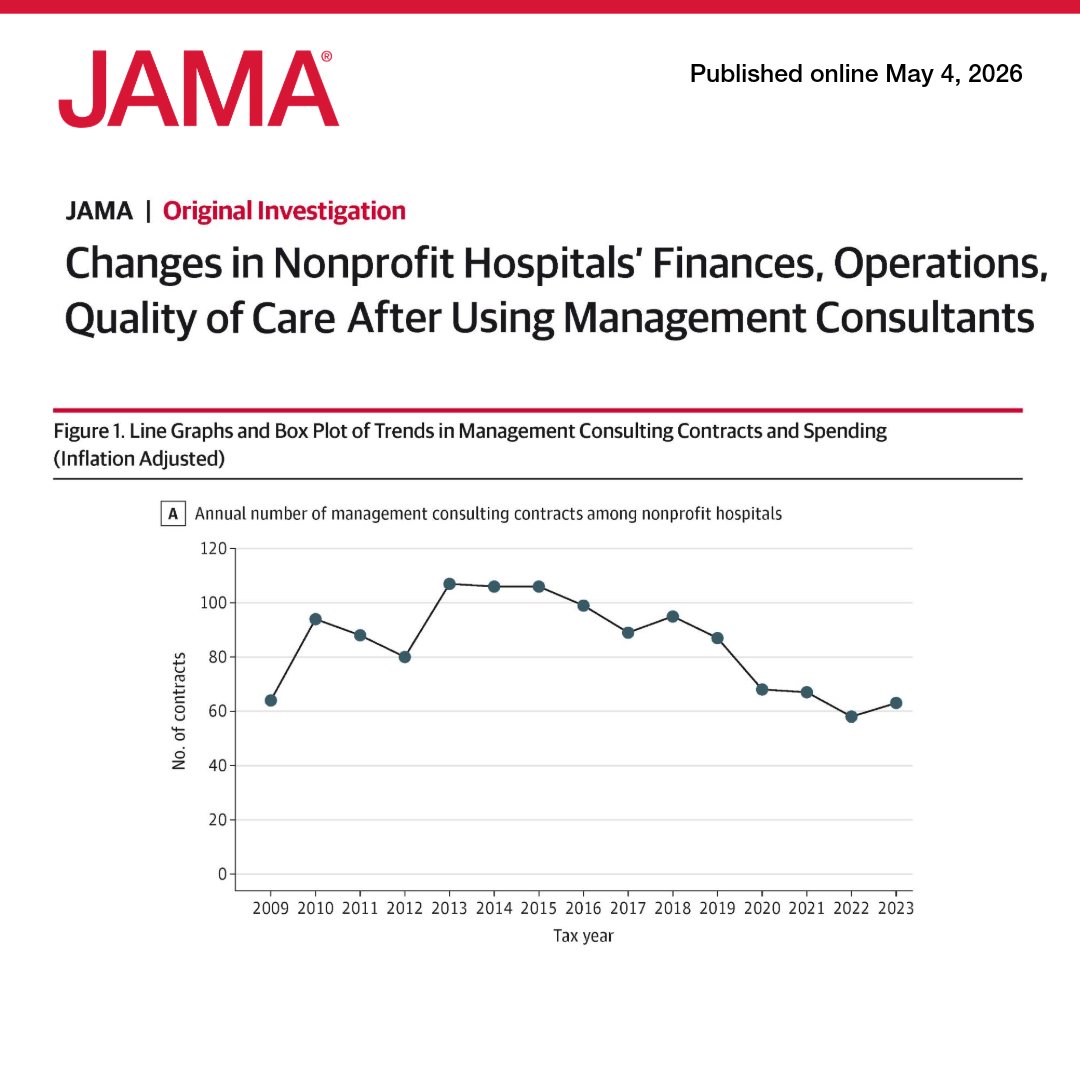
US nonprofit hospitals spent $7.8 billion on management consultants from 2009 to 2023, but contracts were not associated with meaningful changes in finance, operations, or quality of care. 🧵
https://t.co/QQswMYxrG8
Here is the key issue - paperwork.
There are hundreds, if not thousands of different insurance plans with different payment and claim mechanisms. Providers need to account for all of them so that when you show up with your insurance card, they know what to do
We need to standardize contracts b one for commercial. One for Medicare. One for MA. One for Medicaid. Plug in the numbers and other info.
That cuts admin costs and keeps practices and hospitals open
Want to know the craziest part about insurance company Pre Authorization Denials ?
The insurance company defines the network of providers the patient can use
When they deny care, they are effectively saying "we don't trust the judgement of the doctors we require you to use" 🤯🤯🤯
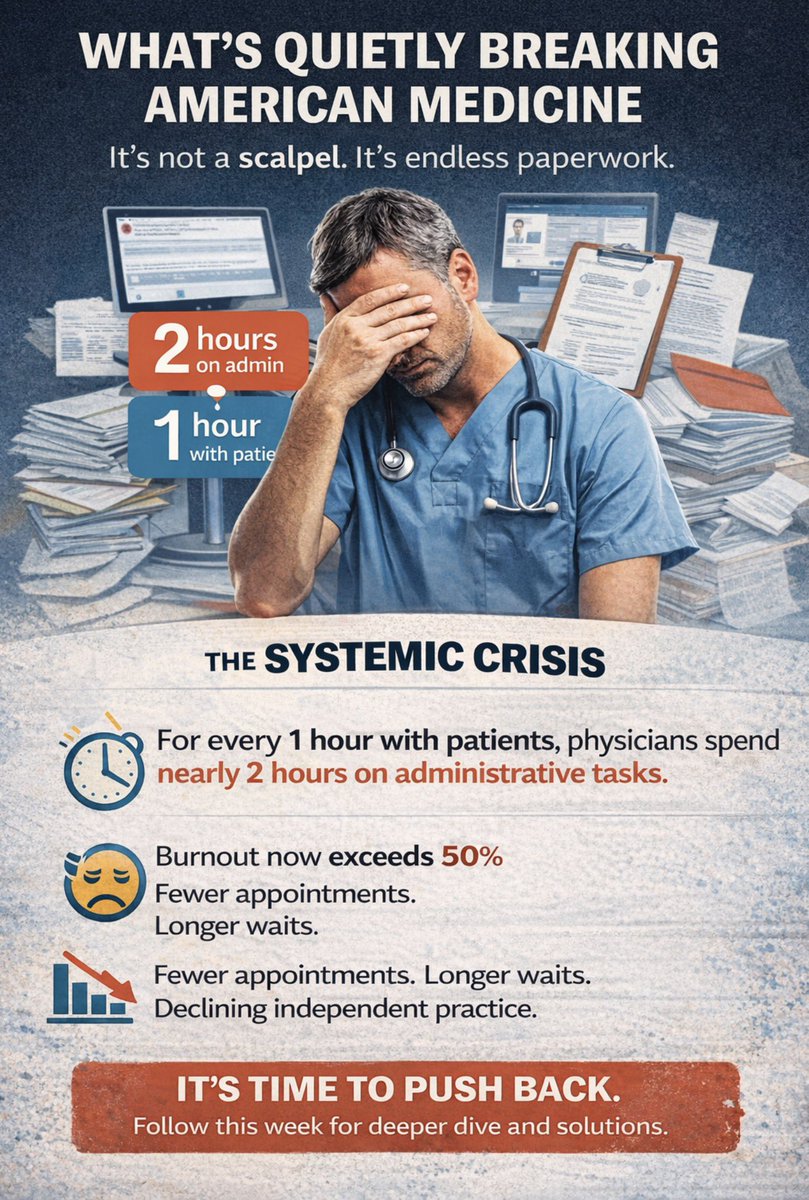
This week we need to talk about something that’s quietly breaking American medicine and it has nothing to do with a scalpel.
I became an orthopedic surgeon to take care of patients; to fix broken bones, restore function, and give people their lives back. What I did not sign up for was spending a significant portion of my working hours on documentation, prior authorizations, insurance portals, and administrative tasks that have nothing to do with the patient in front of me.
I’m not alone.
The average physician now spends nearly 2 hours on administrative work for every 1 hour of direct patient care. Burnout rates among physicians have crossed 50%. Early retirement is accelerating. Medical school graduates are rethinking specialties based not on what they love, but on what comes with the least paperwork. Physicians are choosing employment over independent practice to avoid the headaches.
This is a systemic crisis with real consequences for patients who can’t get appointments, face longer wait times, or lose access to their physician entirely.
The system has spent years adding to physicians’ plates while calling it “efficiency.” It’s time to push back with data, with policy, and with our voices.
Follow along this week as I break down the issue and then provide solutions on Friday.
Reply with your biggest frustrations with administrative burdens in medicine
Galen and Scott do an incredible job articulating what this Indiana Football team has meant to so many of us.
Take a few minutes to listen to this clip from the most recent @CrimsonCast episode.
#iufb
Forgot the most important item. If brand pricing went to net via wholesalers, @costplusdrugs could buy brands from them , make them up only 15 pct and cut the price of EVERY SINGLE BRAND MEDICATION
The greatest deceit in these hearings is not what is said at the table, but what is quietly assumed behind it.
They are staged as inquiries,
stern questions, performative outrage, a theatrical search for accountability. Yet the premise is false.
The lawmakers are not merely observers of the system’s failures.
They are participants in its design.
These hearings exist to create the illusion of scrutiny while preserving the architecture of extraction: the subsidies, the carve-outs, the regulatory protections, the carefully engineered opacity that insulates incumbents from competition and patients from truth.
In Washington, “oversight” has become a kind of ritual, a liturgy if you will, of concern recited by those who have already blessed the outcome.
The public is meant to believe the crisis is accidental. It is not.
The lawmakers are in on it.
The Centers for Medicare & Medicaid Services isn’t a neutral referee.
It’s the rule-maker that built the current system.
It created site-neutral payment loopholes.
It wrote billing codes that favor hospitals.
It designed reimbursement rules that pushed doctors to sell their practices.
It structured 340B to reward consolidation.
These weren’t mistakes.
They were choices, often well-intentioned, responding to political pressure.
But here’s what matters: CMS has enormous power to shape healthcare markets.
When it pays more for health system based care, hospitals expand.
When it restricts physician-owned hospitals, consolidation increases.
When it creates arbitrage opportunities, someone will arbitrage.
The question isn’t whether CMS officials are good people.
It’s whether any centralized authority can design payment rules that produce the outcomes we want.
Maybe instead of trying to engineer the perfect payment system, we should ask: what if patients controlled more of their healthcare dollars?
What if physicians competed for their business?
What if we discovered that voluntary exchange, the same force that’s reduced costs everywhere else, could work in healthcare too?
The average family now spends as much on health insurance as they do on their mortgage or rent.
That wasn’t true in 2010.
Does the fact that health systems, using cash from medicare, to buy 60% of independent practices have anything to do with the rise in premiums?
The US government would never do that....
I like most all physicians in private practice in Connecticut lost my practice as insurance companies stopped paying us reasonable rates for seeing patients and performing surgery. The government supported the vertically integrated insurance companies, doctors went into debt, sold to private equity, joined large groups, or joined hospital systems. Patient service suffered, patients lost their long time doctors, quality sank, patients lost faith in the system, and doctors burned out. The cost of medicine soared as the ACA gave insurers excessive power and the for profit insurers had to answer to Wall Street. More profit equalled less patients treatment for a higher cost.
Saint Francis ➡️ James Madison ➡️ Indiana
No matter where Elijah Sarratt has played, the WR always seems to be open.
The Journey spotlights @IndianaFootball's 𝘞𝘢𝘧𝘧𝘭𝘦 𝘏𝘰𝘶𝘴𝘦 👇
�� @AutoOwnersIns
Let me get this straight….
We’re dumping hundreds of billions in taxpayer dollars into subsidies so people can afford a system deliberately designed to fleece them.
Instead of questioning that, we ask for more money.
That’s like buying a house with termites, finding out it’s on fire,
and responding by refinancing to get a new granite countertop.
The problem isn’t that people don’t care.
It’s that we’ve normalized stupidity.
For fifteen years, we’ve handed nonprofit health systems tax breaks like they’re charities,
while they operate like private equity firms in lab coats.
They merge.
They consolidate.
They crush independents.
They jack up prices.
And somehow, we reward them with even more subsidies.
Meanwhile, the people who actually deliver value,
the independent physicians who innovate,
take risks, and pay taxes
get starved out.
CMS and the insurers treat them like party crashers,
while the nonprofits bill 5x more for the same MRI
and call it a “community benefit.”
You want to fix costs?
Then stop subsidizing the predators
and start supporting the builders.
But no,
we’ll just keep torching taxpayer dollars
so some health system CEO / MBA can collect his seventh bonus for “efficiency gains”
while premiums go up again next year.
Math exists.
People just refuse to use it.
Everyone knows the last Big Ten team to win at Oregon, right?
It's Indiana #iufb
The Gerry DiNardo led '04 Hoosiers beat #24 Oregon 30-24. Here's a Lance Bennett TD return from the game
The costs of health insurance for a family of 4 were $13,000 in 2010 and are now $35,000 in 2025.
The cost-sharing has increased as well.
This is unaffordable and unacceptable, and the ACA has failed to cut costs.
We need to admit that and find a better solution that is physician-led and not government led.
We need to limit the role of health insurance to rare and catastrophic events and let patients pay for the following:
• Imaging
• Labs
• PRescriptions
• physician services
• procedures
• physical therapy
We need absolute price transparency and to overturn every piece of legislation that increases costs and prevents competition. @DutchRojas@DrDiGiorgio@anish_koka@drdanchoi
Enough is enough of the madness caused by hundreds of unsupervised juveniles downtown and the ongoing issue of mass shootings. Parents need to start being responsible, or we must hold them accountable.
History tells us the preferred path for government policymakers trying to deal with too much debt is lowering interest rates and devaluing the currency the debt is denominated in.
Doing this is a very hidden way of reducing wealth, because as your currency goes down, it makes it look like other things are going up. But despite the downsides, this wealth shrinkage and reduction in buying power is favored by policy makers precisely because its impacts are less obvious than the alternatives.
At such times, you should expect interest rates and the currency’s value to fall.