🏃♂️🫀 Exercise Prescriptions Should Be Risk-Stratified — Not Generic
Current guidelines recommend ≥150 min/week of moderate-to-vigorous physical activity (MVPA) for everyone.
But is that optimal for a 45-year-old low-risk individual and a 70-year-old very high-risk patient?
This large UK Biobank cohort (72,884 participants, median 13.2-year follow-up) provides a more nuanced answer .
🔬 What’s innovative?
• Objective 7-day wrist accelerometer data
• ESC-aligned SCORE2 risk stratification
• Isotemporal substitution modeling (reallocating sedentary time)
• Identification of optimal vigorous activity thresholds by risk group
📊 Key findings
Each +150 min/week MVPA →
• 20% lower CVD risk in very high-risk individuals
• 16% reduction in high- and low-to-moderate-risk groups
Higher-risk individuals benefit the most from increasing activity.
BUT intensity matters.
When replacing 300 min/week sedentary time:
🔹 Low-to-moderate risk → Any mix of moderate (MPA) and vigorous (VPA) works. More VPA = more benefit.
🔹 High risk → VPA should be ≤60 min/week (~20% of MVPA).
🔹 Very high risk → Optimal VPA ≈ 42 min/week (~14% of MVPA). Beyond that, benefits decline.
In high-risk groups, excessive VPA may attenuate benefit—likely due to hemodynamic stress, endothelial dysfunction, and oxidative burden.
🎯 Take-Home Messages
1️⃣ Physical activity remains powerfully protective across all risk strata.
2️⃣ Higher-risk patients gain the largest relative benefit.
3️⃣ Vigorous exercise has a ceiling effect in high-risk individuals.
4️⃣ Exercise prescriptions should integrate formal risk stratification (e.g., SCORE2).
Precision prevention now extends to lifestyle medicine.
One size does not fit all.
🫀⚖️ High-risk coronary plaques: intervene early—or hold the line?
This 2026 EuroIntervention Viewpoint by Mintz & Collet delivers a sober, evidence-driven answer to one of interventional cardiology’s most debated questions: should we prophylactically stent “high-risk” plaques, or manage them medically and wait?
🔍 What defines a high-risk plaque?
Across invasive and non-invasive imaging, features such as large plaque burden, small MLA, thin-cap fibroatheroma, large lipid core, low-attenuation plaque, positive remodelling, napkin-ring sign, and spotty calcification consistently associate with future events. Lesions with multiple features are riskier—but here’s the catch 👇
📉 Absolute risk is low
Despite ominous imaging, annual hard event rates (death/MI) are ~1%, and most plaque ruptures are clinically silent, contributing to progression rather than ACS. This reframes the entire preventive-PCI debate.
🧪 What do randomized trials show?
PROSPECT ABSORB and PREVENT tested preventive PCI vs optimal medical therapy (OMT).
PCI improved lumen dimensions and reduced future revascularizations, but did not reduce death or MI at 2, 4, or 7 years.
In PREVENT, 739 PCIs prevented only 20–36 later PCIs—a poor trade-off.
Meta-analysis confirms: benefits are driven by fewer procedures, not fewer hard events.
⏳ What happens if we wait?
Long-term follow-up (PROSPECT II, PREVENT) shows very low event rates with OMT and delayed PCI when symptoms arise, avoiding most upfront interventions without penalty.
🧠 Where the field is heading
The authors advocate a “hold-the-line” strategy:
Detecting high-risk plaque should trigger intensified medical therapy and surveillance, not automatic PCI.
Future precision may come from integrating imaging + physiology + inflammation, to identify the rare plaques whose rupture truly matters.
🔮 Bottom line
Until we can predict **which plaques will cause death or MI—not just progression—**the data favor medical therapy first, PCI later if needed.
Seeing risk ≠ fixing it with a stent 🚀
Advanced imaging in the southern world. CMR with 4D flow enables better understanding of blood flow alterations in a single acquisition. A novel technique particularly useful in aortic pathology and congenital patients. #whycmr@marzagod@AlemanaTemuco@medufro
https://t.co/wCB0WwlM5U
https://t.co/RUyPTlIT8N
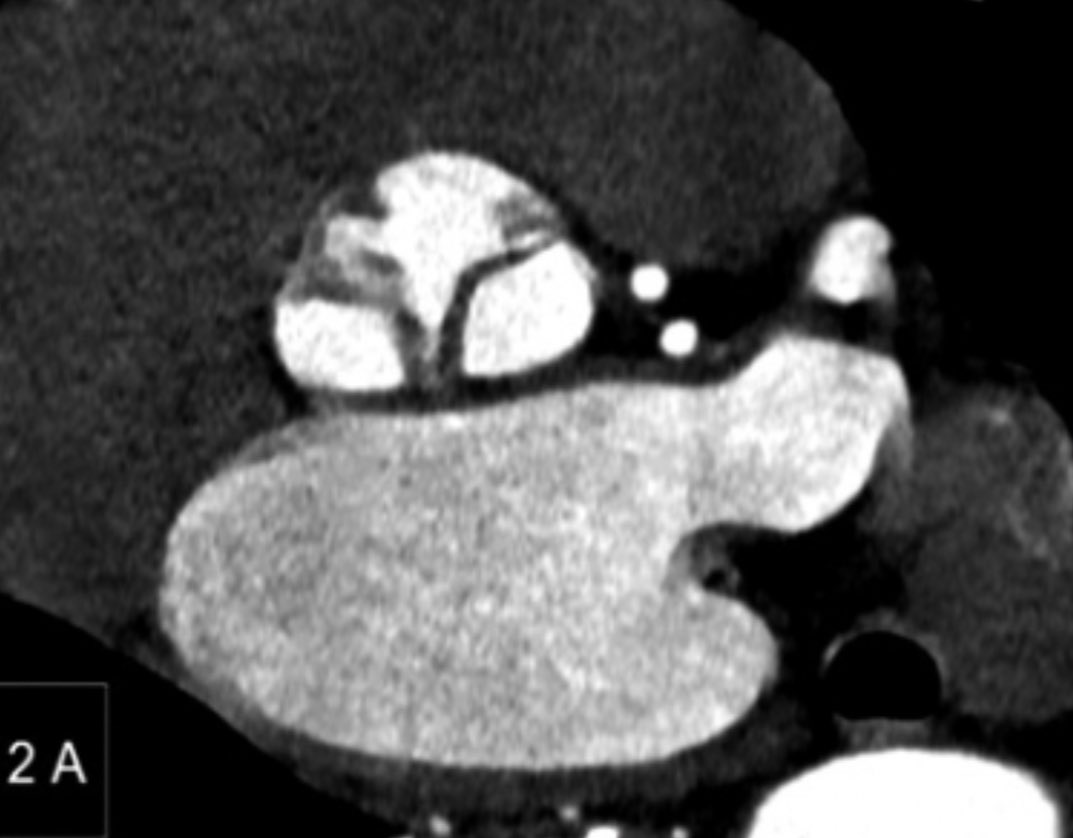
A very nice case. Anomalous origin of the right coronary artery from the left sinus of Valsalva. Gated CT angiography allows us to evaluate the anatomy very precisely (and beautifully): position, relationships, and morphology of the ostium, length of the intramural course, its degree of stenosis, and other associated anomalies. @marzagod@AlemanaTemuco@medufro@HHHATEMUCO
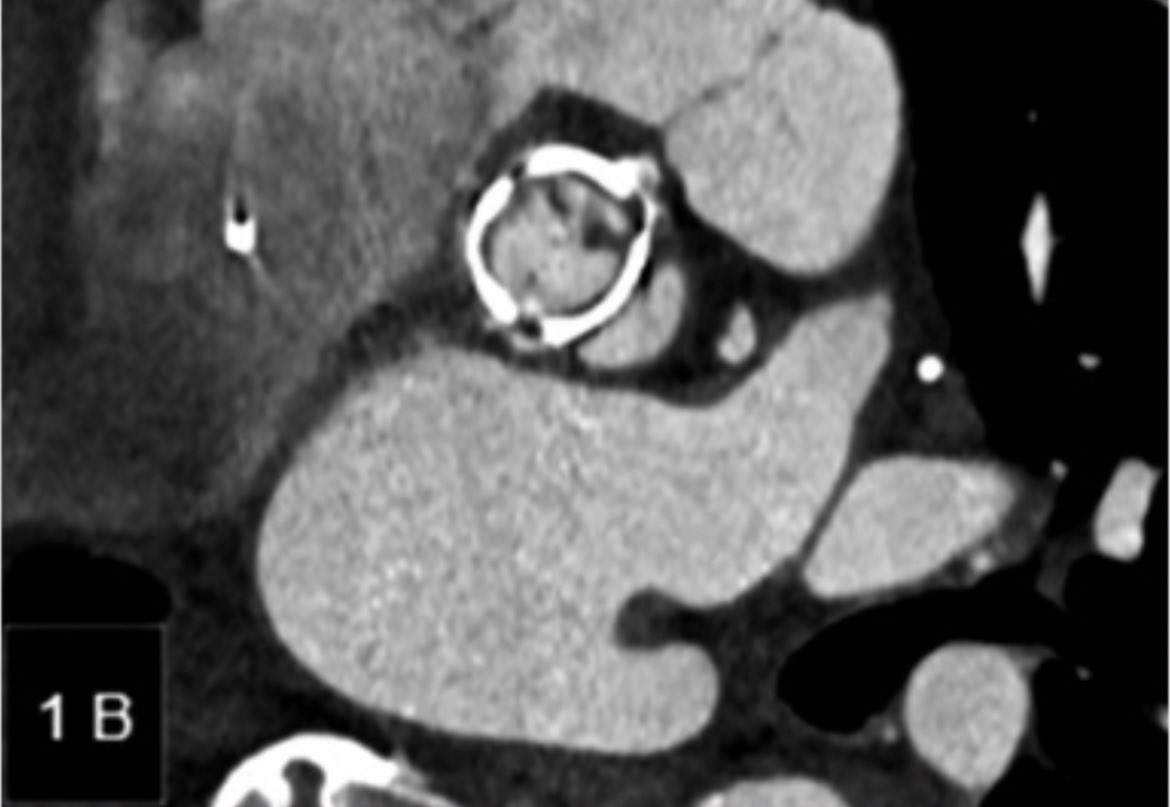
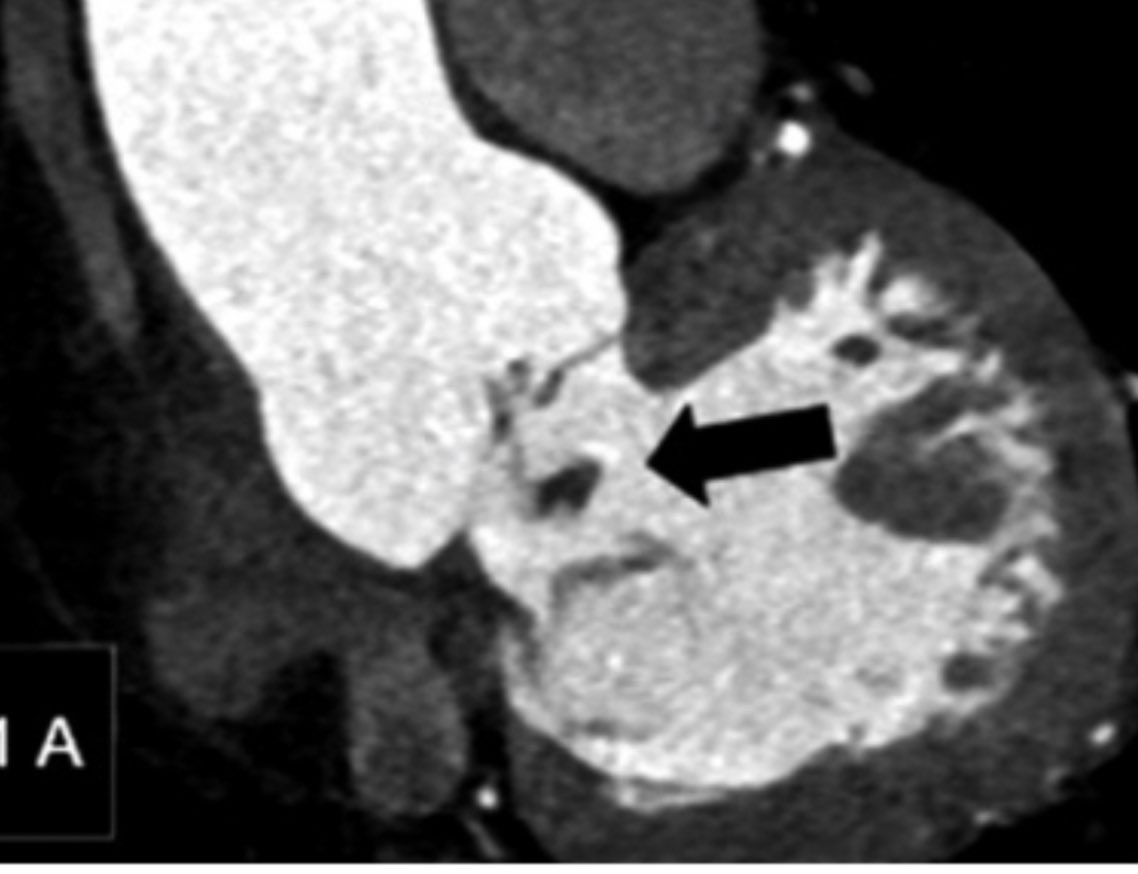
📖👓 Utilidad Angio-TC cardíaco en la evaluación de la endocarditis infecciosa. Una revision de hallazgos en casos locales, lee el artículo completo acá ➡️ https://t.co/qYFzR2Jz3r @marzagod@medufro@AlemanaTemuco@HHHATEMUCO
For any cardiology fellows interested in training in multimodality CV imaging --> we have an unexpected opening for our 2 year fellowship starting July 1, 2026
Please RT/share #YesCCT#ThinkPET#WhyCMR#EchoFirst#CVImaging#ACCImaging#PCCT
#SCCT2025 was a so relevant meeting. Opportunities, inspiration and challenges for all of us. It's always nice to meet up with old friends and masters. Thanks for choosing Montreal, beautiful city. See you in San Diego 2026, maybe HK. @Heart_SCCT
Thank you to all the amazing volunteers, faculty and attendees who made #SCCT2025 a huge success! Can't wait to see you all again next year in San Diego!
President Maros Ferencik spoke with @AuntMinnie about #SCCT2025 and shared some highlights & trends that attendees can expect to absorb in Montréal this week.
Watch the video: https://t.co/57lFtCPZgM