Check out this recent review on oral selective estrogen receptor degraders (#SERDs) for the treatment of hormone receptor-positive, HER2-negative #BreastCancer.
👉https://t.co/3FAC4LCxYr
@ValenzaCarmine@curijoey@darioT_
Happy to share our recently published work! https://t.co/EONa944pcI #mdpiijms - @IJMS_MDPI@Rodrosb@anamg_98
📰Implementation of HER2DX Scores into Treatment Decisions in Early-Stage HER2-Positive Breast Cancer.
🤔HER2DX influenced treatment decisions in over half of patients in routine clinical practice.
👇👇Take a look
During #UterineCancerAwarenessMonth, raising awareness starts with the evidence that guides patient care 🩺 Two evidence-based reviews on #EndometrialCancer offer updated guidance across the continuum of care. Explore the recommendations @gynoncjnls: https://t.co/sj3iG4rqon
Drs. Waks (@adawaksmd) and Sammons (@drsarahsam) introduce a patient case of a 62‑year‑old woman with HER2+/HR- #breastCancer. They discuss how to select an optimal first‑line regimen for her amid an expanding range of therapeutic options. They review and compare data from the DESTINY‑Breast09 and phase 3 HER2CLIMB-05 trials, outlining evidence‑based treatment strategies for this clinical scenario. Watch here ⬇️⬇️
https://t.co/sM1AUHuLag
Results of the T-DXd/durva arm of #BEGONIA for 1L mTNBC are now out in @NatureCancer. High efficacy, with ORR 62% and mPFS 12.6 months. Strikingly, deep responses observed even in HER2-0 (null) dz, reminding that IHC is a poorly predictive ADC biomarker. https://t.co/IlLsYPJxzz
Team Ovary is excited to share our multidisciplinary review on HIPEC in ovarian cancer, now published in Surgical Oncology Insight. 🎉
Read the article here:
https://t.co/jbSIvepQ3N
Evolving Treatment Paradigms in Hormone Receptor–Positive, Human Epidermal Growth Factor 2–Negative Metastatic Breast Cancer
@ASCO Educational Book👇
https://t.co/KKAM0ugITs
Only few days to #ASCO26. For breast oncologists, this edition will deliver a new promising biomarker to spare unnecessary chemo, informative updates from practice-changing trials across subtypes, and major innovations coming from China. See you in Chicago next week! #bcsm
The approval of T-DXd for the (neo)adjuvant treatment of HER2+ breast cancer will add an invaluable tool to our arsenal. Yet, in this era of right-sizing, not all patients require T-DXd treatment to be cured. Some thoughts in my recent JCO editorial. https://t.co/tKCgzzbdiq
Interesting new data from #SERENA6 showing that the cumulative incidence of ESR1 muts rises steadily over time. ctDNA monitoring detected ESR1m in ~20% within 1 year, but the incidence was highest between years 1-4. #ESMOBreast26
Vepdegestrant in ER+, HER2–, ESR1-Mutated Breast Cancer
US FDA approval
VERITAC-2 Trial : An overview
Era of niche precision endocrine therapy has just begun
It’s that time of the year again! #ESMOBreast26 is only a few days away, and promises to bring new important data in breast oncology. This year’s key themes: tailoring therapy for HER2+ eBC, prospective data with ADC sequencing, use of MRD to guide treatment. See you in Berlin!
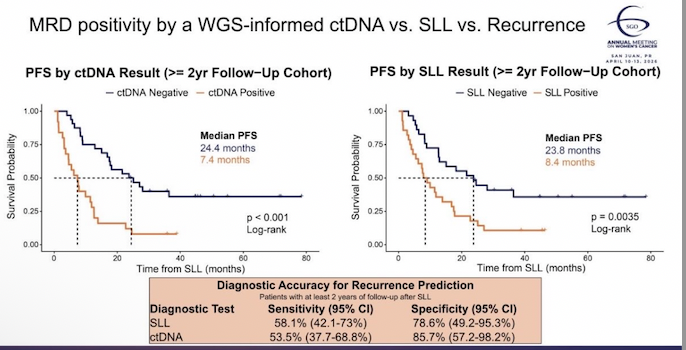
#ctDNA vs second-look laparoscopy for #MRD detection in #ovariancancer. Clark et al. Abstract #207 #SGO2026.
ctDNA positive: median PFS 7.4 months. ctDNA negative: 24.4 months. SLL positive: median PFS 8.4 months. SLL negative: 23.8 months.
Both are prognostic. The survival separation is nearly identical. But the diagnostic properties are not.
SLL sensitivity 58.1%, specificity 78.6%. ctDNA sensitivity 53.5%, specificity 85.7%.
SLL finds more disease. ctDNA is more specific - fewer false positives.
This matters because these tools are not competing for the same job anymore.
Second-look laparoscopy was abandoned because detecting residual disease did not change outcomes. There was nothing to do with the information. That calculus has changed. We now have maintenance strategies, PARP inhibitors, bevacizumab, immunotherapy, that may perform differently depending on MRD status. The question is no longer just whether disease is present. It is whether the answer should change what you do next.
ctDNA cannot replace SLL on sensitivity. But it is non-invasive, repeatable, and longitudinal-exactly what we need to embed in clinical trial designs and escalation/de-escalation strategies.
Pre-test probability in gynecologic cancers is distinct. Do not import ctDNA interpretation frameworks from breast or colorectal cancer and apply them here.
The field needs prospective trials that treat ctDNA status as a decision node, not just a prognostic marker. That is the next step.
#SGO2026 #OvarianCancer #GynOnc #Oncology #MedTwitter @SGO_org@GOG@NRGonc@GYNCancer@gyncsm
#AACR26 | #NeoZanHER - the finding nobody is talking about
#Zanidatamab monotherapy in early HER2 IHC 3+, ERBB2-amplified breast cancer. No chemotherapy.
▪️ 30% pCR
▪️ Much less toxicity
▪️ 56% HER2 downregulation in residual tumor after treatment
That last number is the story. Zanidatamab strips HER2 expression from surviving cells through receptor clustering and internalization. Residual tumor after this drug may look HER2-low or zero.
Standard adjuvant T-DM1 in non-pCR patients assumes HER2 is still there. After zanidatamab - it may not be. Sequencing question nobody has answered yet.
@ZymeworksInc@JazzPharma #BreastCancer #HER2 #AACR26
🤰Pregnancy after breast cancer? Reassuring new data
POSITIVE trial: Temporary interruption of endocrine therapy for pregnancy appears feasible, safe in selected patients with HR+ #breastcancer.
👩⚕️ @AnnPartridgeMD of @DanaFarber at #MBCC26 | #OncoFertility
https://t.co/SLDt0DRWG0
Elevate your approach to high-risk HR+, HER2- early #BreastCancer care with CDK4/6 inhibitors. Don't miss experts Joyce O'Shaughnessy, MD (@BCJoyceO), and Eleonora Teplinsky, MD, FASCO (@drteplinsky) in this new PeerView #MedEd activity! https://t.co/JcGrm0afWa
#Oncology