Safety and efficacy of low-intensity versus standard monitoring following intravenous thrombolytic treatment in patients with acute ischaemic stroke (OPTIMISTmain) - The Lancet https://t.co/p3oxZkSIhD
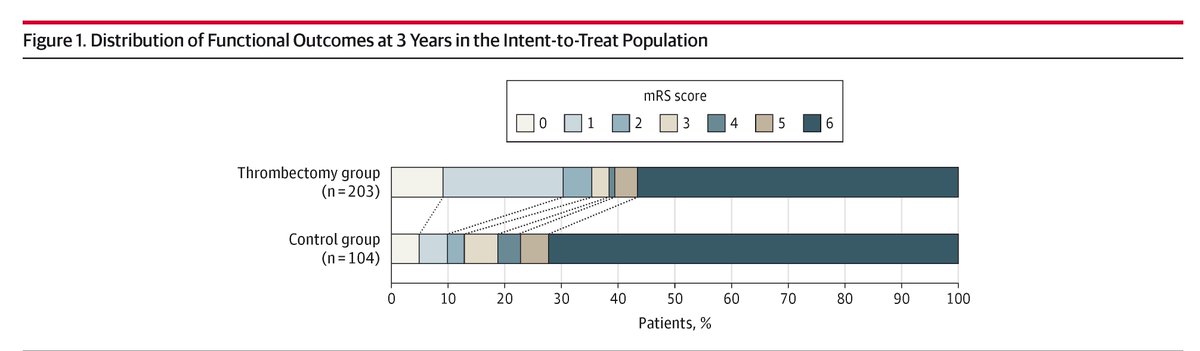
Among patients <70 years with acute #BasilarArteryOcclusion, endovascular thrombectomy doubled the rate of ambulatory and self-care capable outcomes at 3 years vs medical treatment.
https://t.co/Tlv2ftRPuu
#STROKE: In an economic analysis based on the ENRICH trial, minimally invasive trans-sulcal parafascicular surgery was more cost effective than medical management alone. #AHAJournals https://t.co/7iMIk9FuOK
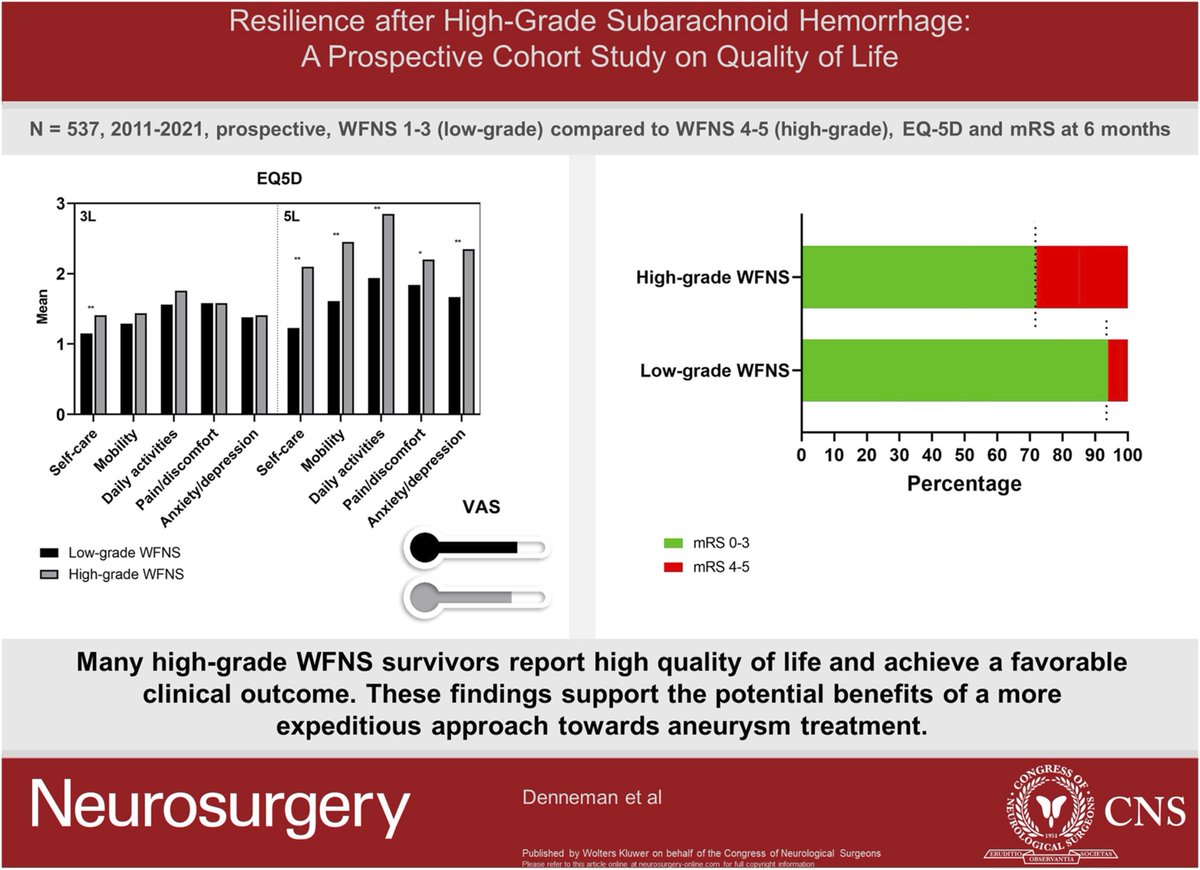
Increasingly clear that pts with high grade #SAH can do well and that we should not limit or delay treatment. @NeurosurgeryCNS@neurocritical https://t.co/VExmyzjkAd
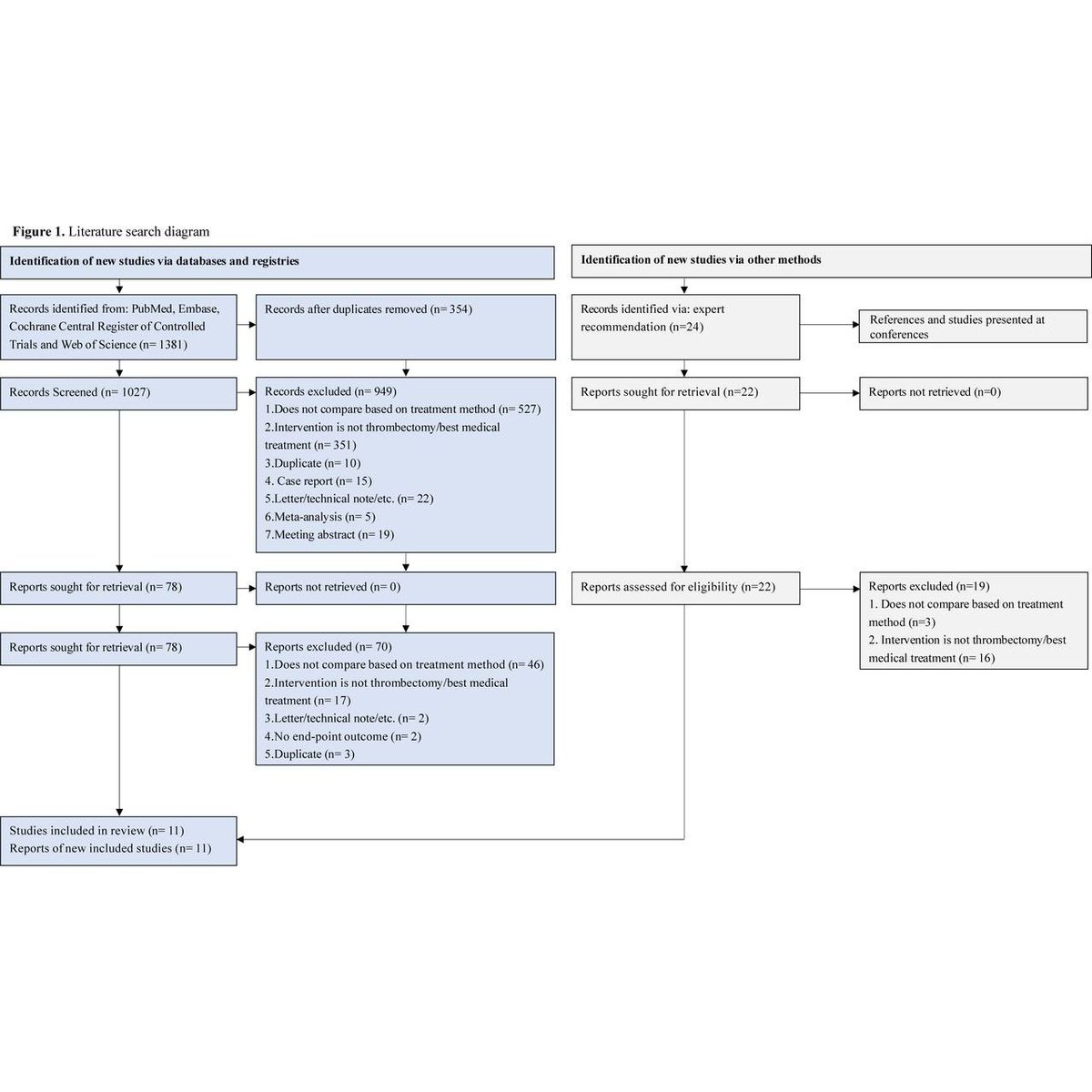
In this meta-analysis, Guo et al. find that Endovascular treatment (EVT) may improve outcomes in acute ischemic stroke due to isolated posterior cerebral artery occlusion (iPCAO), offering higher chances of excellent recovery & early neurological improvement vs best medical treatment (BMT). #EVT #thrombectomy #stroke
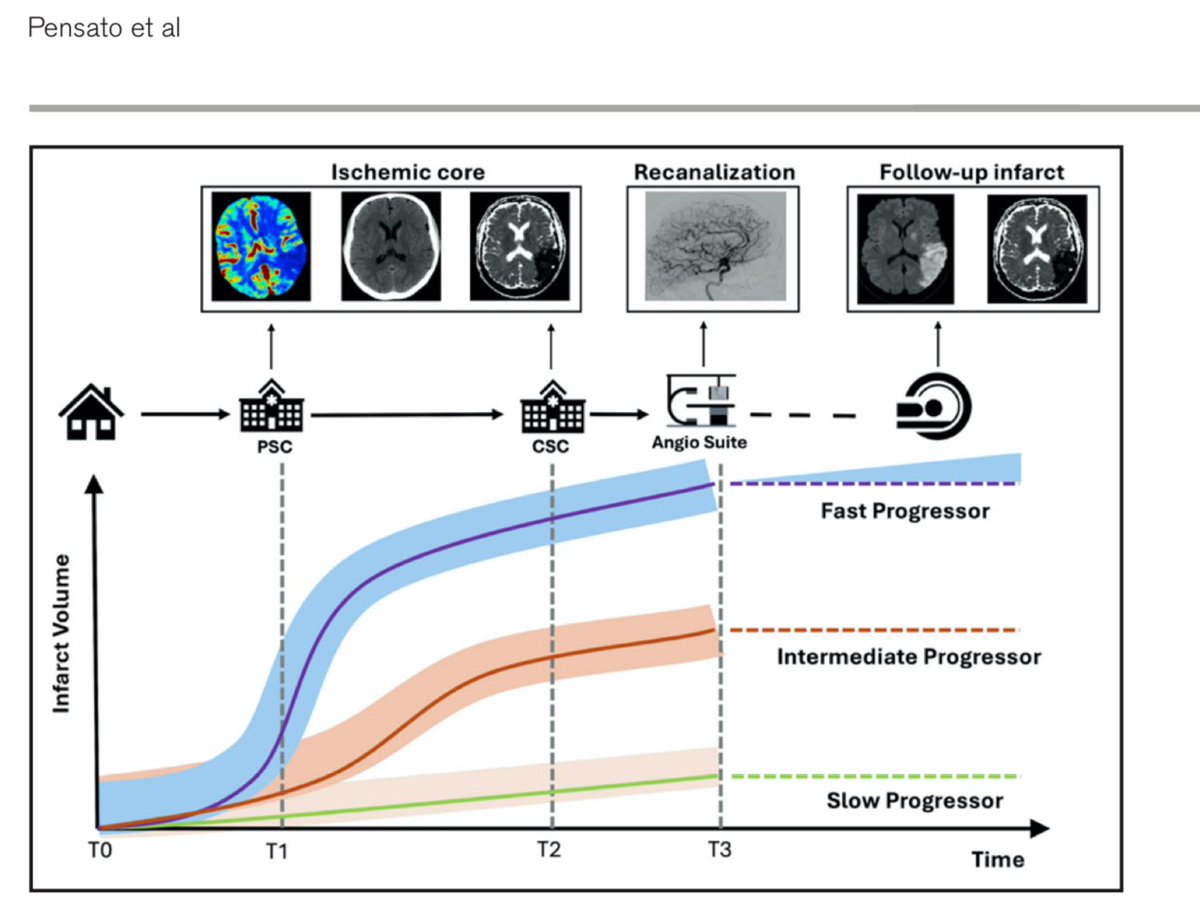
Summarizing Pensato et al Fast, Intermediate, vs Slow Progressors in Stroke:
1.Pathophysiology of Stroke 🧠
Infarct growth occurs due to critical blood flow reduction, leading to energy failure. Tissue in the ischemic penumbra can be salvaged with quick intervention but progresses variably based on factors like collateral flow.
2.Measurement Techniques 📊
Infarct Growth Rate (IGR) is assessed using imaging techniques such as CT and MRI. Methods include single- and double-snapshot approaches or perfusion estimates, with average IGR being 5.4 mL/h but highly variable.
3.Stroke Progressor Phenotypes 🚦
Patients are classified into fast progressors (IGR ≥10 mL/h) and slow progressors (<5 mL/h), aiding in predicting outcomes and planning treatments.
4.Research Gaps 🔍
A lack of standardization and understanding of complex infarct progression dynamics (e.g., nonlinear growth) highlights the need for better, continuous metrics and classifications.
5.Clinical Implications 🩺
Recognizing IGR can assist in predicting patient outcomes, optimizing transfer for thrombectomy, and selecting neuroprotective strategies, reinforcing the “time is brain” principle.
“You’re only as good as your collaterals”
#BayMazwi
#TimeIsBrain #1.9MillionNeuronsLostPerMinLVO
Pensato U, Demchuk AM, Menon BK, et al. Cerebral infarct growth: pathophysiology, pragmatic assessment, and clinical implications. Stroke. 2024;56:00-00. doi:10.1161/STROKEAHA.124.049013.
Internal jugular vein catheters probably don't have any effect on ICP according to this study from @EmoryNeuroCrit : https://t.co/PPwIwDcrzq. Hard cosign on this one! @MDNeurocritcare@NeurocritCareJ
🧵This Controversies in #Stroke analysis by Bower et al. critically appraises the literature on imaging in intracerebral hemorrhage (ICH). #AHAJournals@LaurenHSansing
The advent of mobile stroke units, application of artificial intelligence for hemorrhage detection, and new data on timing and rationale for different imaging modalities are also reviewed.
https://t.co/9ROykQ4Xv8
We still are overly pessimistic when assessing prognosis after #ICH
In the INTERACT-3 trial Of over 6000 ICH patients physicians (75% neurosurgeons) were very accurate in Identifying who was going to die…
…But massively underestimated the proportion of pts who went on to have a good recovery at six months.
Surprised?
#curingcoma
https://t.co/RoPIt7T4BR
My latest with @JoshGoldsteinMD and friends:
Emergency Priorities in the Treatment of Cerebral Hemorrhage: #CodeICH keeps rolling
https://t.co/UtFfMHKmhw
Tenecteplase versus alteplase for acute stroke within 4·5 h of onset (ATTEST-2): a randomised, parallel group, open-label trial - The Lancet Neurology https://t.co/exRKlqnp2N
Among patients with basilar artery occlusion within 12 hours of onset, the benefits of endovascular thrombectomy at one year compared with 90 days were sustained for favorable outcome and enhanced for excellent outcome. https://t.co/Lu4ZKzIOCX
The #CodeICH train is rolling!
I am ecstatic to share this great editorial by @Dr_Cit and @HemphillCl19865
Making the case that INTENSIVISTS are best positioned to organize ICH treatment bundles at the local level
Couldn’t agree more! https://t.co/Mo0ItzgzjR