Radiologist. Past President Radiological Society of New Jersey. FACR. I love reading about anything and everything, along with sharing. Opinions are my own
So the purpose is to dismantle the AMA?
And we have no voice on Capitol Hill other than fragmented specialty societies?
Do we really think changes in billing are going to benefit physicians?
Do any Google search and you will find that the American Dental Association is the second most powerful lobbying group in DC, behind the NRA.
Similarly, in state capitols.
No surprise they are the least regulated, with insurance not universally accepted, and those that accept it often for basic services only.
Be careful what you wish for.
As Past President of the Radiology Society of NJ, and still Executive Committee member, I have come to recognize how powerful lobbying affects outcomes.
That’s why it’s not uncommon to join with the Medical Society of NJ on important issues like Full Practice Authority for NP’s or restricting an influx of FMG’s.
Similarly, I have visited Capitol Hill every year for > 15 years.
The most recent concern is an MEI update, which the AMA supports.
Less is not more here, if you want anything to get done.
Just ask your local Dentist.
https://t.co/azXAVdDU92
Ok
But who do we have to represent us on Capitol Hill?
The Dental Lobby is the strongest , behind the NRA.
They are united, which is why they have the fewest restrictions.
We are fragmented, up until more recently, with competing objectives.
I go to Capitol Hill every year asking for MEI updates at the American College of Radiology Annual Meeting.
The support of the AMA helps
Likewise-
https://t.co/azXAVdDU92
I graduated University of Pennsylvania 43 years ago.
My daughter, likewise, 4 years ago.
I went to Temple Med far up North Broad St in Philly 39 years ago.
Was Residency Director at Cooper in Camden, NJ, 26 years ago.
Everywhere I went you needed to use caution then, and now.
Is it worse?
Maybe a little.
But not a lot, tbh
Homeless and so on.
Cities are a danger
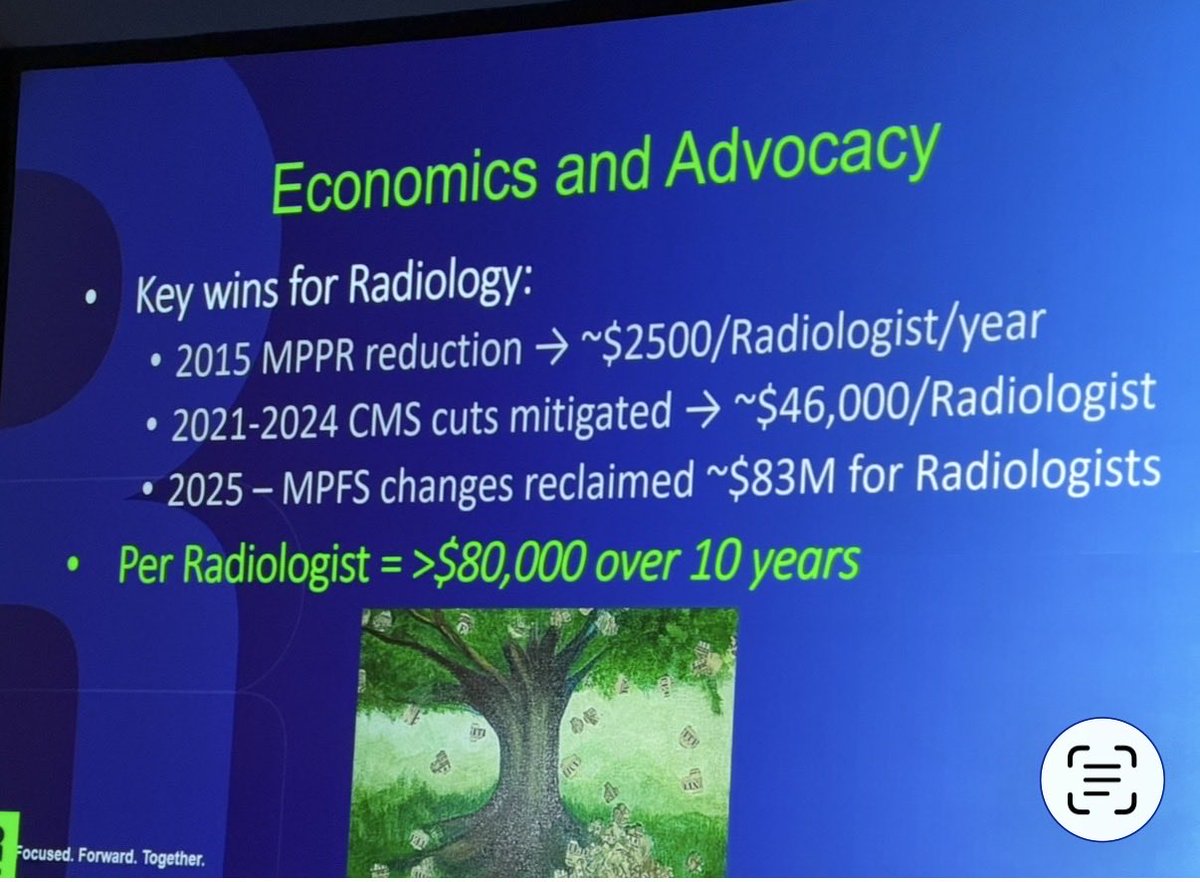
On the other hand, many of my peers on the Radiological Society of NJ look forward to the Annual Meeting and Capitol Hill visit in DC every year.
We’ve won the Governance Award the past 2 out of 3 years for our state.
From a national perspective these are only a few “wins”.
Btw, tbh, I’m not going to respond to simple rhetoric and hearsay anymore.
It’s tiresome
We’ll agree to disagree
Ty
@sethmhardy I have found the Appropriateness Criteria along with the White Papers and Consensus statements of great value for > 30 years of practice in both Academic and Private Practice settings
Regardless of what was spent, CDS/AUC is what is sorely lacking right now.
Anyone who works in an ER setting, or OP setting, recognizes that midlevel practitioners order too many and/or inappropriate exams. Sometimes physicians, too.
Back in 1993 when the ACR Appropriateness Criteria was published I eagerly read many of those sections. It was more than simply what to order, but also relevant findings for individual exams. I gave a lecture to new residents a few years ago about what a great resource it is. I still reference it from time to time. I wish more did.
It certainly is a good guide for clinicians, including Radiologists.
Similarly, predicted to save money, too.
Simply common sense
This highlights the problem….
https://t.co/HR1yMwJeGu
Attention NPs and PAs. “Hi-Resolution Lung CT” isn’t actually any higher resolution than a normal CT and you probably shouldn’t be ordering it unless you work with a pulmonologist.
This is hands down one of the most valuable “tools” I’ve learned.
Saw it about 4-5 years ago.
Rather than theoretical ideas such as investing in the stock market is good financial sense or maxing out your retirement plans, this gives you concrete numbers.
Similarly, as a Radiologist, if imaging volume is increasing 10-15% because of aging baby boomers, you can estimate when your total volume of work may double.
This should be taught to every high school student.
I’ve tried to do likewise for my children.
Few, if any, of my colleagues at work know it, which is why to “enlighten” them.
That, and the concept of Emotional Intelligence, are 2 things that may help determine your likelihood of success?
Certainly a guide IMO.
I benefited from this back around 1980.
Saw him at the Spectrum in Philly
Our seats were back of the floor near soundboard ( didn’t know that when buying them).
Security/ushers told us they were moving our entire section closer.
My girlfriend had gone to the restroom so I had to wait while they moved everyone else.
We ended up 1st row left section on the outside.
Towards the center of our row was Christie Brinkley!
Great seats and great show.
@blogitallnight This is what they should’ve printed for the venue. Would’ve had a long line. I’m going tomorrow night.
Tbh, I’ll pass simply because I collect official merchandise and I have too much stuff already, but kudos. Well done!
Thanks for your concern, Mark!
Unfortunately, it is far more complex than student debt.
I have been in private practice for > 30 years and recent Past President of our State Society.
In that time, I have witnessed how medical care is now mostly controlled by hospitals and corporations. Student debt is not a primary factor. There was a recent paper highlighting why physicians are leaving at a much earlier age and that was not a relevant factor, as well.
Look at this PowerPoint along with that paper, including a good chart listing reasons why physicians are leaving or selling their practices.
A.
https://t.co/azXAVdDU92
B.
https://t.co/y0tSxkcQ4z
Congressman Murphy,
Thank you for sharing my post.
As a fellow physician, I was disappointed by your comments on physicians leaving practice early.
While dedication to the field is essential, blaming those leaving ignores deeper problems.
The practice of medicine has changed dramatically since we graduated—especially post-HITECH and ACA. The recent Permanente Journal study I referenced (May 2026) shows physicians are now exiting clinical practice at an average age of 48 (down from 57 in 2011). Roughly 20% leave within the first five years, with similar losses every five years thereafter. These are outstanding students who endured grueling training; they're not "unmotivated." The field simply isn't what they signed up for.
Data from the Annals of Internal Medicine (link below) also show the annual rate of physicians leaving practice has roughly doubled in recent years, from about 1.6% to 3.1%. Out of a million physicians, that is 30,000 - the equivalent of approximately 200 graduating med school classes lost, every single year.
Additional surveys indicate that a substantial portion plan significant reductions in work or early exit in the coming years. What a tremendous loss of talent and investment.
We can do better. The issues are well known and not the doctors. We’ve lost autonomy - most doctors are now employees with little influence over their practice. We battle insurance prior authorizations, click through EMRs late into the night, and pay for unproven maintenance of certification amid stagnant RVUs.
No one excelled in premed and med school to spend their career fighting the system and archaic EMRs instead of treating patients.
I know your record includes strong support for physicians—Medicare reimbursement protections, reducing regulatory burdens, and highlighting burnout. I urge you to double down on fixing these systemic issues rather than questioning the commitment of those voting with their feet.
And physicians who quit tell only half the story. Many more surveys show that as many as a third of physicians plan to retire in the coming years.
Physicians like you are uniquely positioned to lead.
Don't blame the victims. Let's fix the system.
Respectfully
https://t.co/8vMWQaQpfo 0pubmed
https://t.co/dI6Z0Y3CCV
https://t.co/Gy9lD5kUKr
https://t.co/AP1h3u1Ovg
https://t.co/KkiSqB5fLM
https://t.co/8UOcK5lpdO
Wow.
No disrespect, but that comment is so out of touch.
The loss of independent practices and that autonomy is a far greater concern, with rising burnout leading to earlier retirements.
Similarly, that is a multifactorial problem that needs to be addressed-
https://t.co/azXAVdDU92
@DrDiGiorgio@DrBruggeman@realdocspeaks@EdGainesIII@ACRRAN@RadiologyBiz@MStempniak
@cremieuxrecueil The overwhelming reason for the lack of professional satisfaction is largely related to the change in practice patterns and loss of autonomy.
@DrDiGiorgio
@realdocspeaks This is all you need to know.
It highlights how the hype/promise never met expectations here and abroad
Poorer outcomes and more costly, too.
https://t.co/PqoCRSVlno
@realdocspeaks This is all you need to know.
It highlights how the hype/promise never met expectations here and abroad
Poorer outcomes and more costly, too.
https://t.co/PqoCRSVlno
Nurse Practitioner training programs are exploding, and many of these private equity backed “schools” extort the student for huge sums in exchange for an extremely poor education. We need a “Flexner Report” for NP training in the US! #medtwitter#medicine#physician#medstudent #txlege
@WSJ Here is a more accurate picture.
The hype/promise has never matched the outcome .
Both here and abroad.
Patient care is compromised with increasing costs with full practice authority.
https://t.co/PqoCRSVlno
@realdocspeaks This is all you need to know.
It highlights how the hype/promise never met expectations here and abroad
Poorer outcomes and more costly, too.
https://t.co/PqoCRSVlno