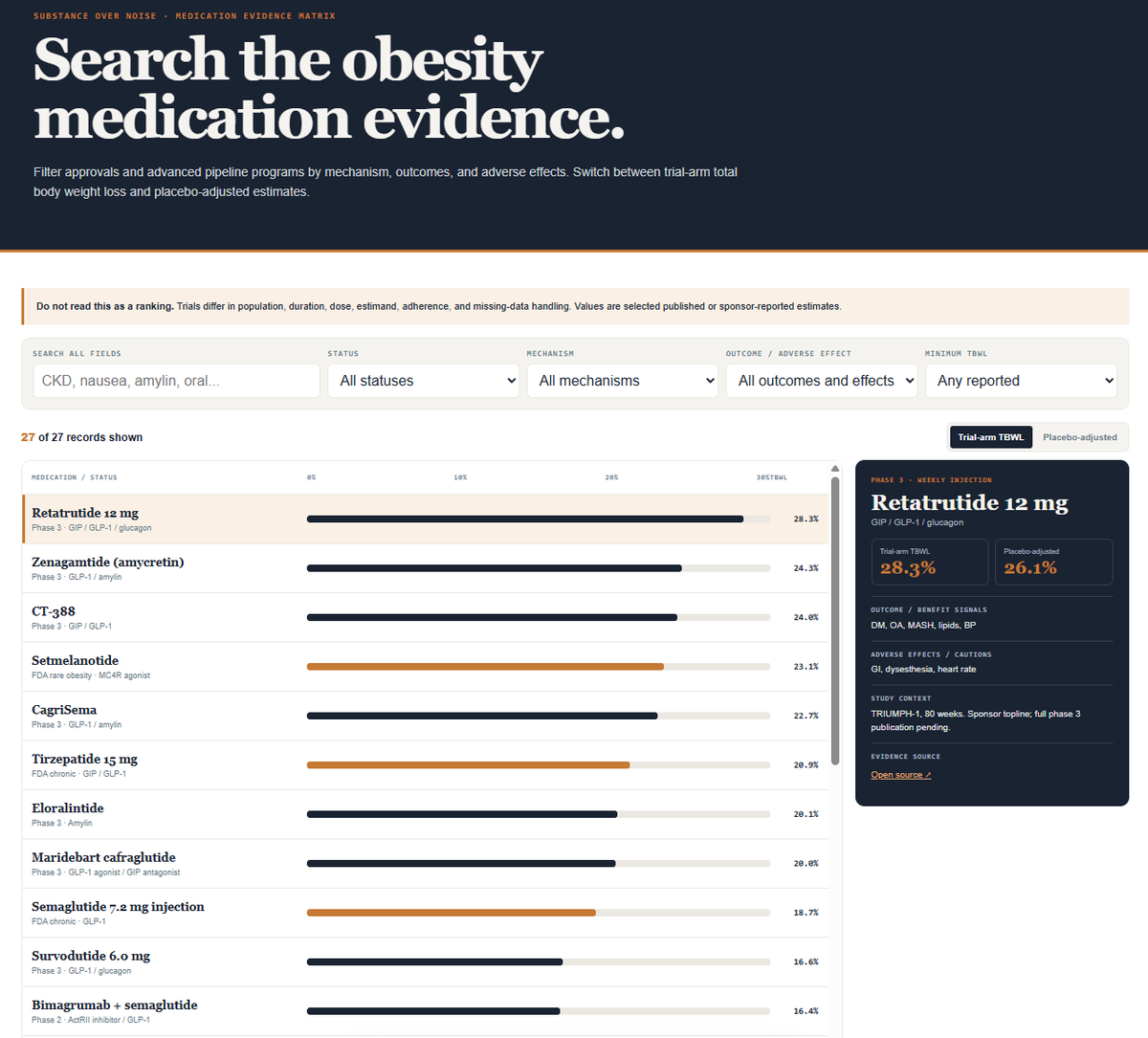
V2 of the obesity trials tracker is live: a real-time https://t.co/pCwIZPJGIW explorer + a ~30-drug weight-loss comparison (trial-arm & placebo-adjusted TBWL, each sourced).
Built for orientation, not ranking. https://t.co/NXmF6AoyoG
Just upgraded the code for the mobile experience of Obesity Trial Tracker. Should improve UX/UI. I'll keep working on it. Please provide feedback if you find it useful. https://t.co/Uc5HllxuPJ
The GLP-1 Bridge Program is so administratively complex. I feel for everyone trying to navigate it right now.
I don't see how any standard busy primary care clinic could participate in it at any scale. The layers of complexity will be a blocker to enrolling eligible patients.
Can you actually reverse heart disease, or just slow it down? Eighteen months after a scan found soft plaque in my arteries, a follow-up suggested it had shrunk by around forty percent, and I wanted to know whether that result could be trusted.
In this episode, I sit down with interventional cardiologist Dr Campbell Rogers to unpack what modern imaging can really see, why a calcium score of zero is not the all-clear, and whether we should be treating plaque rather than chasing a number.
For the full show notes head to: https://t.co/46Kh7zpBpg
Vineyard's goal is to participate in decentralized clinical trials within the next 12–18 months.
If you're an academic clinical trialist considering a career change and are interested in partnering with Grant Tinsley and me to build a new model for obesity research, I'd love to have a conversation.
One group that has received very little attention—but deserves more—is Medicare Part D beneficiaries who qualify for GLP-1 coverage for a non-obesity indication. While they may technically have coverage, many still face copays that can exceed $500 per fill, making treatment financially out of reach for some.
Yes, the Medicare Prescription Payment Plan ("smoothing" or buy now, pay later) can spread those costs over the year, but it doesn't reduce the total amount owed. By comparison, participants in the Bridge program pay no more than $600 per year for their medication, whereas the Inflation Reduction Act caps annual Medicare Part D out-of-pocket prescription drug spending at approximately $2,200. These programs are simply not operating on a level playing field.
As a result, some patients who qualify for Part D coverage are excluded from Bridge solely because they have Medicare drug coverage—even if their actual out-of-pocket costs are substantially higher. In many ways, they have become the group left behind.
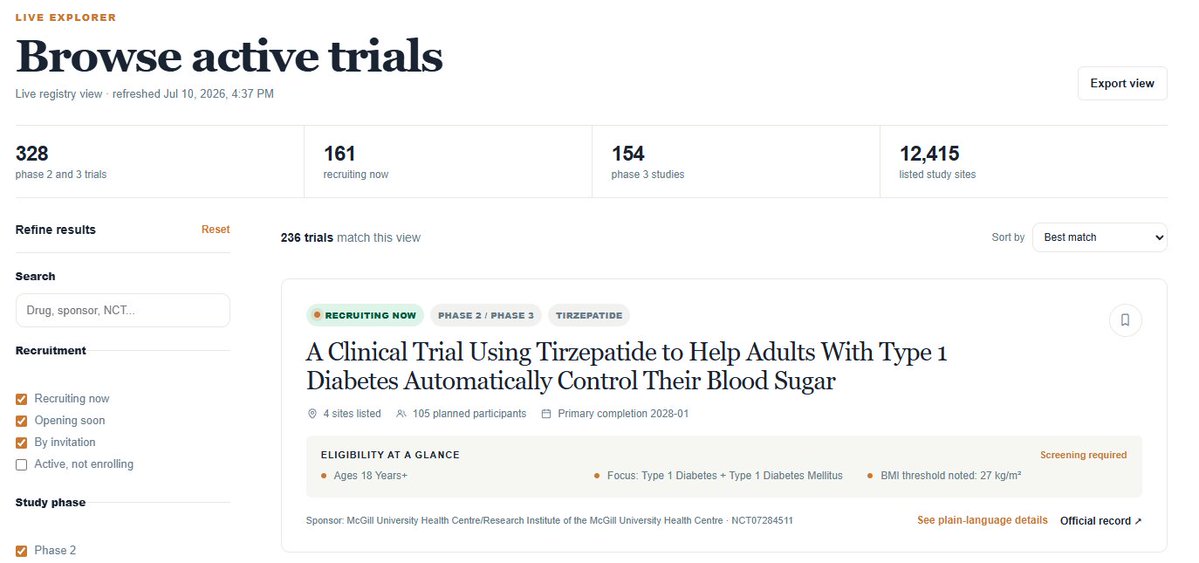
A lot of people have asked how they can keep up with obesity clinical trials, and many are interested in participating.
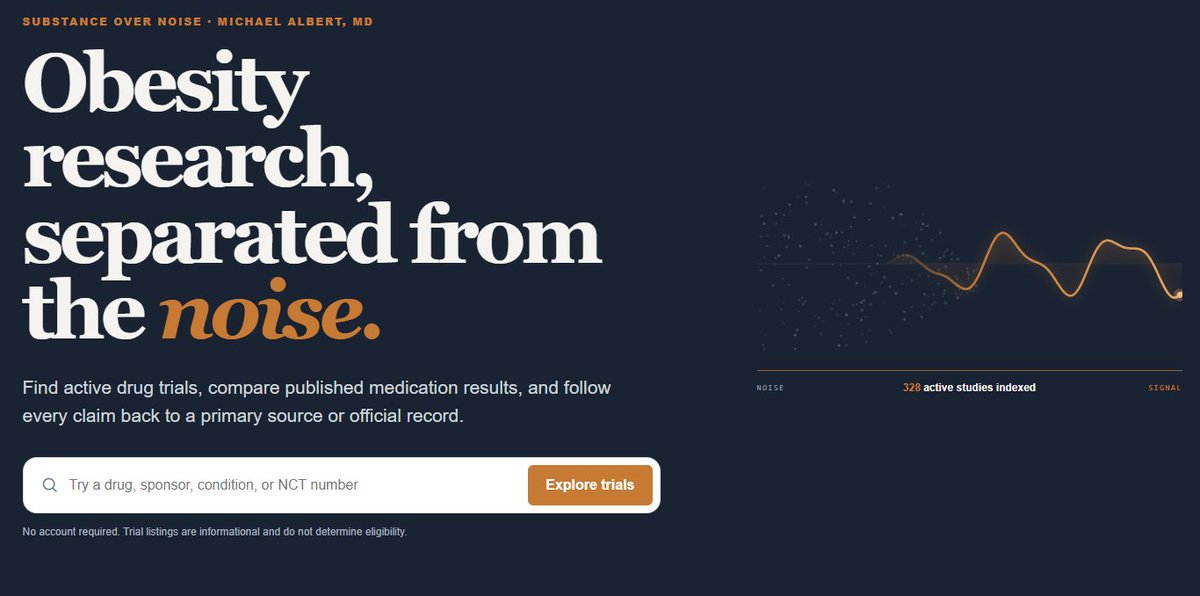
So I built a free, live tracker of active obesity drug trials.
You can explore ongoing studies, see what's recruiting, and learn more here: https://t.co/7dj5bwrwNn
@ZKForTre Nope, and I've voiced that publicly, but the study was designed pre-2021, before we even fully appreciated that circulating drug level predicts response (circa 9/2021).
You had to know I was going to analyze the JAMA Secret GLP1 Shopper Telehealth Study. That breakdown drops this weekend. It's about to get spicy. 🌶️
Be the first to know: https://t.co/ilBUKHFRvA #substanceovernoise
My take on UPFs continues to be:
- there is a need for understanding attributes of foods that influence health beyond classical nutrients, creating metrics around them, and incorporating them into dietary guidance, labeling and regulations. NOVA is a sledgehammer approach to this that has appeal because its an existential cudgel to the industry but is generally unserious as a research tool, let alone a regulatory science tool.
Unfortunately, submitting a grant to NIH to understand the physical and sensory properties of food that impact health isn't sexy enough to land a grant. We've also gutted the research infrastructure needed to do this work, which the pre-2010s research environment wasn't ideal for as is. We continue to splice and dice FFQs in a million ways that won't and can't advance nutrition science and the UPF convo is mostly a swan song for a field charged with addressing major public health crises that its ill-funded to address.