@DrBendary Completely agree Scientific Societies should defend patient interests by using part of the money they receive from Industry to sponsor investigator initiated RCTs
European defence governance and financing https://t.co/aiguKqxdwY # via @cepr_org
Russian aggression, shifting US commitments, global competition over trade, technology, critical minerals, talent, intellectual property create a narrow window
Urgency cannot be over started
🎙️ A Cut Above podcast — The new episode is live now!
Recorded live at the EACTS Annual Meeting, this special episode delves into the theme “Nightmares in CABG.”
Join hosts @FaisalBakaeen, Thomas Gudbjartsson and @Migas2001 for an open and practical discussion on the challenges of coronary surgery.
From fragile conduits and calcified aortas to dissected mammary arteries and “full metal jacket” targets, the panel shares their approaches to complex scenarios, offering valuable insights on preparation, technique and team communication.
The conversation highlights patient assessment, intraoperative decision-making and the humility required to learn from complications. It closes with reflections on mentorship, transparency and the power of honest debriefing in shaping safer surgical practice.
🎥 Watch the full episode here: https://t.co/1wOqguucPr
🎧 Listen to the podcast here: https://t.co/Mz3bWEa06f
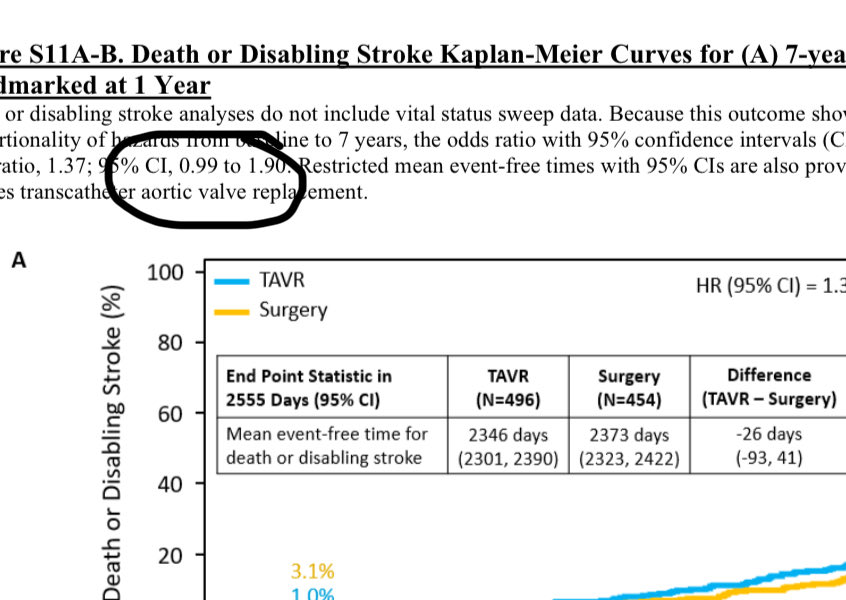
PARTNER 3 at 7 years can be read both ways like a glass half empty or half full However as @kaulcsmv and @drjohnm pointed out HR less appropriate due to non proportionality OR upper bound for death is almost 2x greater for TAVR and seems important in low risk patients
I believe the key issue is this "vital sweep" mentioned in the paper — a term I had never encountered before. Interestingly, the curves you refer to are in the supplementary materials and correspond to the non-sweep analysis. Those in the main paper are less separated and refer to the sweep analysis, in which they retrieved vital status for a substantial number of patients, apparently mostly surgical ones. Of course, if the idea was to let readers choose which set of curves they prefer, it doesn’t seem like a particularly sound approach. In any case, collecting follow-up data beyond five years clearly remains a major challenge.
@DFCapodanno I believe the key issue is the violation of non proportional hazard. When OR is calculated (as occurs when this happens) TAVR has higher risk of stroke or death. This extremely dangerous considering the velocity with which cardiological societies are pushing TAVR to younger pts.
IMPORTANT Hazard ratio for higher death in TAVR arm may be less appropriate due to non-proportional results in years 1-7. As Sanjay writes, the odds ratio of death or disabling stroke at 7 years is 1.37 and upper bound is nearly 2x worse for TAVR. Seems important in low-risk pts
@drjohnm We all know Valve replacement either SAVR or TAVR have >0 hospital risk and just replaces one disease by another plus the risk of endocarditis or pace maker
It is really sad how this type of editorials devoid of any substantial arguments with historically re-known authors aim at influencing and put pressure on guide modification
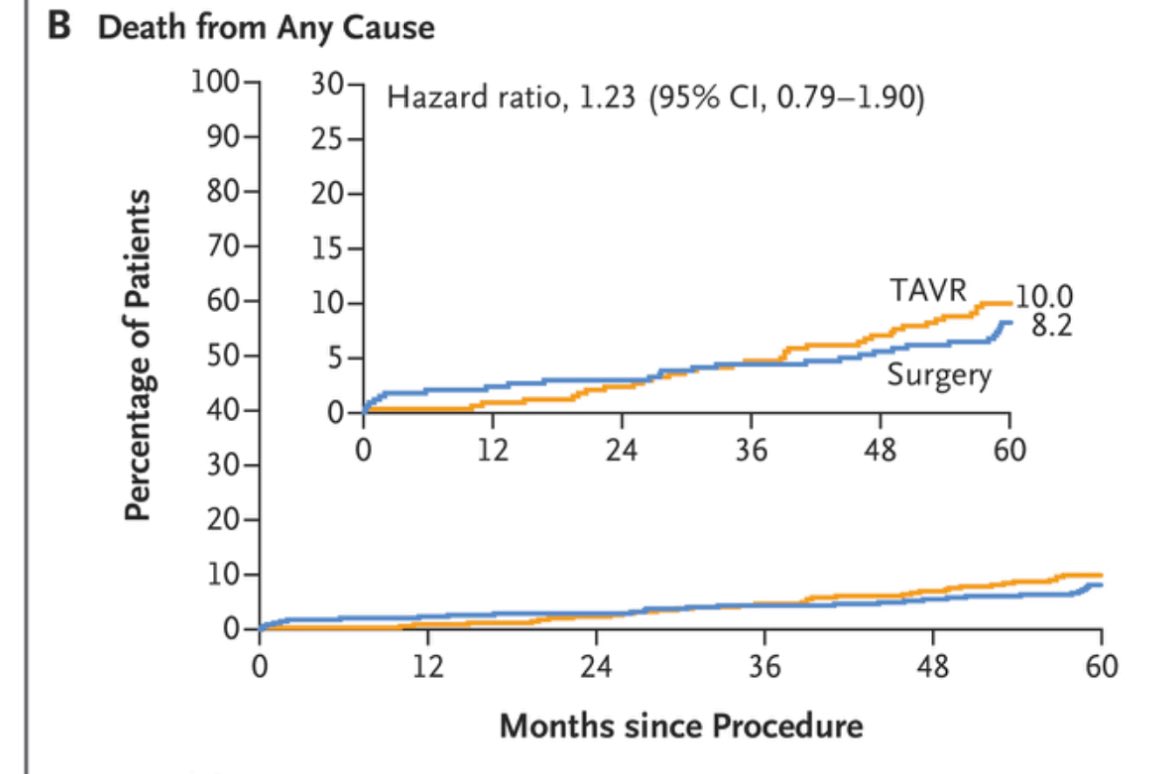
Concerns were raised with the 5 year data of PARTNER 3 regarding mortality (higher with TAVR). The 6 year data posted at the @US_FDA show that curves continue to diverge…..