Every myeloma eventually stops responding to a proteasome inhibitor. Some after years, some after a few months. What you reach for next is half of what we actually do in clinic ?
The Anderson lab's new Blood paper (Du, Fang et al, DFCI) goes somewhere different with that problem. Instead of another 20S inhibitor — bortezomib → carfilzomib → ixazomib → marizomib, two decades of the same engine — they go upstream to the 19S regulatory particle. Specifically PSMD1, the scaffold subunit that lets 19S dock to 20S. At first sounded like yah this would make sense...
The biology is clean:
• PSMD1 overexpressed in MM
• Knockdown → K48 polyubiquitin piles up despite intact 20S catalytic activity — the 26S can't assemble
• ER stress, G0/G1 arrest, caspase 3/9 cleavage, p53-independent
• Active in carfilzomib and bortezomib samples— routes around PI resistance entirely
• Kills CD138+ patient cells, spares CD138-neg cells and healthy PBMCs
The immune piece is the little surprising to me. PSMD1 depletion turns on IFN-α/γ, activates cGAS-STING, flips calreticulin to the surface (immunogenic cell death), and bumps MHC I/II. Patient CD4+/CD8+ T cells activate in coculture. So you're not only killing tumor — you're potentially re-priming the BM at the same time !!
I looked back on what has happened when folks tried targeting - PSMD4 and ADRM1 and both have failed. PSMD1 sits upstream of both — knock it out and PSMD4/ADRM1 fall with it, but not vice versa. The hierarchy explains why the earlier attempts stalled.
Authors explore delivery with LNP-siRNA, same chemistry as patisiran --> in NSG xenograft shows response and synergy wtih Pom.
Interesting thought from my knowledee on LNP; their biodistribution favors liver and BM. We have seen that siRNA durability in heme has been a sticky problem.
Look forward to were it goes next. If you take down the assembly platform of the 26S instead of the catalytic core, you stop chasing 20S mutations and start with a clean resistance slate. The immune activation suggests this could layer with a bispecific rather than compete.
@BloodJournal @JanakiramMurali@bhemato@mpianko @nihrardesai89 @GKaurMD
#Myeloma #mmsm #HemOnc @NikhilMunshiMD@DanaFarber
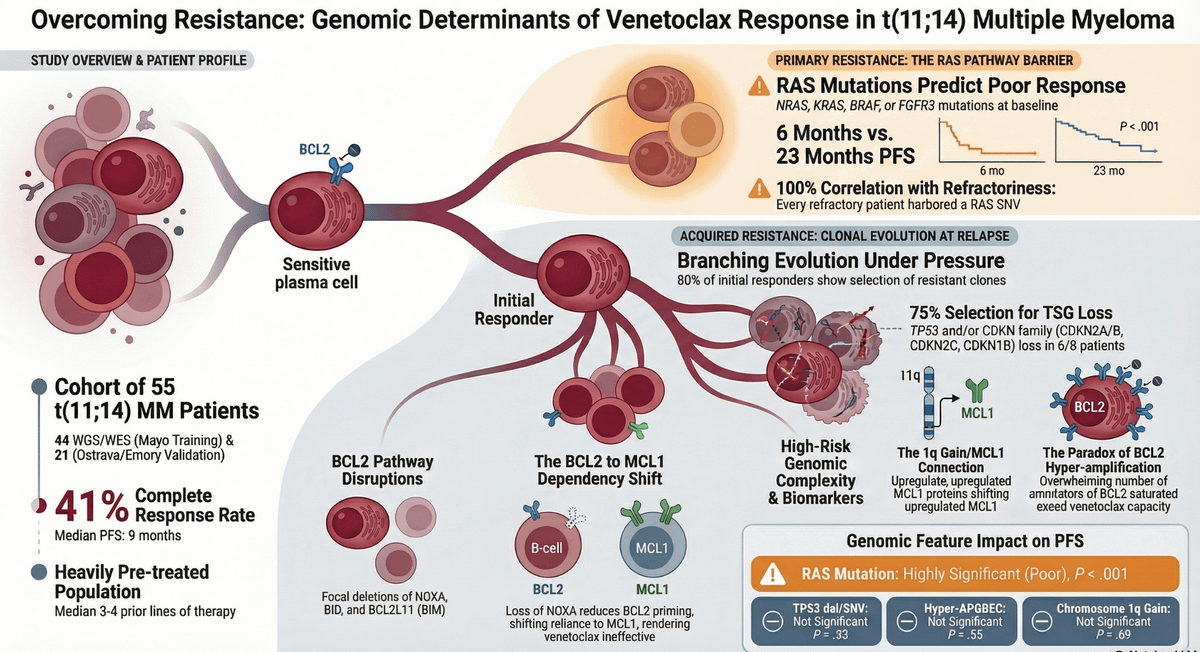
New in Blood (April 2, 2026): "Genomic mechanisms of resistance to venetoclax in t(11;14) myeloma" — Kaddoura, Kumar, Maura, Baughn et al.
We know venetoclax works in t(11;14) myeloma. What we haven't understood well is why some t(11;14) patients don't respond — or respond then progress quickly.
This paper starts to answer that with whole-genome/exome sequencing of 34 patients.
Study link:
https://t.co/hZ9LSxMwNV
⭐🩸 @syed_abutalibmd & @mpianko highlight major advances in T-cell–redirecting therapies for relapsed/refractory #multiplemyeloma from #ASH25: MajesTEC-3, RedirecTT-1, and inMMyCAR
Read their highlights from these featured abstracts ➡️ https://t.co/nXupaR7Bq6
MajesTEC-3 ASH LBA
Best result ever in a RRMM randomized trial. It will transform how we approach myeloma. Congratulations to authors and @JNJNews
https://t.co/UhNOesmjXd
I also don’t use levo prophy… Interestingly, in TEAMM there was a higher proportion of deaths from progressive MM in the levofloxacin group compared with placebo group (73% vs 38%) in the first year of treatment. Was this because levofloxacin initially kept some alive who then died from poorly treatment responsive refractory myeloma, or otherwise caused disruption to the patient’s gut microbiome which may be important for response to MM treatment?
Congratulations to the @Regeneron team. Disappointed we cannot use earlier in the course of the disease. Would gladly use for first relapse in many patients with advanced age. Attrition erodes success.
🩸 Hem/Onc physicians, including community practitioners, fellows & faculty — join us for the Fall 2025 Hematologic Malignancies Symposium at @UMichMedicine!
📅 Sat, Oct 11 | ⏰ 9 AM–3:30 PM
📍 The Kensington Hotel, Ann Arbor, MI
💵 No cost to attend
💡 Focus on myeloma, lymphoma, leukemia & CAR-T
Register: https://t.co/zfUznemQz4
Agenda: https://t.co/H9qWRcfO2Q
#HemOnc #mmsm #Lymphoma #Leukemia #CAR_T #MedEd #UMich @UMRogelCancer@umichFFMI
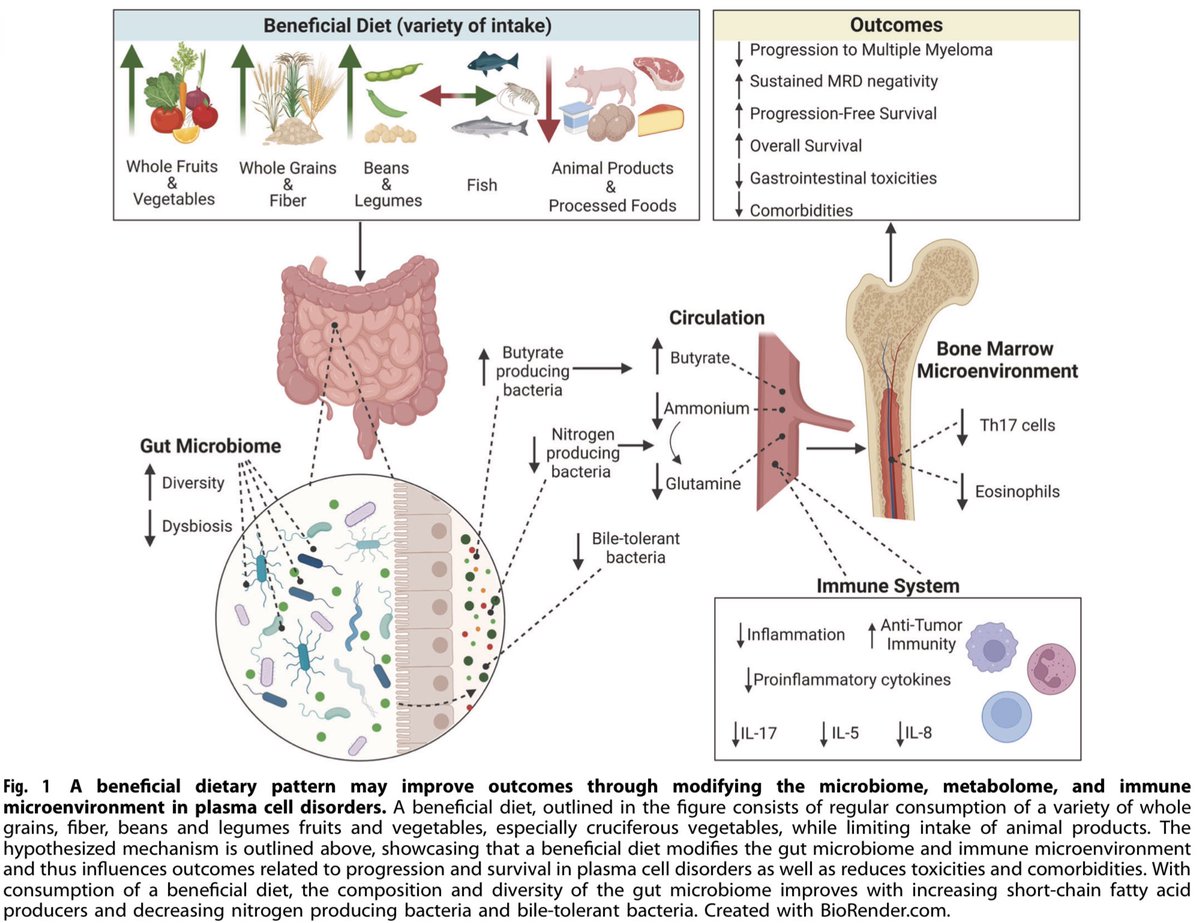
Many oncologists dismiss nutrition as part of a patients overall cancer care plan since they don’t get nutrition training.
I discuss nutrition in oncology with Dr Tracy Cushing and Dr Eden English on their podcast. Hope this episode changes your mind.
https://t.co/YmKnMOBX4U 1/3
Calling all physicians/advanced practice providers seeing pts with multiple myeloma!
We invite you to participate in a quick survey on "Clinician Perspectives on Smoldering Myeloma."
Led by @bdermanmd@rajshekharucms@Eddie_Cliff
Survey link: https://t.co/DrnfYPROjE
#mmsm
@Abdallah81MD https://t.co/i7x2tQDpKi could suggest this method to your pharmacists… how to prepare a stable suspension of thalidomide. Perhaps it could be modified to suit your needs
Update: Someone from BCBSM reached out to us directly to help, which is very appreciated. Since it seems no PA is actually required yet for Tecvayli, Part of the issue here may be related to PA for tocilizumab(Actemra) which is essential for safe management of Tecvayli-related cytokine release syndrome. Getting fast auth for both of these drugs is another important issue for getting tecvayli started in a timely manner
waiting patiently for @BCBSM to approve Teclistamab for my patient in great need of this drug. Apparently ‘urgent’ means a 10-14 day review time. Unreasonable prior authorization times are dangerous and irresponsible. What can be done to stop this madness? #mmsm
waiting patiently for @BCBSM to approve Teclistamab for my patient in great need of this drug. Apparently ‘urgent’ means a 10-14 day review time. Unreasonable prior authorization times are dangerous and irresponsible. What can be done to stop this madness? #mmsm